
Abstract
Background:
Fatty infiltration (FI) of the supraspinatus is commonly seen in chronic large-to-massive rotator cuff tears. Evaluating FI in patients with severe muscle atrophy can be confusing.
Purpose/Hypothesis:
The purpose of this study was to investigate the anatomic relationship between the suprascapular artery and supraspinatus muscle on magnetic resonance imaging (MRI) to provide a method for defining the border of the supraspinatus muscle on Y-view MRI. It was hypothesized that the branches of the suprascapular artery would encircle the supraspinatus muscle on Y-view and adjacent MRI slices and could be used for defining the supraspinatus outline on oblique sagittal images.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 172 shoulders that had undergone arthroscopic repair for large-to-massive rotator cuff tears were retrospectively included. Two methods, one based on the supraspinous fossa and trapezius (SF method) and the other based on the region bounded by the branches of the suprascapular artery (SA method), were used for defining the supraspinatus outline on Y-view MRI for the assessment of FI. Preoperative supraspinatus FI grade and tangent sign and postoperative tendon integrity were evaluated. Shoulder function was assessed using the American Shoulder and Elbow Surgeons (ASES) score and active range of motion.
Results:
The branches of the suprascapular artery encircled the supraspinatus in all shoulders, with the diameter of the branches ranging from 0.5 to 3 mm. The agreement in supraspinatus FI grading between the SF and SA methods was 65.12%. When limited to the 61 shoulders with a positive tangent sign, the agreement dropped to 22.95% (κ = 0.032). The group (FI grade 2 by SA method and ≥3 by SF method) showed no significant difference in postoperative outcomes compared with the 2-vs-2 group but had significantly better postoperative ASES scores (P = .001) and active range of motion in forward elevation (P = .020) compared with the ≥3-vs-≥3 group. The tangent sign was positive in 92.16% of the 2-vs-≥3 group.
Conclusion:
The suprascapular artery is a reliable reference for the evaluation of supraspinatus FI. When a positive tangent sign presents, supraspinatus FI is likely to be overestimated if the hyperintensity outside the region bounded by the branches of the suprascapular artery is mistaken as FI.
Keywords
Fatty infiltration (FI) is commonly seen in chronic large-to-massive rotator cuff tears (RCTs) and is linked to poor outcomes after rotator cuff repairs.9,20,38 FI, fatty degeneration, or fatty atrophy are often used interchangeably in different studies to describe the same process of intramuscular fat accumulation of the rotator cuff, which could occur in both perifascicular and intrafascicular spaces without altering muscle organization.17,18 Dramatic degeneration and inflammation have been found in rotator cuffs with severe FI. 18
Although FI is often accompanied by atrophy in chronic RCTs, atrophy and degeneration are different pathological processes with distinct mechanisms of muscle loss involving different pathways.2,48 Muscle atrophy is a normal response to disuse, which is caused by tenotomy-induced mechanical unloading or inactivity,32,44 and can be nearly reversed by muscle reloading. 12 After RCT, muscle atrophy results in the loss of contractile force from the supraspinatus, but exacerbated weakness is observed with increased FI. 46 The distinction between FI and atrophy has critical implications for therapeutic strategies.
The Goutallier grading system is the method used most commonly for evaluating FI based on computed tomography (CT) or magnetic resonance imaging (MRI).13,21,22 Fuchs et al 13 found that MRI and CT methods had unsatisfactory agreement on FI evaluation. They attributed the discrepancy to the fact that the muscular regions examined were not identical. They also concluded that muscle and fibrous tissue are very difficult to distinguish on CT, whereas connective tissue could not be mistaken for muscle on MRI. As FI is defined as intramuscular fat accumulation and the Goutallier grading system evaluates the proportion of fat in muscle, precisely defining the border of the supraspinatus is crucial. When FI and atrophy exist in the supraspinatus at the same time, however, it may be difficult to identify the muscle border.
The anatomic relationship between the supraspinatus muscle and suprascapular artery may allow for a solution to this issue. The suprascapular artery is one of the branches of the thyrocervical trunk. It runs behind and parallel to the clavicle and subclavius muscle and passes over (or below in some cases) the superior transverse scapular ligament. 41 The artery enters the supraspinous fossa, travels close to the bone, running between the scapula and the supraspinatus muscle, to which it supplies branches. 33 It then passes through the greater scapular notch to reach the infraspinous fossa. However, the anatomy of suprascapular artery on MRI is not well documented.
In this study, we investigated the anatomic relationship between the suprascapular artery and supraspinatus muscle on MRI to provide a method for defining the border of the supraspinatus muscle on Y-view MRI. We hypothesized that the branches of the suprascapular artery would encircle the supraspinatus muscle on Y-view MRI and adjacent slices and could be used for defining the supraspinatus outline on oblique sagittal MRI.
Methods
Study Design
Institutional review board approval for the study protocol was obtained for this study, which was conducted between July 1, 2016, and January 31, 2020. A total of 196 arthroscopic repairs of large-to-massive RCTs (anteroposterior tear size >3 cm) were performed and considered eligible for inclusion.8,16 Other inclusion criteria were patients with a follow-up period of >2 years and complete sets of preoperative and 1-year postoperative MRI scans. The exclusion criteria were patients with (1) partial tears or small- to medium-sized tears, (2) open repair or tendon transfer surgery, (3) surgical history of the same shoulder, and (4) incomplete follow-up data.
Surgical Technique and Rehabilitation
All patients underwent arthroscopic repair of RCTs performed by a single surgeon (C.J.). Patients were placed in the lateral decubitus position with the arm in traction. The tear margin was debrided to gain better access to tendon tissues. We also performed 270° capsular release, complete rotator interval release, subacromial release, and comprehensive bursectomy as needed. The transosseous-equivalent suture-bridge technique was used for repair (SwiveLock anchor [Arthrex] and Healix anchor [DePuy-Synthes]) if the medial edge of the tear could be pulled to cover 50% of the footprint without undue tension; otherwise, the single-row technique was used. Biceps tenotomy or tenodesis was performed in all patients.
Postoperatively, immobilization with an abduction pillow after surgery was maintained for 6 weeks. Passive range of motion (ROM) exercises were started 3 weeks after surgery. Active ROM (aROM) exercises and daily activities were not allowed until 6 weeks postoperatively. Muscle strengthening exercises were started 6 months after the surgery. All rehabilitation procedures were supervised by the same group of physical therapists.
MRI Evaluation
Preoperative MRI was used for evaluating the suprascapular artery, supraspinatus FI, and atrophy. One-year postoperative MRI was used for evaluating tendon integrity.
The suprascapular artery was identified on the Y-view and adjacent oblique sagittal slices of T1-weighted (T1-wt) image (repetition time/echo time: 480/15 ms, slice thickness: 2.6 mm; flip angle: 110°; imaging matrix: 392 × 408) and fat-suppressed T2-weighted (FS-T2-wt) MRI (repetition time/echo time: 2600/35 ms, slice thickness: 2.6 mm; flip angle: 110°; imaging matrix: 392 × 408). In this study, the Y-view was defined as the most lateral oblique sagittal image in which the scapular spine is in contact with the scapular body (Figure 1, B and E). The oblique sagittal slices just medial and lateral to the Y-view were defined as the medial Y-view (Figure 1, A and D) and lateral Y-view (Figure 1, C and F), respectively.

