
Abstract
Background:
Managing an in-season anterior shoulder instability poses a special challenge for team physicians, as they need to balance the aim of promptly returning the athlete to play while mitigating the chances of recurrence and further injury to the shoulder.
Purpose:
To investigate and report on the treatment preferences of National Hockey League (NHL) team physicians when managing in-season first-time anterior shoulder instability in professional hockey players.
Study Design:
Cross-sectional study.
Methods:
A survey consisting of 33 sport-specific questions focused on the treatment options and preferences for anterior shoulder instability in hockey players was developed, and 32 NHL team physicians were invited to anonymously complete the survey. Following the collection of the data, the distribution of the responses to each question was documented as counts and percentages.
Results:
Of the 32 invited team physicians, 31 (97%) completed all (n = 28) or most (n = 3) of the survey. The mean experience of the respondents was 13 ± 11 years. A total of 28 (90%) respondents would attempt nonoperative treatment of an in-season initial anterior shoulder dislocation with an isolated soft tissue injury, while 28 (90%) would recommend operative treatment of the same injury with bony involvement. Of the 31 respondents, 30 (97%) utilized rehabilitation parameters rather than time from injury when determining whether a player could return to play. Of those parameters, clinical strength (100%), range of motion (87%), anterior apprehension (84%), and pain (65%) were the most utilized. For surgical management of an isolated soft tissue lesion, 28 (90%) of the respondents preferred arthroscopic repair, while 2 (7%) preferred open repair.
Conclusion:
Of the 32 NHL team physicians surveyed, 28 preferred nonoperative management for the treatment of initial anterior shoulder dislocations with isolated soft tissue injuries, while initial operative management was preferred by the same number of team physicians for any injuries with bony involvement.
Professional hockey players are susceptible to various injuries due to the high speed of play and nature of the sport. Because of the high intensity and aggressive nature of the sport, the shoulder is at particular risk, accounting for 54.4% of all upper extremity injuries. 38 One of the most common injuries to the shoulder among hockey players is anterior shoulder subluxation/dislocation with resultant anterior instability. 29 Anterior shoulder instability occurs primarily after a traumatic event when the humeral head is dislocated from the glenohumeral joint, leading to a soft tissue or bony insult. These injuries pose a unique challenge to the athlete, as appropriate and expedient management can have serious consequences on performance and career longevity. Currently, the main treatment options for in-season anterior shoulder instability are nonoperative management and surgical procedures such as Latarjet, open Bankart repair, and arthroscopic Bankart repair.
Managing an in-season anterior shoulder instability poses a special challenge for team physicians. Team physicians need to balance the aim of promptly returning the athlete to play while mitigating the chances of recurrence and further injury to the shoulder. Shoulder instability in professional contact athletes is common and can result in a considerable amount of time missed based on a variety of factors. Anderson et al 1 highlighted this in an epidemiologic study of shoulder instability in National Football League (NFL) athletes. During their study period (2012-2017), there were 403 missed-time shoulder instability injuries in 355 different players with a median of 47 days missed after a shoulder dislocation and 13 days missed after a subluxation event. 1 Other studies on nonprofessional athletes found that if the player is treated nonoperatively, the mean return-to-play (RTP) time is 10.2 days. 9 Recurrence is high, and reaggravation of the injury can lead to prolonged RTP times and subsequently worse outcomes. 13 Okoroha et al 31 found that 54.6% of nonoperatively treated NFL athletes had a recurrent instability episode. However, if the player is treated surgically, the mean RTP is 4.1 months, requiring a lengthy rehabilitation course. 13 Depending on the severity of the injury, the individual player might see a significant decrease in number of games played and a reduction in financial compensation, in terms of contracts, endorsements, publicity, and bonuses.4,20 As a result, operative versus nonoperative management should be individualized based on several key factors. Surveying team physicians on how these factors influence their decision-making will offer key insights into optimal management practices of anterior shoulder instability among professional athletes.
In collision athletes, first-time, in-season shoulder instability without glenoid bone loss is typically managed nonoperatively.2,9,23,25,30,33,35 Athletes with recurrent instability, subcritical glenoid bone loss between 13.5% and 25%, and glenoid bone loss >25% are generally treated operatively.2,5,25,30,33,35 Interventions may vary depending on the amount of glenoid bone loss. These include arthroscopic versus open anterior capsulolabral reconstruction with or without remplissage as well as a Latarjet or other glenoid osseous augmentation procedure. The standard of care for anterior shoulder instability in the NHL athlete is not well-defined.
