
Abstract
Background:
Approximately 20% of acute ankle sprains progress to chronic lateral ankle instability (CLAI), requiring surgical intervention. When only the anterior talofibular ligament (ATFL) is ruptured, it is controversial whether to perform arthroscopic inferior extensor retinacular (IER) reinforcement.
Purpose:
To assess the postoperative outcomes of IER reinforcement versus nonreinforcement in arthroscopic treatment of CLAI with ATFL-only injury.
Study Design:
Systematic review; Level of evidence, 3.
Methods:
Using PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, the PubMed, Cochrane Library, Embase, and Web of Science databases were searched for publications on arthroscopic ATFL repair with versus without IER reinforcement. The final search date was July 7, 2023. Through a comprehensive meta-analysis, functional outcomes (American Orthopaedic Foot & Ankle Society Ankle-Hindfoot [AOFAS], Karlsson-Peterson [K-P], and Foot and Ankle Outcome Score [FAOS] scores), radiological outcomes (talar anterior translation and talar tilt), and complication rates (superficial peroneal nerve injury, knot irritation, and total complications) were evaluated. The mean difference (MD) was compared for continuous outcomes, and the odds ratios (ORs) were compared for categorical outcomes between the patients with versus without IER reinforcement.
Results:
A total of 4 studies (n = 271 patients; 157 male, 114 female; 141 patients with IER reinforcement, 130 without IER reinforcement) were included in the final analysis. There were no significant differences between the patients with versus without reinforcement regarding AOFAS score (MD = 0.72 [95% CI, –2.17 to 3.61]; P = .63; I2 = 0%), any of the FAOS subscores, talar anterior translation (MD = 0.10 [95% CI, –0.53 to 0.73]; P = .76; I2 = 0%), talar tilt (MD = 0.14 [95% CI, –0.86 to 1.13]; P = .79; I2 = 0%), or total complications (OR = 2.29 [95% CI, 0.92 to 5.71]; P = .07; I2 = 24%). However, the IER reinforcement group showed superior postoperative K-P scores compared with the nonreinforcement group (MD = 6.22 [95% CI, 2.17 to 10.26]; P = .003; I2 = 0%).
Conclusion:
The results of the meta-analysis suggest that IER reinforcement may not be necessary for achieving satisfactory postoperative outcomes in CLAI with ATFL-only injury. Further research is required to investigate the impact of ligament injury severity, body weight, and concomitant calcaneofibular ligament injuries on the results.
Registration:
CRD42023447669 (PROSPERO).
Keywords
Ankle sprain is the most common injury to the ankle joint, comprising approximately 85% of all ankle injuries, with the majority being lateral inversion sprains. 33 The injury primarily involves the anterior talofibular ligament (ATFL), and the extent of damage to the ATFL ranges from mild stretching to severe complete tear. 30 Most patients achieve favorable treatment outcomes with temporary activity restriction and functional rehabilitation. However, studies have shown that up to 20% of acute ankle sprains may progress to chronic lateral ankle instability (CLAI), which may require surgical intervention. 40
Some studies have demonstrated that the Broström-Gould technique, which involves repairing the ATFL repair with an inferior extensor retinacular (IER) augmentation, has shown favorable outcomes in restoring lateral ankle stability.4,15,24 A previous study reported that IER reinforcement during ATFL repair can provide stability to the subtalar joint. Since its force vector is similar to that of the calcaneofibular ligament (CFL), IER reinforcement is important when ATFL injury is combined with CFL injury. 24 An anatomic investigation highlighted the importance of the oblique superolateral band in IER reinforcement, but its presence can be subject to variability owing to anatomic differences in the IER structure. 12 Concerns have been raised about the potential for overtightening the IER, which could lead to posterior subtalar joint stiffness. 2 Another concern arises from the IER reinforcement, as it may not strictly align with an anatomic repair due to its calcaneal attachment's being 10 mm anterior to that of the CFL, possibly limiting full ankle plantarflexion. 6
There has been debate about the need for IER augmentation during the arthroscopic repair of ATFL for CLAI. Therefore, this systematic review and meta-analysis aimed to pool the results of multiple studies to compare the effect of arthroscopic ATFL repair with and without IER reinforcement. We hypothesized that IER augmentation may not be necessary for arthroscopic repair of CLAI with ATFL-only rupture.