Identification of suprascapular artery on oblique sagittal MRI slices of a left shoulder. Fat-suppressed T2-wt images: (A) medial Y-view, (B) Y-view, and (C) lateral Y-view. T1-wt images: (D) medial Y-view, (E) Y-view, and (F) lateral Y-view. *Suprascapular artery; †clavicle. MRI, magnetic resonance imaging; T1-wt, T1-weighted; T2-wt, T2-weighted.
As described in a previous study, 33 the suprascapular artery was confirmed on MRI to (1) travel parallel with the clavicle (Figure 1, A,B,D and E), (2) run between the scapula and the supraspinatus muscle (Figure 1, A-F), and (3) pass through the greater scapular notch to reach the infraspinous fossa (Figure 1, C and F). After identification of the suprascapular artery, we recorded whether the branches of suprascapular artery encircled the supraspinatus muscle. The diameter of the branches of suprascapular artery was measured on T1-wt MRI and was compared with the reported diameter of the arch arterioles of the supraspinatus tendon, which is about 25 μm. 33
Two methods were used to define the supraspinatus muscle outline on Y-view T1-wt images. The first method took the region bounded by the supraspinous fossa and trapezius as the supraspinatus muscle outline and was labeled the supraspinous fossa method (SF method) (Figure 2B). The second method took the region bounded by the branches of the suprascapular artery as supraspinatus muscle outline and was labeled the suprascapular artery method (SA method) (Figure 2C). When the suprascapular artery was difficult to identify on Y-view T1-wt MRI, the Y-view and adjacent slices of FS-T2-wt MRI were used (Figure 2, D-F).