The purpose of this study was to investigate and report on the treatment preferences of NHL team physicians when managing in-season, first-time anterior shoulder instability in professional hockey players. We hypothesized that in-season, first-time anterior shoulder instability in NHL players is currently being treated nonoperatively for most injuries.
Methods
We collaborated on and developed a survey consisting of 33 sport-specific questions focusing on the preferred treatment approach for a professional hockey player who sustained an anterior shoulder dislocation. Considerations incorporated into the survey questions included whether the injury was an inaugural or a recurrent event, at what point in the season the event occurred, and both the operative and nonoperative treatment preferences of the participating physician/surgeon. The survey questions were uploaded to Research Electronic Data Capture (REDCap; Vanderbilt University), a secure web-based application that is utilized for building and managing online surveys and databases. This study was determined to be exempt from institutional review board approval, and all answers from the survey were kept anonymous.
Beginning in April 2021, invitations to complete the online survey were electronically distributed to 32 NHL team physicians/surgeons (32 teams in the NHL). The team physicians consisted of 30 orthopaedic surgeons and 2 primary care orthopaedic sports medicine physicians. This invitation included a secure link allowing access to the REDCap survey and the necessary instructions required for its completion. Parameters were set within REDCap that blinded the identity of the participants associated with each set of responses. With regard to questions involving surgical decision-making, nonoperative team physicians were asked to consult their team orthopaedic surgeon. Data collection continued through November 2021, when the final call for responses was distributed and the survey was closed. All responses were compiled using Microsoft Excel, and the results were then analyzed and compared.
Results
By the end of the collection period, 31 of the 32 team physicians/surgeons submitted responses to the anonymous survey, for a response rate of 97%. Of the 31 surveys, 28 (90%) were completed in their entirety, 2 surveys (7%) were each missing 1 response (97% completion), and 1 survey (3%) was partially completed (first 20 questions; 61% completion). The mean experience of the respondents was 13 ± 11 years, and the mean number of annual shoulder stabilization procedures performed was 54.29 (range, 0-300).
During the first half of the season, 28 respondents (90%) were likely to treat a first-time anterior shoulder dislocation with an isolated soft tissue labral injury (Bankart) nonoperatively. Three (10%) would initially recommend surgical stabilization. In the same scenario but for a lesion with bone involvement (bony Bankart lesion), 28 (90%) were likely to recommend surgical stabilization, while 3 (10%) would still initially attempt nonoperative management (Figure 1).

Responses of National Hockey League team physicians when asked how they would treat a first-time anterior shoulder dislocation in a player with a soft tissue versus a bony Bankart lesion (injury in the first half of the season): 90% of respondents would recommend nonoperative management for soft tissue–only lesions, while 90% of respondents would recommend surgical stabilization for lesions with bony involvement.
With regard to the timing of the injury, a first-time anterior shoulder dislocation in the second half of the season or the playoffs could affect the recommendation for 14 (45%) physicians for patients with soft tissue–only lesions and 11 physicians (35%) for patients with late-season bony Bankart lesions, with initial recommendations for nonoperative management being more likely or influenced. Respondents typically cited that if the team was either in or likely to head to the playoffs, nonoperative management would be preferred. If the team was not in the playoffs and the injury occurred in the second half of the season, respondents had a lower threshold to recommend surgery.
With regard to diagnostic imaging, if the magnetic resonance imaging showed a Bankart lesion, 23 (74%) respondents would not routinely order a computed tomography scan to assess for bony involvement. If nonoperative management were selected, 21 of 30 respondents (70%) would recommend a stabilizing shoulder brace for wear during play. The player's position was not a major influential factor for 21 (68%) of the respondents. Of the 32% who considered this potentially influential, the primary concern was that goalies would not be able to wear a brace with their gear. Player handedness, which determines which hand is the top hand and which hand is the bottom hand on the hockey stick, did not affect the treatment plan for 65% of the respondents. The major concern for the 35% potentially influenced by player handedness was that if the injured shoulder were on the side of the bottom hand on the stick, there was a greater risk for further instability, due to the routine and required positions for the shoulder of the bottom hand during play.
