
Abstract
Background:
Fatty infiltration (FI) or atrophy alone has been found to be inaccurate in predicting shoulder function after repair of large-to-massive rotator cuff tears (L/MRCTs), especially when a diverse extent of FI and atrophy presents in multiple rotator cuff muscles.
Purpose/Hypothesis:
The Posterosuperior Tetralogy Scoring System (PS-Tetra Score), which integrates FI and atrophy, was proposed to predict shoulder function after surgery. It was hypothesized was that a PS-Tetra Score ≥3 would be a risk factor for poor shoulder function after repair of posterosuperior L/MRCTs and would possess greater diagnostic value than using isolated FI or atrophy of the supraspinatus (SSP) or infraspinatus (ISP).
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 187 arthroscopic repairs of posterosuperior L/MRCTs were reviewed. Magnetic resonance imaging evaluations were performed of FI and atrophy of the SSP and ISP, teres minor hypertrophy, tendon retraction, and acromiohumeral distance. A postoperative American Shoulder and Elbow Surgeons (ASES) score of 70 was used to subgroup patients according to shoulder function. Univariate and multivariate analyses were performed to determine the risk factors of poor shoulder function (ASES ≤70). The diagnostic values of different indicators for predicting shoulder function were evaluated.
Results:
In univariate analysis, female sex, higher Goutallier grade of the SSP and ISP, positive SSP tangent sign, and PS-Tetra Score ≥3 was significantly associated with ASES score ≤70, whereas in binary logistic regression analysis, a PS-Tetra Score ≥3 was the only significant risk factor for poor shoulder function. The occurrence rate of poor function in shoulders with a PS-Tetra Score of 0, 1, 2, 3, and 4 was 0% (0/52), 0% (0/52), 19.57% (9/46), 58.06% (18/31), and 83.33% (5/6), respectively. PS-Tetra Score ≥3 possessed higher crude agreement (87.70%), specificity (90.97%), positive predictive value (62.16%), and area under the receiver operating characteristic curve (0.814) than the other 3 indicators, with relatively high negative predictive value (94.00%) and moderate sensitivity (71.88%).
Conclusion:
PS-Tetra Score ≥3 was a risk factor of poor shoulder function after repair of posterosuperior L/MRCTs and possessed greater diagnostic value than using isolated FI or atrophy of SSP or ISP alone for predicting shoulder function.
Fatty infiltration (FI) and atrophy of rotator cuff muscles on magnetic resonance imaging (MRI) are considered to be associated with poorer shoulder function or retear after repair of large-to-massive rotator cuff tears (RCTs) (L/MRCTs) in many studies.4,11,21,23,29,30 However, there is no consensus on whether FI and atrophy of rotator cuff could predict shoulder function.1,2,11,20,23,26,30,35 The discordance or lack of cutoff values for Goutallier grade further contribute to the inconvenience of using FI as a predictor for postoperative functional outcomes. Some studies have emphasized the importance of defining FI as Goutallier grade ≥3 in RCTs,4,19 some studies have used a cutoff value of Goutallier grade 2 for analysis,11,17 whereas other studies have not mentioned a cut-off value.2,6,18,24,29,32,33
Muscle atrophy of the rotator cuff has usually been evaluated on MRI scans by the tangent sign or occupational ratio.15,36 Although atrophy has been related to poor functional outcomes after repair of L/MRCTs, 11 few studies have reported on the accuracy of predicting postoperative shoulder function using atrophy.
MRCTs of multiple tendons with Goutallier grade ≥3 FI have a high risk for severe functional impairment such as pseudoparalysis. 4 Some patients with posterosuperior L/MRCTs with Goutallier grade of 2 or 3 in multiple muscles have ended with moderate, mild, or no apparent shoulder dysfunction. It was difficult to distinguish similar patients with possibly diverse outcomes by merely using Goutallier classification.
We have proposed a new tool, the Posterosuperior Tetralogy Scoring System (PS-Tetra Score), to predict shoulder function on an MRI scan after repair of posterosuperior L/MRCTs. The PS-Tetra Score ranges from 0 to 4, with each point representing 1 status (FI or atrophy) existing in 1 muscle (supraspinatus [SSP] or infraspinatus [ISP]). We hypothesized that a PS-Tetra Score ≥3 would be a risk factor for poor shoulder function after repair of posterosuperior L/MRCTs and that it would possess greater predictive value than using FI or atrophy alone for predicting shoulder function.
Methods
Study Design
The study protocol received institutional review board approval. A retrospective case-control study was performed in which all patients who underwent arthroscopic rotator cuff repair (RCR) at a single institution from October 1, 2015, to June 30, 2019, were eligible for inclusion. Inclusion criteria were posterosuperior L/MRCT patients (anteroposterior tear size >3 cm) who (1) underwent arthroscopic RCR, (2) had intact subscapularis (SUB) or repairable partial SUB tears (Lafosse type 1 or 2), 22 (3) had a follow-up period >2 years, (4) had complete sets of preoperative and postoperative 1-year MRI scans, and (5) had Hamada grade ≤2.3,9 Exclusion criteria were (1) partial tears or small- to medium-sized tears; (2) SUB tears of Lafosse type ≥3; (3) patients who underwent open repair or tendon transfer surgery; (4) patients with surgical history of the same shoulder; and (5) incomplete follow-up data.