Oblique sagittal MRI slices of a left shoulder. (A) Y-view T1-wt image. (B) Supraspinatus muscle border defined by the supraspinous fossa method, suggesting Goutallier grade ≥3. (C) Supraspinatus muscle border defined by the suprascapular artery method, suggesting Goutallier grade 2. (D-F) The Y-view and adjacent fat-suppressed T2-wt slices were used to reveal the branches of the suprascapular artery (asterisks). MRI, magnetic resonance imaging; T1-wt, T1-weighted; T2-wt, T2-weighted.
Imaging Outcomes
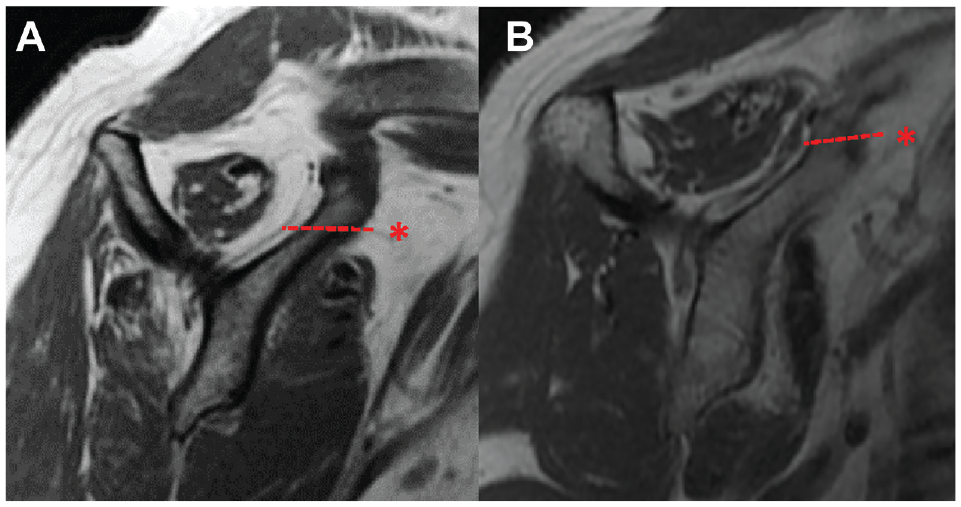
The FI of the supraspinatus was evaluated using the Goutallier classification.21,22 The 3-grade (≤1, 2, and ≥3) classification suggested by Fuchs et al 13 was used; for each shoulder, the supraspinatus FI grades for the SF and SA methods were recorded separately for further statistical analysis. Supraspinatus atrophy was evaluated using the tangent sign as described by Zanetti et al 50 (Figure 3). Postoperative tendon integrity was evaluated using the classification described by Sugaya et al. 43 Tendons classified as Sugaya types 4 or 5 were considered retears.