There were 3 major factors identified that could influence the decision to move forward with in-season surgical intervention: recurrent dislocation, recurrent subluxation(s) without dislocation, and the player's subjective sense of instability. Pain and apprehension were factors that were considered less influential. One respondent listed poor performance due to symptoms as an influential factor, and only 1 respondent listed the player's age as an influential factor in the recommendation for in-season surgery (Figure 2).
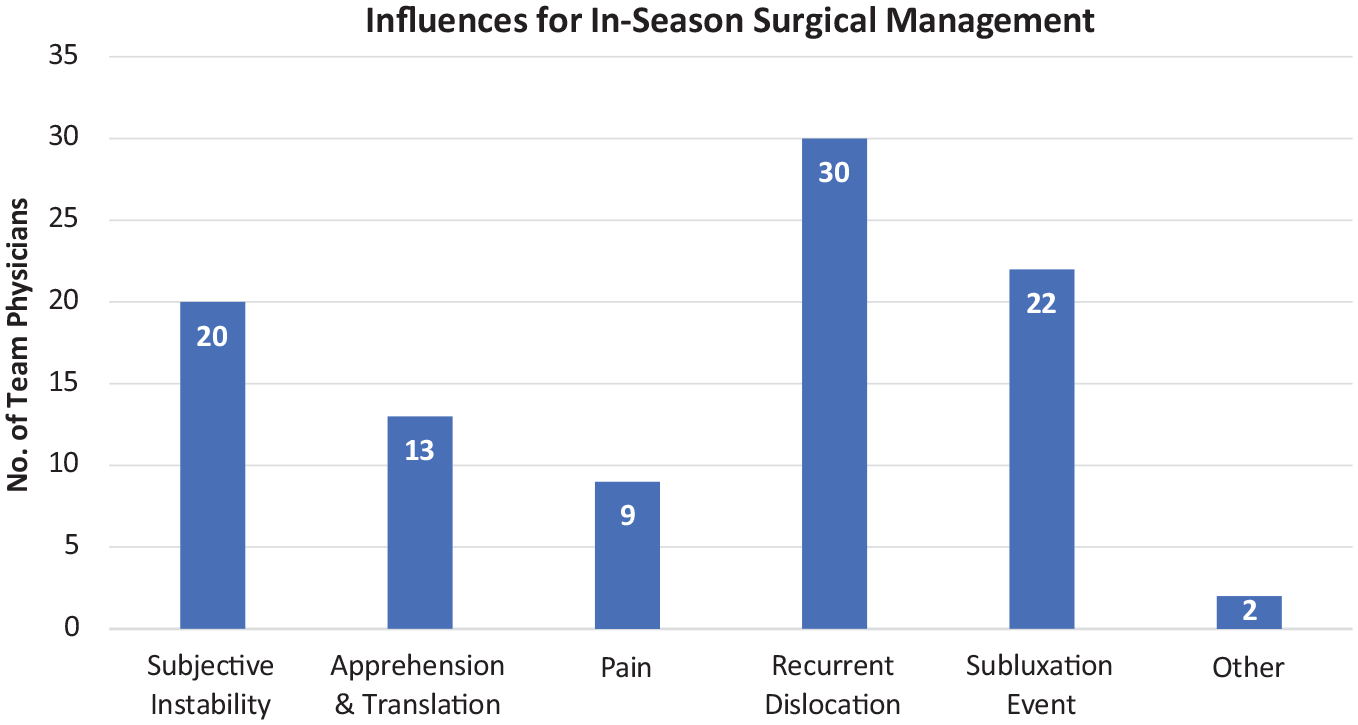
Responses of National Hockey League team physicians when asked which factors could influence the decision for in-season surgical intervention. Recurrent dislocation(s), subluxation(s), and subjective instability were most influential. The 2 “Other” responses included poor performance and patient age.
Questions regarding same-season RTP resulted in a wide variety of time-based responses with a mean of 4.23 weeks (range, 1-8 weeks). Regardless of time, 97% of respondents emphasized that the successful achievement of rehabilitation parameters ultimately determined a player's overall readiness to return. Of the rehabilitation parameters, 100% of respondents used clinical strength for this determination, with a majority also using range of motion (ROM), apprehension, and to a lesser extent, pain (Figure 3).