Methods
Search Strategy and Inclusion Criteria
The present study was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for reporting systematic reviews and meta-analyses. 29 We registered the review protocol in the PROSPERO database (CRD42023447669). 35 The PubMed, Cochrane Library, Embase, and Web of Science databases were searched; the last search date was July 7, 2023. The search procedure was based on the following keywords: (“Anterior Talofibular Ligament” OR “ATFL” OR “ankle lateral ligament” OR “Brostrom”) AND (“Inferior Extensor Retinacular” OR “inferior extensor retinaculum” OR “IER” OR “Modified Brostrom” OR “Brostrom-Gould”). We initially screened the title and abstract of each article to determine eligibility, followed by a full-text assessment of those meeting the criteria. Moreover, we thoroughly examined the references cited in the included articles for completeness.
Included in this systematic review were comparative studies of arthroscopic ATFL repair with versus without IER reinforcement. Noncomparative and acute ankle instability studies were excluded.
Quality Assessment
Two authors (B.Z. and L.S.) evaluated the quality of the included studies using the Cochrane risk-of-bias tool, 17 where risk of bias is assessed according to 7 domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and other sources of bias. For each criterion, a study is judged as having low, unclear, or high risk of bias. In addition, non–randomized controlled trials (RCTs) were evaluated according to the Newcastle-Ottawa Scale, which includes items on selection, comparison, and outcome bias. 38 Studies scoring ≥7 points are considered to be of high quality. The assessments of the included studies were conducted independently by 2 reviewers (B.Z. and L.S.), and any disagreements were resolved by consulting a third reviewer (J.Z.).
Data Extraction and Outcome Measures
Relevant data from the included studies, including first author, publication date, sample size, patient characteristics and follow-up time, and surgical approach, were extracted independently by 2 reviewers (B.Z. and L.S.). The outcome measures we evaluated were the American Orthopaedic Foot & Ankle Society Ankle-Hindfoot (AOFAS) score, the Karlsson-Peterson (K-P) score, Foot and Ankle Outcome Score (FAOS), talar anterior translation, talar tilt, and complication rate. The rates of superficial peroneal nerve injury and knot injury were also evaluated. When standard deviations were missing from studies, we attempted to contact the authors of articles by email to obtain relevant metrics. Medians and ranges were extracted without means and standard deviations, as recommended by Singotani et al. 37 Disagreements during the extraction process were resolved through consultation with a third investigator (J.Z.).
Statistical Analysis
Outcomes were compared between the patients who underwent arthroscopic ATFL repair with IER reinforcement (reinforcement group) versus those who underwent repair without IER reinforcement (nonreinforcement group). Data were analyzed using Review Manager (RevMan Version 5.4.1; Nordic Cochrane Center) for this meta-analysis. Mean differences (MDs) with 95% CIs were used for the analysis of continuous data, while odds ratios (ORs) with 95% CIs were used for the analysis of dichotomous data. Heterogeneity was determined with the I2 test, with I2 > 50% and P < .10 indicating high heterogeneity. In cases of significant heterogeneity, we applied random-effect models. Conversely, we used fixed-effect models when heterogeneity was low.
Results
Study Selection
After searching the databases, we identified 465 relevant articles. Of these publications, 4 studies16,18,25,34 comparing the effects of IER reinforcement versus nonreinforcement in arthroscopic ATFL repair were selected for this review. The PRISMA flow diagram (Figure 1) illustrates the literature search and selection process.

The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of the inclusion process for studies.
Study Characteristics
The included studies consisted of 1 RCT 18 , 1 cohort 25 and 2 retrospective cohort studies,16,34 with a total of 271 patients (157 male, 114 female), of whom 141 underwent ATFL repair with IER reinforcement and 130 had ATFL repair without IER reinforcement (Table 1).
General Characteristics of the Included Studies a

BMI, body mass index; CS, cohort study; F, female; M, male; ND, no data; NR, nonreinforcement; R, reinforcement; RCS, retrospective comparative study; RCT, randomized controlled trial.
Risk-of-Bias Assessment
The results of the Cochrane risk-of-bias assessment for each included study are shown in Figure 2. The 3 retrospective case-control studies16,25,34 evaluated using the Newcastle-Ottawa Scale were all rated as high quality, with scores of 9 (Table 2).