(A) Negative tangent sign and (B) positive tangent sign in a left shoulder. The dotted line indicates the tangent.
Clinical Evaluation and Outcomes
The patients were evaluated preoperatively and postoperatively at 6 weeks, 3 months, 6 months, 1 year, and every year thereafter until the final follow-up. aROM including forward elevation, external rotation at the side, and internal rotation was recorded. The aROM for internal rotation was recorded as the mean vertebral level the patient could reach with the hand behind the back, with the highest and lowest levels also recorded. Shoulder function and pain were assessed using the American Shoulder and Elbow Surgeons (ASES) score.
Statistical Analysis
The ASES scores and aROM in forward elevation and external rotation were recorded as means and standard deviations. The independent t test or Mann-Whitney U test was used to analyze continuous variables, and the chi-square test or Fisher exact test was used for categorical variables. The paired t test was used to compare the preoperative and postoperative ASES scores and aROM for forward elevation and external rotation, and the Mann-Whitney U test was used to compare the preoperative and postoperative aROM for internal rotation.
The kappa value was calculated to assess the agreement between the SF and SA methods for evaluating supraspinatus FI. In addition, we conducted a subgroup analysis of the clinical and imaging outcomes for the shoulders that showed disagreement in FI grading between the 2 muscle outline methods.
All statistical analyses were performed using SPSS for Windows (Version 22; SPSS Inc). All statistical tests were 2-tailed, and a P value of <.05 was considered statistically significant.
Results
Patient Characteristics and Clinical Outcomes
Among the 196 arthroscopic repairs of large-to-massive RCTs eligible for inclusion, 24 shoulders were excluded because of loss to follow-up (n = 13) and incomplete sets of images (n = 11). The final study group consisted of 172 shoulders, with a mean age at surgery of 59.26 ± 8.58 years and a mean follow-up period of 27.85 ± 8.67 months. Complete repairs were performed in 156 shoulders, of which 29 shoulders (18.59%) had a retear. Partial repairs were performed in 16 shoulders. The other characteristics are summarized in Table 1. All shoulders showed significant improvement in ASES score and aROM from preoperatively to last follow-up (P < .001 for all) (Table 1).
Patient Characteristics and Clinical Outcomes (N = 172 Shoulders) a

Data are presented as mean ± SD or No. of shoulders unless otherwise indicated. Boldface P values indicate statistically significant difference between times (P < .05). aROM, active range of motion; ASES, American Shoulder and Elbow Surgeons.
aROM for internal rotation was recorded as mean vertebral level (highest level-lowest level).
Characteristics of the Suprascapular Artery on MRI
The branches of the suprascapular artery were confirmed to encircle the supraspinatus muscle on Y-view and adjacent slices in all shoulders. When supraspinatus atrophy was absent or lacking, the branches of the suprascapular artery almost fully filled the space between the supraspinatus muscle and surrounding musculoskeletal structures (ie, the scapula and trapezius) (Figure 4). When supraspinatus atrophy and FI were present, the space between the supraspinatus muscle and surrouonding musculoskeletal structures became enlarged. On the Y-view of the T1-wt image, the branches of the suprascapular artery, which showed a similar hypointense signal to that of the supraspinatus muscle, could be mistaken for part of the muscle (Figure 5).

Branches of the suprascapular artery encircle the supraspinatus muscle on oblique sagittal MRI slices of a right shoulder. (A) Y-view, T1-wt image. (B) Medial Y-view, T1-wt image. (C) Y-view, fat-suppressed T2-wt image. (D) Medial Y-view, fat-suppressed T2-wt image. *Suprascapular artery. MRI, magnetic resonance imaging; T1-wt, T1-weighted; T2-wt, T2-weighted.