Responses of National Hockey League team physicians when asked which rehabilitation parameters they would use when determining the readiness of a player to return to play. Clinical strength was utilized by 100% of the respondents, with range of motion (ROM), apprehension, and pain as additional commonly used parameters. Biodex, Biodex dynamometer.
The team physicians were also questioned about surgical timing when moving forward with surgical intervention. We found that 77% would recommend proceeding with surgery at the end of that season, even if the player successfully completed the season after nonoperative treatment, and 87% would recommend in-season surgical stabilization if the player sustained a second dislocation in the same season. Ultimately, 100% of respondents would recommend surgery if a player sustained a second dislocation in a subsequent season. With regard to the preferred treatment method for an isolated soft tissue injury, 90% of the respondents would treat the soft tissue injury with arthroscopic repair, while 7% would utilize open repair. Last, a time-based question regarding postoperative RTP yielded 29 time-based responses with a mean RTP of 20.14 weeks (range, 12-24 weeks). One respondent maintained that RTP was still determined by functional progress and the successful achievement of rehabilitation parameters.
Discussion
The key findings of our survey of NHL team physicians were as follows. Soft tissue injuries in the first half of the season were primarily treated nonoperatively, with 28 of 31 (90%) respondents electing for nonoperative management. Bony injuries were primarily treated operatively, with an identical finding of 28 of 31 (90%) respondents choosing operative management. Soft tissue injuries occurring in the second half of the season would change treatment for 45% of the team physicians, whereas 35% would change treatment for bony injuries. We found that 100% of team physicians would pursue operative management for players sustaining a recurrent dislocation. Finally, 97% of team physicians emphasized that the successful achievement of rehabilitation parameters ultimately determined a player's overall readiness to return, with clinical strength being the most utilized factor.
Shoulder injuries in ice hockey players make up anywhere between 8.6% and 21.9% of all upper limb injuries.16,21,37 The high-speed collision nature of hockey places players at particular risk for injury. When an instability event occurs, there are many clinical options when deciding how to manage this unique challenge for the in-season athlete. Many factors must be considered, such as imaging modalities, timing in the season, presence of bone loss, and RTP timing, to name a few. Contact athletes, such as football players and wrestlers, have been shown to be at high risk for recurrence with multiple studies examining the outcomes and management of said athletes.32,39 No consensus exists for the management of shoulder dislocation in hockey players.
In our study, 90% of respondents would treat an initial soft tissue injury nonoperatively. If a player does not have any contraindications to nonoperative management and is able to complete an evidence-based rehabilitation protocol, it is not an unreasonable option for an athlete to attempt RTP. 25 There are many factors that may affect decision-making for the physician and athlete to proceed with nonoperative management, including the timing of injury during the season, sport, position, handedness, and goals/priorities of the athlete. All of this must be balanced with the risk of recurrence. In this study, 68% and 65% of physicians surveyed stated they do not take position or handedness, respectively, into account. Those who did stated that goalies and bottom hand were more likely to need surgery. In a study examining 30 in-season athletes, Buss et al 9 showed that 87% of athletes were able to RTP at a mean of 10 days with rehabilitation and bracing. These athletes also experienced a recurrence of 1.4 episodes per athlete-season. Dickens et al 4 found that 49% of athletes were able to RTP after a median of 4 days and to complete the remainder of the season, but only 55% of athletes completed the season without a subsequent instability event. Swindell et al 37 showed that nonoperatively treated NHL players missed a mean of 25.6 games (±22.6 games) with 10.7% recurrence rate in the same season. Physicians in this study stated that nonoperative treatment would keep a player out of play for 2 to 6 weeks, depending on return of function, motion, and strength.