Surgical Technique
All patients underwent arthroscopic repair of RCTs. All surgical procedures were performed by 3 surgeons (C.J., Y.L., and Y.Z.). Patients were placed in the beach-chair position or lateral decubitus position with traction of the arm. The margin of the tear was debrided to gain better access to the tendon tissues. A 270° capsular release, complete rotator interval release, and subacromial release and comprehensive bursectomy was performed. The transosseous-equivalent suture-bridge technique was used for repair (SwiveLock [Arthrex] and Healix [Depuy-Synthes]) if the medial edge of the tear could be pulled to cover 50% of the area of the footprint without undue tension. Otherwise, the single-row technique was used. Biceps tenotomy or tenodesis was performed in all patients. Acromioplasty was performed in all cases. Distal clavicle excision was not performed in any of the included cases.
Postoperative Rehabilitation
Immobilization with an abduction pillow after surgery was maintained for 6 weeks. Passive range of motion (ROM) exercises were started at 3 weeks after surgery. Active ROM exercises and daily activity were not allowed until 6 weeks postoperatively. Muscle strengthening exercises were started at 6 months after surgery. All rehabilitation was supervised by the same therapist group.
Clinical Evaluation
The patients were evaluated preoperatively; at 6 weeks, 3 months, 6 months, and 1 year; and every year postoperatively until the final follow-up. Active ROM including forward elevation, external rotation at side, and internal rotation was recorded. Shoulder function and pain were assessed with American Shoulder and Elbow Surgeons (ASES) scores. Patients with a postoperative ASES score ≤70 at final follow-up were considered to have poor shoulder function. 31
MRI Scan Evaluation