Branches of the suprascapular artery could be mistaken for part of the supraspinatus muscle. (A-C) Y-views of T1-wt MRI scans from 3 different patients. (D-F) Y-views of fat-suppressed T2-wt MRI scans from the same 3 patients as shown in (A-C), respectively. *Suprascapular artery. MRI, magnetic resonance imaging; T1-wt, T1-weighted; T2-wt, T2-weighted.
The branches of the suprascapular artery were also confirmed to encircle the supraspinatus muscle on axial MRI slices (Figure 6). The diameter of the branches of the suprascapular artery on T1-wt images ranged from 0.5 to 3 mm (Figure 7), which was much larger than that of the arch arterioles of the supraspinatus tendon (25 μm). 33

Branches of suprascapular artery encircle the supraspinatus muscle on axial MRI slices of a left shoulder. (A) Y-view T1-wt image, (B) Y-view fat-suppressed T2-wt image, (C-F) axial slices, fat-suppressed T2-wt images. *Suprascapular artery; †clavicle; ‡supraspinatus muscle. MRI, magnetic resonance imaging; T1-wt, T1-weighted; T2-wt, T2-weighted.
Diameter of the branches of suprascapular artery on T1-wt MRI scans. (A) The diameter of the indicated artery was about 0.5 mm. (B) The diameter of the indicated artery was about 3 mm. *Suprascapular artery. MRI, magnetic resonance imaging; T1-wt, T1-weighted.
Evaluation of Supraspinatus FI According to Muscle Outline Method
The supraspinatus FI grading between the SF and SA methods is shown in Table 2. The agreement between the methods was 65.12% (112/172). When limited to the 111 shoulders with negative tangent sign (ie, no atrophy), the agreement increased to 88.29% (98/111). However, when limited to the 61 shoulders with positive tangent sign, the agreement between the 2 methods dropped to 22.95% (14/61), with a kappa value of 0.032, which suggested poor agreement between the 2 methods. Supraspinatus FI was very likely to be judged as Goutallier grade ≥3 (86.89%) by the SF method and as grade 2 by the SA method (90.16%) (Table 3).
Supraspinatus FI Evaluated Based on Different Muscle Outline Methods a

Data presented as No. of shoulders. FI, fatty infiltration; SA, suprascapular artery; SF, supraspinous fossa.
Supraspinatus FI Evaluated Based on Different Muscle Outline Methods for Shoulders With Supraspinatus Atrophy (n = 61) a

Data presented as No. of shoulders. FI, fatty infiltration; SA, suprascapular artery; SF, supraspinous fossa.
Subgroup Analysis Based on Disagreement in Supraspinatus FI Grading
Disagreement between the SF and SA methods occurred in 60 shoulders. The majority of disagreement (85.00%; 51/60) lay between shoulders with a Goutallier grade of 2 by the SA method and ≥3 by the SF method (2-vs-≥3 group), while the minority (15.00%; 9/60) lay between grades ≤1 by the SA method and 2 by the SF method (≤1-vs-2 group) (Figure 8). The outcomes from these disagreement groups were compared with the outcomes for which agreement in grades was found (the ≥3-vs-≥3, 2-vs-2, and ≤1-vs-≤1 groups).

(A) Distribution of Goutallier grades evaluated by the SF and SA methods. (B-G) Y-view T1-wt MRI scans (top) and Y-view fat-suppressed T2-wt MRI scans (bottom) of different Goutallier grades of the same shoulder in the same position: (B and E) grade ≥3; (C and F) disagree, grades 2 vs ≥3; (D and G) grade 2. MRI, magnetic resonance imaging; SA, suprascapular artery; SF, supraspinous fossa; T1-wt, T1-weighted; T2-wt, T2-weighted.
The 2-vs-≥3 group had significantly better ASES scores (P = .001) and aROM for forward elevation (P = .020) at last follow-up compared with the ≥3-vs-≥3 group, with no significant differences in terms of final supraspinatus continuity, ASES scores or aROM compared with the 2-vs-2 group (Table 4). There were no significant differences in final postoperative clinical or imaging outcomes between the ≤1-vs-2 group and either the 2-vs-2 group or ≤1-vs-≤1 group (Table 5). A positive tangent sign was found in 92.16% (47/51) of shoulders in the 2-vs-≥3 group. In the 4 shoulders without a positive tangent sign, apparent atrophy could also be observed. The tangent sign was negative for all shoulders in the ≤1-vs-2 group.
Clinical and Imaging Outcomes of Shoulders With Disagreement in Goutallier Grading: 2 or ≥3 a