Results of the Cochrane risk-of-bias assessment for the included studies. 17 (A) Risk-of-bias summary. (B) Graph presenting overall risk of bias as percentages.
Quality Assessment for the 3 Non-RCT Studies According to the Newcastle-Ottawa Scale a

Key to items: S1 = representativeness of the exposed cohort; S2 = selection of the nonexposed cohort; S3 = ascertainment of exposure; S4 = demonstration that outcome of interest was not present at start of study; C1 = comparability of controls for the most important factor; C2 = comparability of controls for a second important factor; E1 = assessment of outcome; E2 = was follow-up long enough for outcomes to occur; E3 = adequacy of follow-up of cohorts. RCT, randomized controlled trial.
Each star represents 1 point, with each item being awarded up to 1 star. The total score can range from 0 to 9 points, with higher scores indicating higher study quality.
Functional Outcomes
The forest plots for the meta-analyses of functional outcomes are shown in Figure 3. Postoperative AOFAS scores were reported in 2 studies16,25 (65 patients in the reinforcement group and 56 patients in the nonreinforcement group). The reinforcement and nonreinforcement groups had mean scores of 89.9 and 89.1, respectively, with no significant difference (MD = 0.72 [95% CI, –2.17 to 3.61]; P = .63) and no heterogeneity (I2 = 0%; P = .33) (Figure 3A).
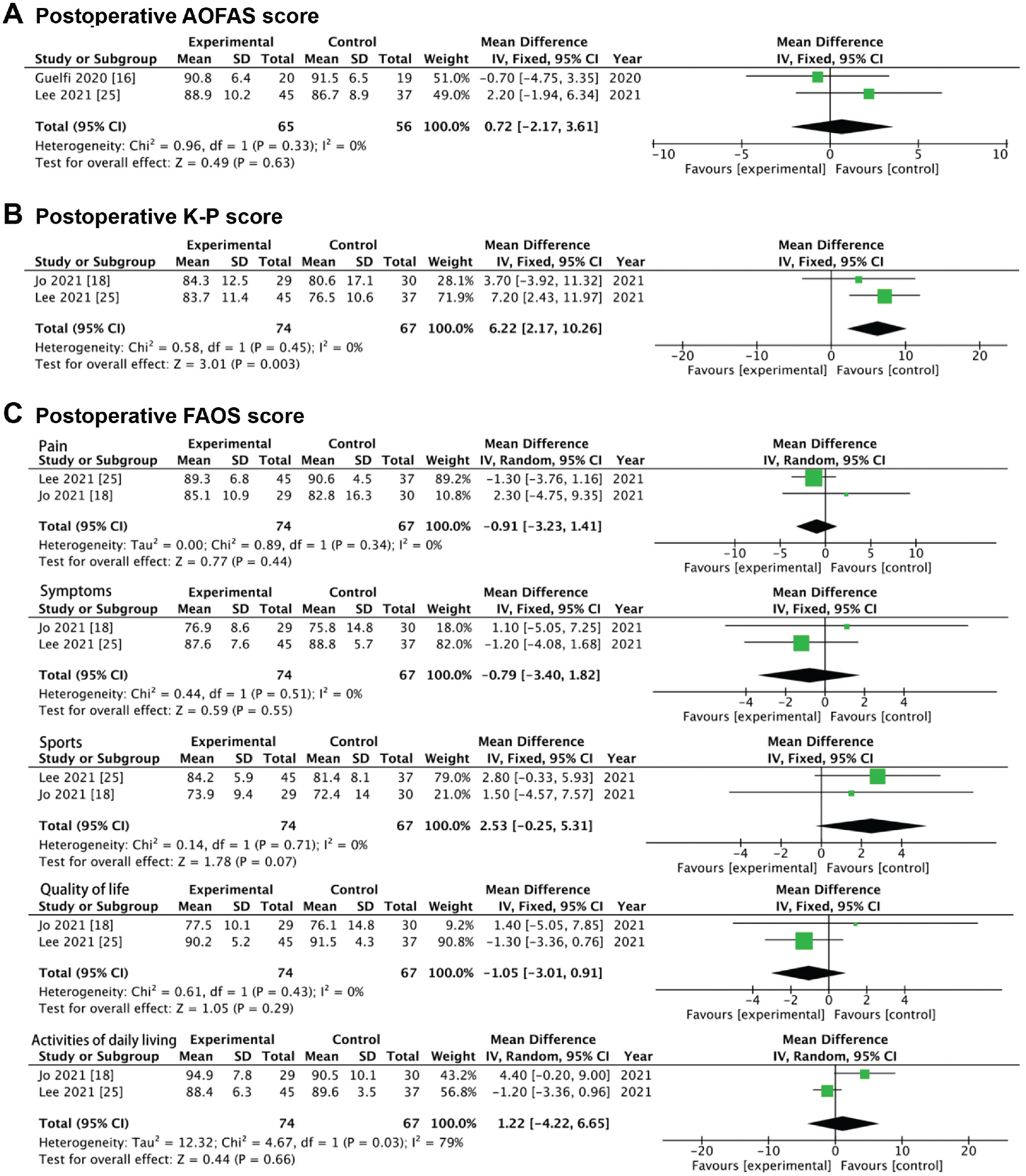
Forest plots showing the comparison of postoperative (A) AOFAS, (B) K-P, and (C) FAOS scores between the reinforcement (experimental) and nonreinforcement (control) groups. AOFAS, American Orthopaedic Foot & Ankle Society Ankle-Hindfoot; FAOS, Foot and Ankle Outcome Score; IV, inverse variance; K-P, Karlsson-Peterson.
Postoperative K-P scores were reported in 2 studies18,25 (74 patients in the reinforcement group and 67 patients in the nonreinforcement group). The mean scores for the reinforcement and nonreinforcement groups were 84.0 and 78.6, respectively, indicating a significant difference (MD = 6.22 [95% CI, 2.17-10.26]; P = .003), with no heterogeneity (I2 = 0%; P = .45) (Figure 3B).