Preoperative and 1-year postoperative MRI was routinely performed, with an additional MRI scan performed during follow-up when retear was suspected. The final diagnosis of retear was determined by an independent radiologist who was blinded to this study.
All MRI scan evaluations were performed on 1-year postoperative images. FI, atrophy, and teres minor (TM) hypertrophy were measured on the most lateral oblique sagittal image in which the scapular spine was in contact with the scapular body (Y-view). FI was evaluated using the Goutallier classification.12,13 The 3-grade (0+1, 2, 3+4) classification suggested by Fuchs et al 7 was used for further evaluation and statistical analysis (Figure 1). SSP atrophy was evaluated with the tangent sign as described by Zanetti et al. 36 ISP atrophy and TM hypertrophy were evaluated using the occupational ratio. The areas of the ISP, TM, and anatomic external rotation (a-ER) muscles were measured using ImageJ software (National Institutes of Health). The occupational ratios of the ISP and TM were calculated as the area of the respective muscle divided by the area of the a-ER muscle. ISP muscles with an occupational ratio <0.586 were defined as atrophic, and TM muscles with an occupational ratio >0.288 were defined as hypertrophic (Figure 2).15,16
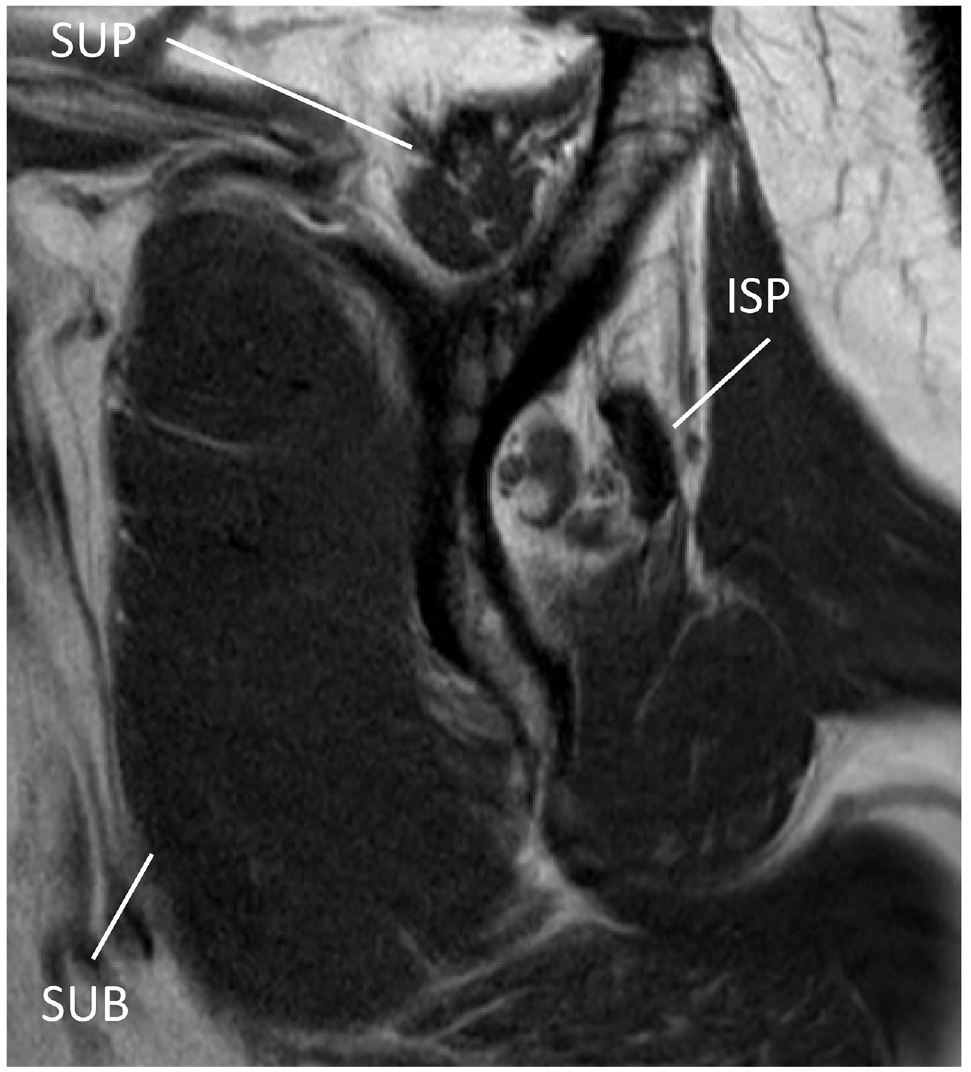
Evaluation of FI in a left shoulder showing Goutallier grade 3 in the ISP, grade 1 in the SUB, and grade 2 in the SSP. FI, fatty infiltration; ISP, infraspinatus; SSP, supraspinatus; SUB, subscapularis.
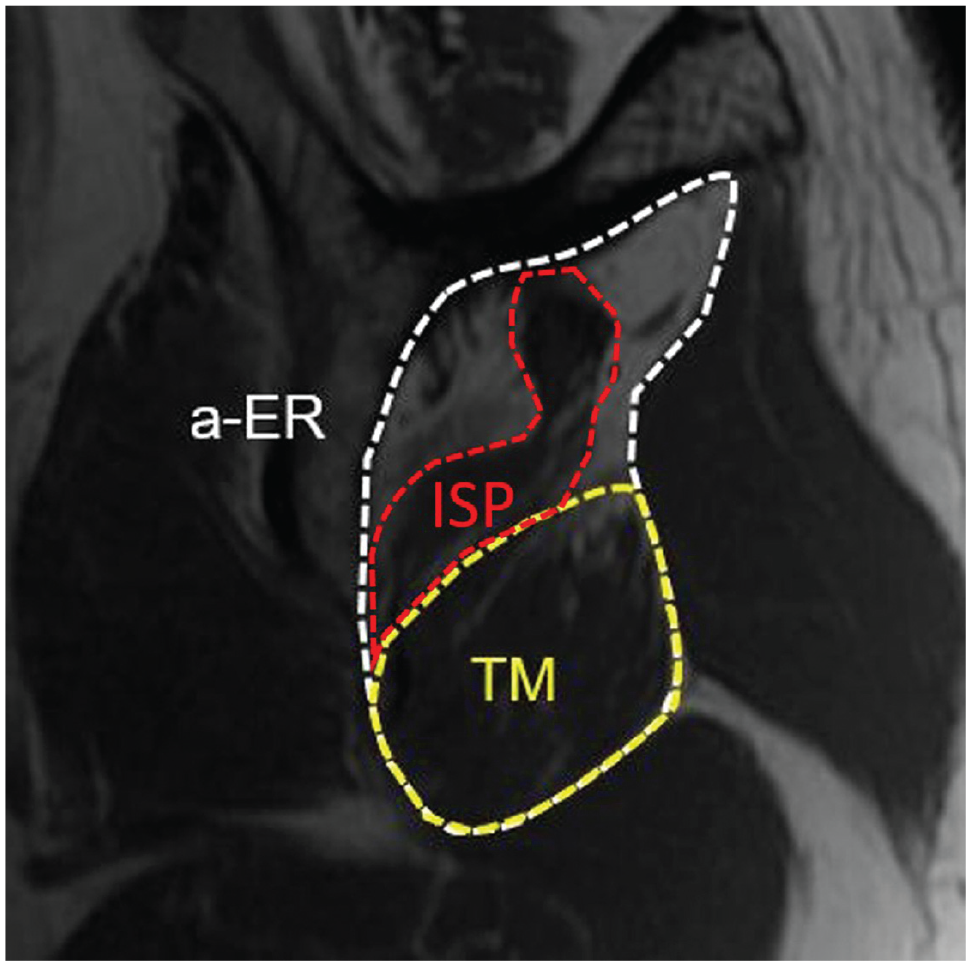
The areas of the ISP, TM, and a-ER muscles are outlined on a Y-view MRI scan of a left shoulder. The occupational ratio of the ISP muscle was 0.212, indicating ISP atrophy. The occupational ratio of the TM muscle was 0.487, indicating TM hypertrophy. a-ER, anatomic external rotator; ISP, infraspinatus; MRI, magnetic resonance imaging; TM, teres minor.