Data are presented as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). aROM, active range of motion; ASES, American Shoulder and Elbow Surgeons.
aROM for internal rotation was recorded as mean vertebral level (highest level-lowest level).
Clinical and Imaging Outcomes of Shoulders With Disagreement in Goutallier Grading: ≤1 or 2 a

Data are presented as mean ± SD unless otherwise indicated. Boldface P value indicates statistically significant difference between groups (P < .05). aROM, active range of motion; ASES, American Shoulder and Elbow Surgeons.
aROM for internal rotation was recorded as mean vertebral level (highest level-lowest level).
Discussion
In support of our hypothesis, the suprascapular artery was able to be used to define the outline of the supraspinatus. As previous studies have described,33,41 the suprascapular artery was confirmed on MRI to travel parallel with the clavicle, run between the scapula and the supraspinatus muscle, and pass through the greater scapular notch. This finding indicated that the suprascapular artery is a reliable landmark on MRI. In addition, the branches of the suprascapular artery were found to encircle the supraspinatus muscles on MRI Y-view and adjacent slices in all 172 study shoulders. The Y-view is also the most commonly used slice for evaluation of FI. ‡ These features ensured that the supraspinatus outline defined by the SA method could be used for evaluating FI without switching slices. The diameter of the branches of the suprascapular artery was found to be from approximately 0.5 to 3 mm, larger than that of the arch arterioles of the supraspinatus tendon (25 μm) as measured by scanning electron microscopy. 33 This suggested that the branches of the suprascapular artery recognizable on MRI were not in the supraspinatus muscle. The region outside the circle formed by the branches of the suprascapular artery also had no reason to be considered as intramuscular.
The supraspinatus muscle has been described as fusiform, bipennate, multipennate, or circumpennate.25,42 However, the supraspinatus was proven to have a more complex architecture, which could be divided into anterior and posterior portions, and the structural differences might lead to functional differences between the anterior and posterior portions.15,42,47 Using histologic analysis in an ovine model, Meyer et al 36 noted that the FI process starts with an increase in the pennation angle (Figure 9), which separates the muscle fiber bundles mechanically. Infiltrating fat cells fill the created space between the reoriented muscle fibers without affecting the structural properties of the muscle cells. The pennation angle increase along with muscle atrophy and FI was also confirmed in cadaveric shoulders with RCTs. 45 FI was therefore not seen as a degenerative process but a necessary rearrangement of the tissue after macroarchitectural changes caused by musculotendinous retraction. However, Gibbons et al 18 reported in 2017 that dramatic degeneration and inflammation of the rotator cuff muscles were characteristics of the most chronic and severe rotator cuff disease states, suggesting that muscle loss is more complicated than, and distinct from, the simple atrophy found in less severe cases.