It is interesting to compare trends found in our study with the current literature on NFL athletes, as it is also an elite professional contact sport. Okoroha et al 31 evaluated 83 NFL players who experienced a shoulder instability event (72 dislocations and 11 subluxations) from 2006 to 2014 and found that 31% were treated operatively after their index instability episode while 69% were treated nonoperatively. Regardless of the initial treatment method, 92.8% of athletes achieved successful RTP; however, 46% later experienced a recurrent shoulder instability event. Nonoperatively managed RTP was significantly quicker for players who were injured late in the season compared with those injured early in the season (0.5 vs 3.1 weeks). Operatively treated players required significantly longer recover time (39.3 vs 2.3 weeks) than nonoperatively treated; however, the operative group was significantly less likely to have a recurrent instability event compared with the nonoperative group (26.1% vs 54.6%). 31
Although athletes treated nonoperatively are able to RTP at a reasonable rate and can often complete the season, it is important to understand that this is not without consequence. In a prospective cohort study of 714 athletes over 4 years, Dickens et al 15 found that recurrent episodes during a season led to further bone loss. In 23 athletes with first-time instability events, the mean glenoid bone loss was 6.8%; this subsequently increased to 22.8% in athletes with a single subsequent episode of recurrence. 15 LeClere et al 24 examined a single NFL team's medical records and found that nonoperative management of shoulder instability led to a significantly higher rate of repeat dislocation (41.7% vs 10.5%) as well as an earlier time to recurrence (4.4 vs 26 months). Additionally, NHL players who experienced a recurrence missed significantly more total career games compared with those who were treated initially with surgery (80.3 vs 35.2, respectively). 37 Considering all these factors, it is important to properly counsel athletes who wish to RTP on the risk of recurrence and the effect it can have on further joint damage to an athlete's shoulder.
If a bony injury was present, 90% of NHL team physicians responded that they would treat the injury operatively. In 2000, Burkhart and de Beer 8 published on the inverted-pear shape glenoid, which represented a significant amount of glenoid bone loss that signified high risk of failure after Bankart repair. This critical bone loss was initially defined as bone loss >25% of the glenoid width. Many studies followed, all with the goal of defining the critical amount of glenoid bone loss at which soft tissue repair would no longer be adequate and a bony procedure would be recommended.3,10,14,24,36 Studies by Shaha et al 36 and Dickens et al 14 demonstrated worse clinical outcome scores and an increased risk of recurrent instability in athletes with glenoid bone loss of >13.5%. These studies redefined the concept of “critical bone loss” and led to an update to the original algorithm for the management of in-season anterior shoulder instability that was proposed by Owens et al. 33 Athletes with subcritical glenoid bone loss of >13.5% are now recommended to undergo early in-season surgery. 33 When asked to elaborate on the effect of bone loss on decision-making, physicians participating in this study described bone loss of >10% to 15% leading to acute surgery, with possible bony procedure for larger defects. Despite this, 74% of physicians would not order a computed tomography scan routinely to evaluate for bone loss. If the injury happened in the second half of the season, many physicians stated they would attempt rehabilitation and RTP, especially if the team was going to the playoffs.
For those patients with an isolated soft tissue lesion or subcritical glenoid bone loss that does not require bony stabilization, the surgeon may choose to perform either an open or arthroscopic Bankart repair. In the current study, 90% of NHL team physicians responded that they would perform an arthroscopic repair over an open repair. Open repairs were favored historically due to the belief they resulted in a lower recurrence rate. 34 More recent literature has shown no significant difference in the recurrence of instability after either arthroscopic or open Bankart repair. 7 Fabbriciani et al 19 conducted a prospective randomized study comparing open versus arthroscopic treatment of Bankart lesions and reported that there were no differences in recurrence or patient-reported outcomes at 2 years postoperatively. Bottoni et al 7 demonstrated similar results in a prospective randomized control study of 64 patients, finding no difference in failure rates between the open (6.9%) and arthroscopic (3.1%) groups at 2 years. When 60 of the patients were evaluated 15 years later, there was again no significant difference between the open and arthroscopic groups, although the rate of failure did increase (12.5% and 14.3%, respectively). 6 In a systematic review of 26 studies (N = 1781 patients), 22 arthroscopic repair had a recurrence rate of 8.5% versus 8.0% in open Bankart repair techniques (P = .82). Each technique has its advantages and disadvantages and should be considered based on injury and patient characteristics as well as surgeon preferences.