Tendon retraction was evaluated with the modified Patte classification according to Guo et al. 14 Tendon retraction was assessed on 2 specific oblique coronal MRI scan sections: section A (defined as the first slice when coracoid is in contact with the scapular body) and section P (defined as the first slice when spinae scapulae is separated from the scapular body). The modified Patte classification consisted of stage 1, in which the tendon was lateral to the glenoid in sections A and P; stage 2, in which the tendon was medial to the glenoid on either section A or P; and stage 3, in which the tendon was medial to the glenoid in sections A and P (Figure 3).

Tendon retraction was evaluated with the modified Patte classification of a right shoulder on oblique coronal view MRI scan. (A) The base of coracoid process (circle) was in contact with the scapular body in section A. (B) The spinae scapulae (ellipse) is separated from the scapular body in section P. The residual tendon was medial to the glenoid in sections A and P, indicating tendon retraction of modified Patte stage 3. MRI, magnetic resonance imaging.
The acromiohumeral distance was measured on oblique coronal MRI scan, in which the distance between the undersurface of the acromion and the top of the humeral head was shortest (Figure 4). 14

AHD (arrow) in a left shoulder. AHD, acromiohumeral distance.
The PS-Tetra Score
The PS-Tetra Score was used to assess 4 aspects (ie, tetralogy) of shoulder function: SSP atrophy, FI of the SSP, ISP atrophy, and FI of the ISP, with related criteria listed in Table 1. For a specific case, the PS-Tetra Score equaled the number of aspects met (Figure 5). Two examiners (Q.Q. and P.Z.) determined the PS-Tetra Scores for all included shoulders. Scores were measured twice at a 3-month interval.
PS-Tetra Score a

FI, fatty infiltration; ISP, infraspinatus; PS-Tetra Score, the posterosuperior tetralogy scoring system; SSP, supraspinatus.
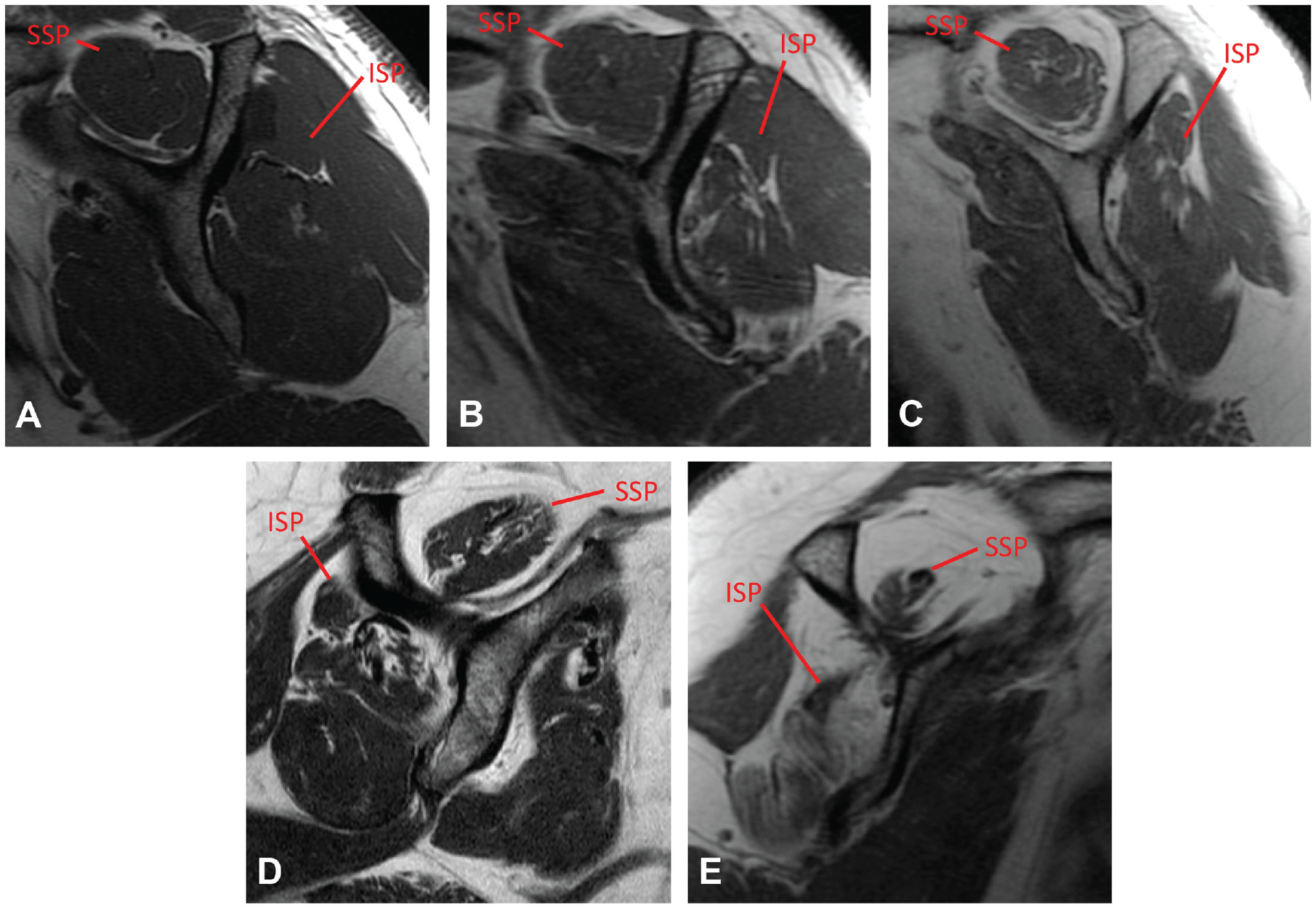