Postoperative FAOS scores were reported in 2 studies18,25 (74 patients in the reinforcement group and 67 patients in the nonreinforcement group). There were no significant differences between the reinforcement and nonreinforcement groups on any of the mean subscores. FAOS Pain scores were 87.2 and 86.7, respectively (MD = −0.91 [95% CI, −3.23 to 1.41]; P = .44), with no heterogeneity (I2 = 0%; P = .34). FAOS Symptoms scores were 82.25 and 82.3, respectively (MD = −0.79 [95% CI, −3.40 to 1.82]; P = .55), with no heterogeneity (I2 = 0%; P = .51). FAOS Sports scores were 79.1 and 76.9, respectively (MD = 2.53 [95% CI, −0.25 to 5.31]; P = .07), with no heterogeneity (I2 = 0%; P = .71). FAOS Quality of Life scores were 83.9 and 83.8, respectively (MD = −1.05 [95% CI, −3.01 to 0.91]; P = .29), with no heterogeneity (I2 = 0%; P = .43). FAOS Activities of Daily Living scores were 91.7 and 90.1, respectively (MD = 1.22 [95% CI, −4.22 to 6.65]; P = .66); as the heterogeneity was high (I2 = 79%; P = .03), a random-effects model was used for this analysis (Figure 3C).
Radiological Outcomes
Postoperative talar anterior translation and talar tilt were reported in 2 studies18,25 (74 patients in the reinforcement group and 67 patients in the nonreinforcement group). The mean postoperative talar anterior translation was 5.65 mm and 5.55 mm in the reinforcement and nonreinforcement groups, respectively, with a significant group difference (MD = 0.10 [95% CI, –0.53 to 0.73]; P = .76) and no heterogeneity (I2 = 0%; P≥ .99) (Figure 4A). The mean postoperative talar tilt was 5.9 degrees and 5.7 degrees in the reinforcement and nonreinforcement groups, respectively, with no significant group difference (MD = 0.14 [95% CI, –0.86 to 1.13]; P = .79) and no heterogeneity (I2 = 0%; P = .56) (Figure 4B).