When assessing a player for RTP, rehabilitation parameters were the most important factors for NHL team physicians. Rather than any specific time period, physicians considered clinical strength (100%), ROM (87%), apprehension (84%), and pain (65%) before return to play. Rehabilitation after an acute episode of traumatic anterior instability generally consists of 3 phases. 27 For nonoperative management, phase 1 consists of reduction of pain and inflammation and adequate neuromuscular control. Phase 2 consists of achieving normal ROM and gentle exercises. Phase 3 focuses on advanced strengthening and RTP exercises. Commonly cited criteria for RTP include external rotation/internal rotation (ER/IR) strength ratio of 66% to 76% or higher at 180° per second, and ER to abduction ratio of 67% to 75% or higher at 180° per second, along with other shoulder-specific RTP functional assessments.11,12,40,41 In this study, 70% of physicians would recommend a brace when treating a first-time instability event nonoperatively. ROM should be 85% to 100% of the contralateral side, and strength 90% to 100% of the contralateral side, with minimal or no pain and negative apprehension except at extreme abduction/ER.
If surgery is performed, phase 1 of rehabilitation consists of protection of the repaired tissue and gentle passive and active-assisted ROM. 27 Phase 2 consists of restoring full ROM and beginning strengthening exercises for the rotator cuff and scapular stabilizers. Phase 3 focuses on restoring function for sporting activities. However, unlike ACL injury, there are limited data on RTP criteria after anterior shoulder instability. Matheson et al 28 proposed a 3-step RTP model for athletes after shoulder surgery. The first step is to evaluate the patient functionally, assessing symptoms, ROM, strength, and health status. Next, the clinician evaluates the participation risk based on the type of sports and the ability of the athlete to protect his or her shoulder. Finally, the clinician will evaluate modifiable risk factors including timing of the season and environment before RTP clearance. In terms of strength, an isokinetic ER/IR ratio of 66% or an isometric ER/IR ratio of 75% to 100% has been advised with the dominant shoulder typically 10% higher than the nondominant side.11,12,40,41 Deficits in glenohumeral motion have been associated with pain and risk for injury in overhead athletes. Therefore, side-to-side differences in internal rotation ROM are recommended to be <18° and total arc of motion difference no more than 5°. 42 Many other functional assessment tools are available and can be utilized based on the patient and the sport played to help guide the clinician toward a more evidence-based decision on RTP.
Strengths and Limitations
This study has several strengths. It is the first study to investigate the standard of care for anterior shoulder instability in ice hockey players. This was a detailed investigation of management trends for anterior shoulder instability in elite ice hockey players at the highest level. There was a high response rate, with 97% of all currently practicing NHL team physicians participating. Other studies seeking consensus opinion on management of a particular pathology by team physicians are often limited to 1 specific position.17,18,20,26 Our study was not limited to any position and thus could be applied to all professional ice hockey players.
There are several limitations to our study. First, these are all hypothetical scenarios. Real-life clinical scenarios are more nuanced and contain several variables that may affect clinical decision-making. The study did not take into account the shared decision-making and include the athlete’s/player’s thoughts on treatment. Additionally, this was a study based on expert opinion in a single sport rather than clinical data. These decisions are being made for male, professional athletes and may not apply to high school, collegiate athletes, or the general population participating in ice hockey recreationally.
Conclusion
Of the 32 NHL team physicians surveyed, 28 preferred nonoperative management for the treatment of initial anterior shoulder dislocation with isolated soft tissue injury, while initial operative management was preferred by the same number of team physicians for any injuries with bony involvement. Readiness to RTP was determined by rehabilitation parameters for ≥30 of 32 team physicians. When proceeding with surgical management, arthroscopic repair of isolated soft tissue lesions was preferred by ≥28 of the 32 team physicians. Defining the treatment approach taken by NHL team physicians for anterior shoulder instability injuries and defining how different clinical factors influence medical decision-making will offer key insights into optimal management practices of anterior shoulder instability among professional athletes.
Footnotes
Final revision submitted November 30, 2023; accepted February 12, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.G. has received grant support from Arthrex and education payments from Arthrex and Smith+Nephew. N.P. has received education payments from Mid-Atlantic Surgical Systems. R.E. has received education payments from Arthrex and Smith+Nephew and hospitality payments from Stryker. D.V. has received education payments from Arthrex and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Pittsburgh (ref No. STUDY20030061).