Illustration showing the supraspinatus muscle, suprascapular artery, and relevant structures.
Despite the controversy about the essence of FI, it has been uniformly described as intramuscular fat accumulation, which excludes perimuscular adipose tissue.17,18 The superficial aspects of the supraspinatus tendon are covered by a thick sheet of connective tissue that contains fibrous tissue and adipose tissue (Figure 9). We suspect the hyperintensity surrounding the branches of the suprascapular artery on T1-wt MRI (Figures 1-8) mainly reflects the connective tissue covering supraspinatus muscle, which should not be mistaken as FI. The supraspinous fossa is supported by the bony structures of the scapula and does not collapse even when severe supraspinatus atrophy occurs, which may explain the enlarged hyperintensity surrounding atrophic supraspinatus muscle. Intermuscular adipose tissue increase, which results from reduced physical activity, 34 and retraction of the supraspinatus tendon may also contribute to the enlarged hyperintensity surrounding the atrophic supraspinatus muscle.14,31
In the current study, the occurrence rate of supraspinatus Goutallier grade ≥3 FI was 34.30% by the SF method and 4.65% by the SA method. The reported occurrence rate of supraspinatus Goutallier grade ≥3 FI in large-to-massive RCTs has varied tremendously in studies, ranging from 4.08% to 96.2%.4,10,23,27,28 Although this discrepancy in the occurrence rate might be a result of the diverse inclusion criteria, the different ways of defining the supraspinatus border might also be an explanation. To our knowledge, no studies have described their methods for defining the supraspinatus border on MRI Y-view when evaluating FI. Only a few studies have provided example figures of supraspinatus Goutallier grade 3 or 4.27,29,35 Although the methods for defining the supraspinatus outline were not described in these studies, some of the examples given were classified only as Goutallier grade 2 by the SA method used in this study. It is possible that the current studies claiming Goutallier grade 3 or 4 FI of the supraspinatus may actually indicate heterogeneous extent of FI and atrophy. Thus, describing the method for defining the muscle outline when evaluating supraspinatus FI is recommended for future studies.
Regarding disagreement in supraspinatus Goutallier grading between the muscle outline methods, the frequency of the 2-vs-≥3 group (n = 51) was more than one-fourth of the total study group (N = 172) and more than 6 times that of the agreement ≥3-vs-≥3 group (n = 8). These 2-vs-≥3 group shoulders functionally resembled the shoulders with Goutallier grade 2, and all showed apparent supraspinatus atrophy. The supraspinatus Goutallier classifications were likely to be overestimated as grade ≥3 by the SF method for these shoulders. When supraspinatus atrophy is apparent, usually with a positive tangent sign, the hyperintense area outside the region bounded by the suprascapular artery is large and may be a source of overestimation. Thus, apparent atrophy without severe FI may be considered as the main characteristic of these shoulders.
Although FI is often accompanied by atrophy in chronic RCTs, the distinction between FI and atrophy is still of clinical relevance. Muscle atrophy is primarily the result of mechanical unloading, which can occur via tendon failure, bed rest, casting, limb suspension, or otherwise decreased voluntary muscle activation.1,3,7,19,40 Surgical repair and physical exercise can reload the muscle and restore the function. 12 Conversely, FI is believed to be irreversible with merely surgical repair 17 and may benefit from possible anti-inflammatory and/or promyogenic therapy. 18 Moreover, FI is sometimes considered one of the indications for alternative treatments for large-to-massive RCTs, such as lower trapezius or latissimus dorsi transfer.11,37 Thus, the precise evaluation of FI has critical implications for therapeutic strategies.
Limitations
This study had some limitations. First, it was a retrospective study. Second, patients with inadequate imaging results or follow-up times were excluded, which could have led to selection bias. And finally, as only a few shoulders were classified as Goutallier grade ≥3 by the SA method, some of the statistical analysis might have been underpowered.
Conclusion
The study results indicated that the suprascapular artery could be used as a reliable reference for evaluation of supraspinatus FI. When a positive tangent sign presents, supraspinatus FI is likely to be overestimated if the hyperintensity outside the region bounded by the branches of the suprascapular artery is mistaken as FI. Awareness of the suprascapular artery could help to precisely define the supraspinatus border, avoiding the mistaking of connective tissue and branches of the suprascapular artery for muscle.
Footnotes
Final revision submitted January 22, 2024; accepted February 26, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by a grant from the National Natural Science Foundation of China (general program, 82172513, to C.J.). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital (ref No. JST202104-19).