The PS-Tetra Score. (A) A left shoulder with no obvious atrophy or FI of the SSP or ISP, indicating a PS-Tetra Score of 0. (B) A left shoulder with FI of the ISP, indicating a PS-Tetra Score of 1. (C) A left shoulder with FI of the SSP and ISP, indicating a PS-Tetra Score of 2. (D) A right shoulder with atrophy of the ISP and FI of the SSP and ISP, indicating a PS-Tetra Score of 3. (E) A right shoulder with atrophy and FI of both the SSP and ISP, indicating a PS-Tetra Score of 4. FI, fatty infiltration; ISP, infraspinatus; PS-Tetra Score, the posterosuperior tetralogy scoring system; SSP, supraspinatus.
Statistical Analysis
An independent t test or Mann-Whitney U test was used for the analyses of continuous variables, the paired t test was used to compare the preoperative and 2-year postoperative ASES scores, and the chi-square test or Fisher exact test was used to compare categorical variables. Variables were selected for univariate analysis if they were found to have potential for affecting shoulder function or rotator cuff muscle function. A binary logistic regression analysis was used to determine independent factors affecting poor postoperative shoulder function (ASES score ≤70) by inputting the significant variables derived from the univariate analysis using the stepwise forward conditional method. Statistical analyses were conducted using SPSS for Windows Version 22 (SPSS). All statistical tests were 2-tailed, and a P value <.05 was considered as statistically significant.
Intraobserver and interobserver reliability of the PS-Tetra Score were assessed by calculating the intraclass correlation coefficient (ICC). The crude agreement, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of using different indicators to predict poor shoulder function.
Results
Patient Characteristics
A total of 242 L/MRCT repairs were performed between October 1, 2015, and June 30, 2019. A total of 55 shoulders were excluded because of undesired tear pattern (n = 26), insufficient follow-up period (n = 17), and incomplete sets of images (n = 12). The final study group consisted of 187 shoulders from 180 patients, with a mean follow-up period of 3.11 ± 1.51 years. The mean age of the patients at surgery was 57.78 ± 8.74 years. The other characteristics are summarized in Table 2. The difference between mean preoperative and postoperative 2-year ASES score (45.58 ± 18.76 and 83.07 ± 13.34) was statistically significant (P < .001).
Patient Characteristics a
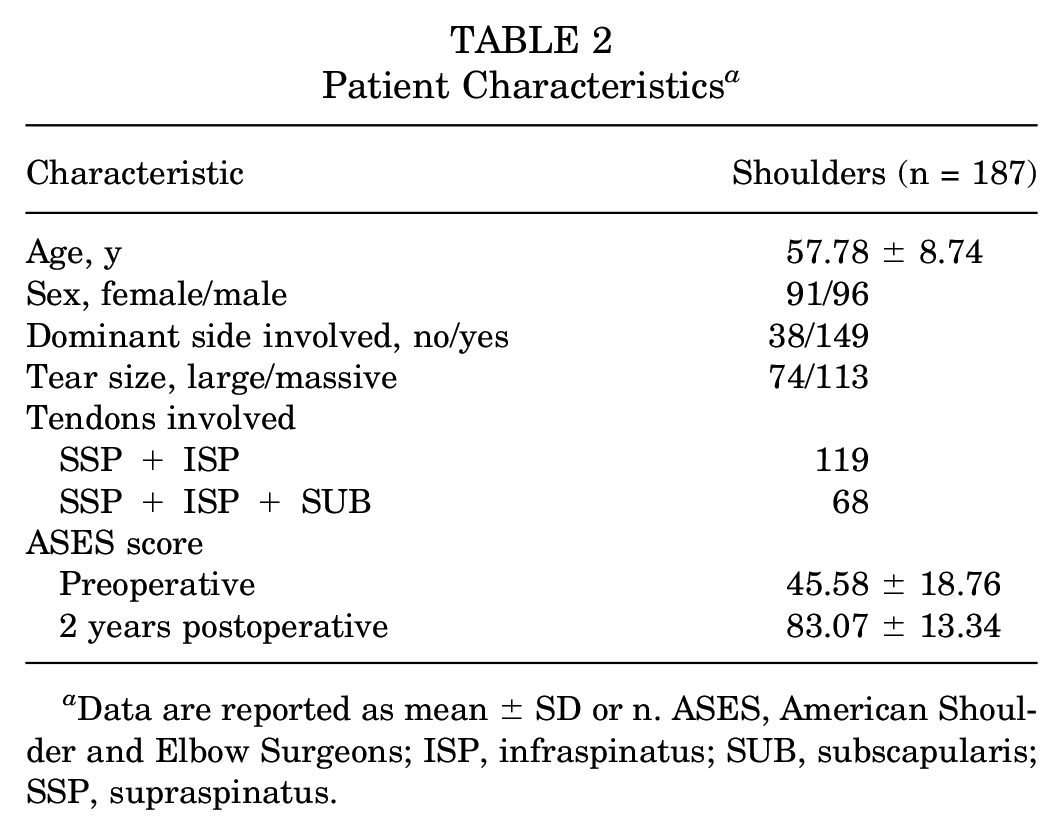
Data are reported as mean ± SD or n. ASES, American Shoulder and Elbow Surgeons; ISP, infraspinatus; SUB, subscapularis; SSP, supraspinatus.
When comparing shoulders with good function (ASES score >70; n = 155) and poor function (ASES score ≤70; n = 32), active ROM in forward elevation (P < .001), external rotation at side (P < .001), and internal rotation (P < .001) were significantly worse in the shoulders with poor shoulder function (Table 3). A post hoc power analysis was performed using G*Power software (Version 3.1; Heinrich Heine University) to detect whether the sample sizes of 155 (good function group) and 32 (poor function group) would be reasonable. With an effect size of 0.8 and α of 0.05 with 2 tails, the power was 0.984, suggesting that the sample sizes were sufficient.
Characteristics of Shoulders with Good (ASES Score >70) Versus Poor (ASES Score ≤70) Function a

Data are reported as mean ± SD or n. Boldface P values indicate statistically significant difference between groups (P < .05). AHD, acromiohumeral distance; ASES, American Shoulder and Elbow Surgeons; PS-Tetra Score, the posterosuperior tetralogy scoring system; ROM, range of motion; TM, teres minor.
Results shown as highest vertebral level reached (range).
Factors Affecting Poor Postoperative Shoulder Function
In the univariate analysis, female sex (P = .013), a higher Goutallier grade of the SSP (P = .001) and ISP (P = .001), positive SSP tangent sign (P = .035) and PS-Tetra Score ≥3 (P < .001) was associated with poor postoperative shoulder function (Table 3).
In the binary logistic regression analysis, PS-Tetra Score ≥ 3 (P < .001) was the only risk factor for poor postoperative shoulder function, while sex, Goutallier grade of SSP or ISP and SSP tangent sign were not (Table 4). The occurrence rate of poor postoperative function in shoulders with a PS-Tetra Score of 0, 1, 2, 3, and 4 was 0% (0/52), 0% (0/52), 19.57% (9/46), 58.06% (18/31), and 83.33% (5/6), respectively.
Binary Logistic Regression Analysis of Risk Factors Affecting Poor Shoulder Function a

Boldface P value indicates statistical significance (P < .05). CI, confidence interval; FI, fatty infiltration; ISP, infraspinatus; OR, odds ratio; PS-Tetra Score, the posterosuperior tetralogy scoring system; SSP, supraspinatus.
The PS-Tetra Score
Inter- and Intraobserver Reliability
The interobserver reliability of the PS-Tetra Score was excellent, with ICCs of 0.986 for the first time and 0.978 for the second time (P < .001 for both). Both examiners had excellent intraobserver reliability, with ICCs of 0.988 and 0.994 (P < .001 for both).
Diagnostic Value of the PS-Tetra Score to Predict Poor Shoulder Function
The crude agreement, sensitivity, specificity, PPV, and NPV of using the different indicators (PS-Tetra Score ≥3, SSP Goutallier grade ≥2, ISP Goutallier grade ≥2, and positive SSP tangent sign) to predict poor shoulder function are shown in Table 5. PS-Tetra Score ≥3 possessed higher crude agreement (87.70%), specificity (90.97%), and PPV (62.16%) than the other 3 indicators. It also had high NPV (94.00%) and moderate sensitivity (71.88%). Although SSP Goutallier grade ≥2 had the highest sensitivity (90.63%), the crude agreement (54.55%), specificity (47.10%) and PPV (26.13%) was rather low. ISP Goutallier grade ≥2 had a low PPV (27.71%). Positive tangent sign had a low sensitivity (25.00%) and PPV (34.78%).
Diagnostic Value of Indicators to Predict Poor Shoulder Function a

Data are shown as % (n/N). CA, crude agreement; ISP, infraspinatus; NPV, negative predictive value; PPV, positive predictive value; PS-Tetra Score, the posterosuperior tetralogy scoring system; SSP, supraspinatus.
The ROC curves of using different indicators to predict poor shoulder function are illustrated in Figure 6. The indicator PS-Tetra Score ≥3 possessed a higher area under the ROC curve (AUC = 0.814) than the other 3 indicators (Table 6).
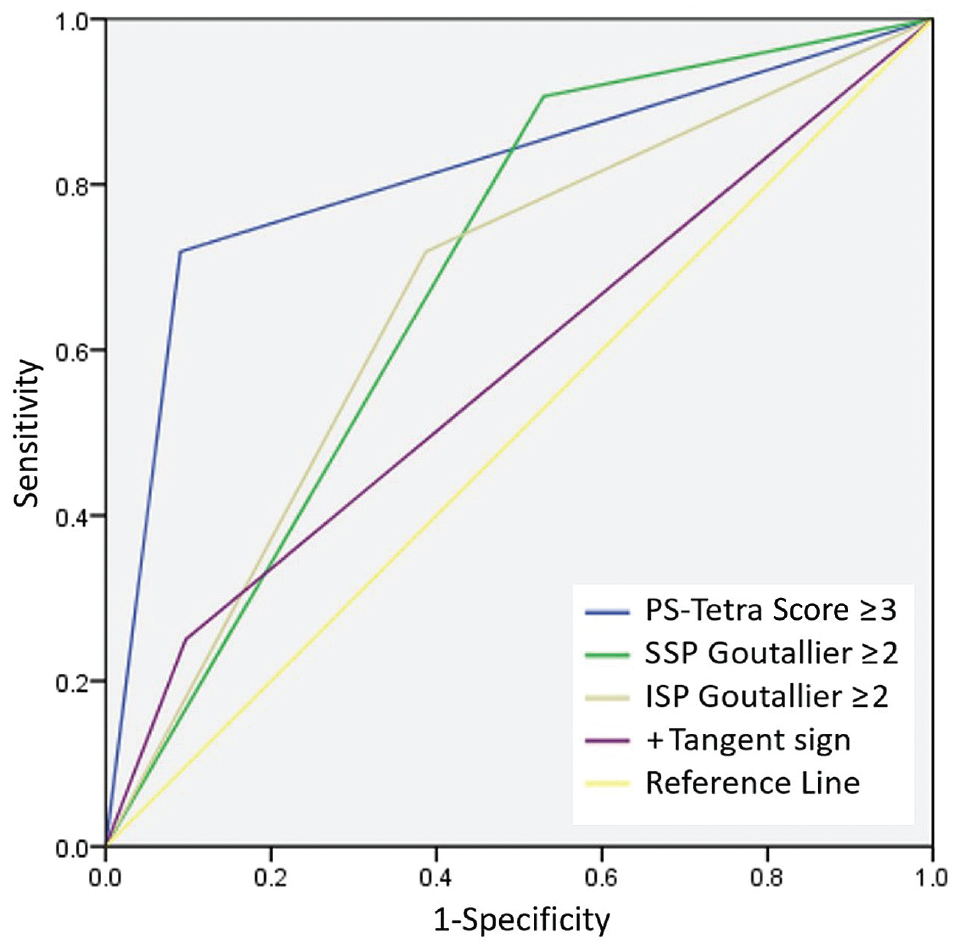
ROC curves using different indicators to predict poor shoulder function. ISP, infraspinatus; PS-Tetra Score, the posterosuperior tetralogy scoring system; ROC, receiver operating characteristic; SSP, supraspinatus.
Results of ROC Models to Predict Poor Shoulder Function a

AUC, area under the ROC curve; ISP, infraspinatus; PS-Tetra Score, the posterosuperior tetralogy scoring system; ROC, receiver operating characteristic; SSP, supraspinatus.
Discussion
The most important finding of this study was that a PS-Tetra Score ≥3 was an accurate predictor of poor shoulder function after L/MRCT repairs, with higher reliability and superior validity than isolated FI or atrophy of SSP or ISP alone.
Both atrophy and FI have been associated with decreased elasticity and contractile force of rotator cuff muscles10,27,34 and might be the reasons for poor postoperative shoulder function. However, neither of them in isolation, and using only a single muscle, can be taken as an accurate predictor for postoperative functional outcomes. The results of this study revealed that using Goutallier grade ≥2 of SSP or ISP had a rather low PPV (26.13% and 27.71%, respectively) of predicting poor postoperative function, which suggested that only one-quarter of patients with Goutallier grade ≥2 of either SSP or ISP actually experienced poor function after surgery. A positive SSP tangent sign likewise had low sensitivity (25.00%) and PPV (34.78%) for predicting shoulder function. Possible explanations include that atrophy was not as responsible for SSP contractile force loss as FI was. 34 Muscle atrophy accounted for the loss in force in tenotomized muscles with minimal FI. In addition, the determination of SSP atrophy on the Y-view of the MRI scan might be disturbed by retraction. 8
Although ISP atrophy has been associated with shoulder function,11,30 our results did not reveal this association, even in univariate analysis. This discrepancy might result from the different methods used for judging ISP atrophy. In this study, an ISP occupational ratio <0.586 was defined as ISP atrophy, according to the method proposed by Kikukawa et al. 16 However, in this study, an occupational ratio <0.586 was sometimes seen in an ISP muscle with a smooth border and absence of FI, which might not represent actual atrophy. The occupational ratio of the ISP seemed to be related to Y-view selection, TM hypertrophy, and the native muscle outline of the ISP and TM.
When a diverse extent of FI and atrophy presented in multiple rotator cuff muscles, it might not be reasonable to use only FI or atrophy of a single muscle to predict shoulder function. The main strength of the PS-Tetra Score was the integration of FI and atrophy of SSP and ISP, which might better reflect the function of the entire posterosuperior rotator cuff complex. Shoulder function after RCR can be influenced by many factors, such as the number of torn tendons and the severity of FI and atrophy, which are difficult to predict precisely using any single parameter. Less severe FI or atrophy of 1 or 2 torn tendons might not result in shoulder function impairment. Our results demonstrated that a PS-Tetra Score ≥3 possessed greater diagnostic value to predict poor postoperative shoulder function than using isolated FI or atrophy of SSP or ISP alone, which might reveal the threshold of shoulder function impairment after RCR.
Kikukawa et al 16 demonstrated that compensatory TM hypertrophy could provide greater strength and range of external rotation. However, TM hypertrophy did not affect shoulder function after repair of L/MRCTs in this study, which was in line with the outcomes reported by Oh et al. 30 We assumed that the compensatory effects of TM “hypertrophy” might not reflect real muscle hypertrophy if the ISP were severely atrophic, or it may not adequately compensate for severely affected SSP and ISP muscles.
Melis et al 25 suggested that RCT repair should be performed before the appearance of FI of Goutallier grade 2 and atrophy (positive tangent sign), especially when the tear involves multiple tendons. Our results showed that Goutallier grade 2 and atrophy was associated with poor function after repair or L/MRCTs. However, shoulders with a PS-Tetra Score of 1, which meant moderate FI or atrophy of single SSP or ISP, did not always end up with poor postoperative function. Even shoulders with a PS-Tetra Score of 2, which exhibited mostly moderate FI of both SSP and ISP, had an 80% chance of acceptable function. In other words, patients with a PS-Tetra Score <3 usually did not showed poor postoperative function.
This study also included patients with partial SUB tears of Lafosse type 1 or 2. FI or atrophy of SUB was not observed in preoperative MRI scans. We assumed the force couple involved with SUB was intact. Thus, the shoulder function of these patients was considered the same as those with posterosuperior tears.
FI and atrophy have been considered as indications for alternative treatments for L/MRCT, such as lower trapezius or latissimus dorsi transfer.5,28 As patients with PS-Tetra Scores <3 usually did not showed poor postoperative function, tendon transfer might not be a suitable treatment for these patients. More than one-third of the patients with PS-Tetra Scores ≥3 had postoperative ASES scores >70. To avoid overtreatment, a PS-Tetra Score of 4 might be the most appropriate cut-off value for alternative treatments. Patients with a PS-Tetra Score of 3 might benefit from alternative or additional treatments other than RCT repair.
A post hoc power analysis was performed using G*Power software (Version 3.1; Heinrich Heine University) to detect whether sample sizes of 155 (ASES >70 group) and 32 (ASES ≤70) would be reasonable. With an effect size of 0.8 and α of 0.05 with 2 tails, the power was 0.984, suggesting that the sample size was sufficient.
Limitations
There are some limitations to this study. First, this was a retrospective study. Second, patients with inadequate imaging results or follow-up time were excluded, which could lead to selection bias. Third, ASES scores were used for subgrouping, which might not fully represent postoperative shoulder function. However, ROM was also used in this study to validate subgrouping by ASES scores. Finally, the PS-Tetra Score might not be accurate for predicting function of L/MRCTs characterized by SUB dysfunction.
Conclusion
A PS-Tetra Score ≥ 3 was confirmed to be a risk factor for poor shoulder function after repair of posterosuperior L/MRCTs and possessed greater diagnostic value than using isolated FI or atrophy of SSP or ISP alone for predicting shoulder function. Patients with PS-Tetra Scores <3 usually had good postoperative function.
Footnotes
Final revision submitted June 15, 2023; accepted June 29, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: funding for this study was received from the National Natural Science Foundation of China (to C.J., general program, 82172513). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Beijing Jishuitan Hospital.