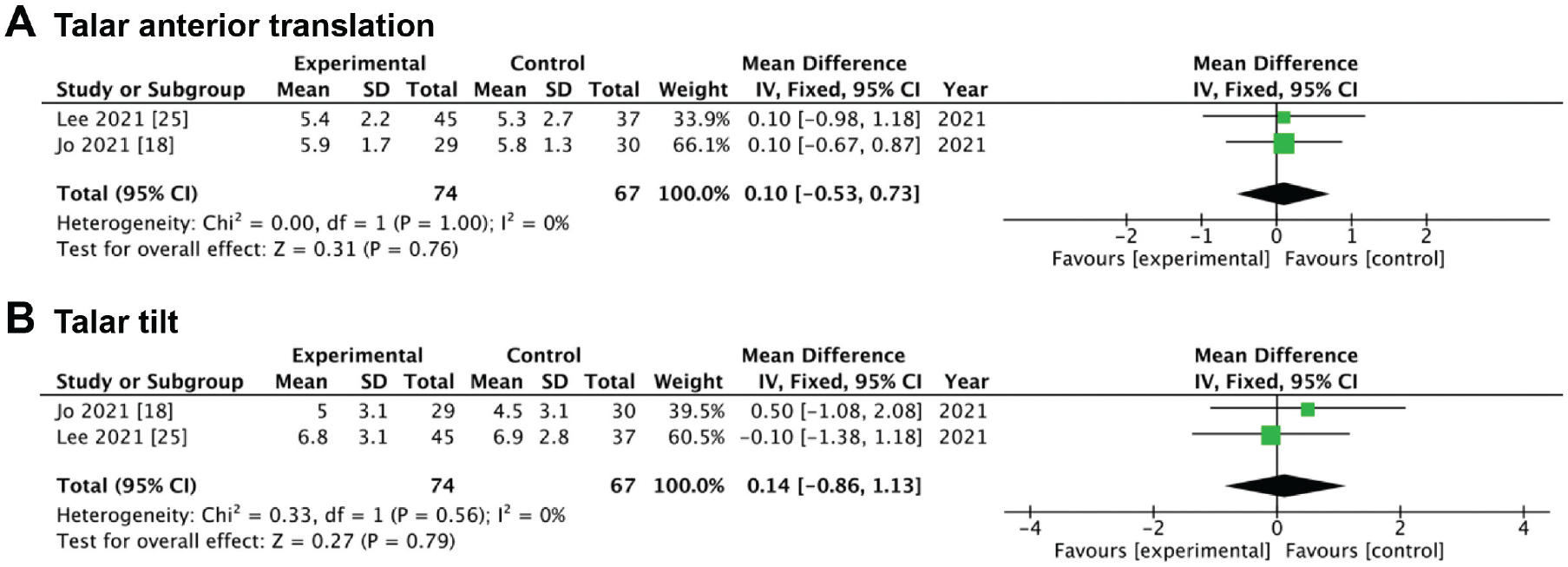
Forest plots showing the comparison of (A) talar anterior translation and (B) talar tilt between the reinforcement (experimental) and nonreinforcement (control) groups. IV, inverse variance.
Complications
The total complication rate was reported in 4 studies16,18,25,34 (141 patients in the reinforcement group and 130 patients in the nonreinforcement group). The mean total complication rate was 11.3% and 5.4% in the reinforcement and nonreinforcement groups, respectively, with no significant difference between the groups (OR = 2.29 [95% CI, 0.92-5.71]; P = .07) and no heterogeneity (I2 = 24%; P = .27). (Figure 5A)

Forest plots showing the comparison of (A) total complications, (B) superficial peroneal nerve injury, and (C) knot irritation between the reinforcement (experimental) and nonreinforcement (control) groups. M-H, Mantel-Haenszel.
The incidence of superficial peroneal nerve injury and knot irritation was reported in 3 studies16,18,25 (95 patients in the reinforcement group and 86 patients in the nonreinforcement group). The mean postoperative nerve injury rate was 6.3% and 1.2% in the reinforcement and nonreinforcement groups, respectively, with no significant difference between the groups (OR = 3.42 [95% CI, 0.69-16.89]; P = .13) and low heterogeneity (I2 = 30%; P = .60) (Figure 5B). The mean knot irritation rate was 4.2% and 0% in the reinforcement and nonreinforcement groups, respectively, with no significant group difference (OR = 3.57 [95% CI, 0.57-22.17]; P = .17) and no heterogeneity (I2 = 0%; P = .94) (Figure 5C).
Discussion
The findings of our meta-analysis indicated that IER augmentation may not be necessary for arthroscopic repair of CLAI with ATFL-only rupture. No significant differences between the patients with versus without IER reinforcement were seen in postoperative AOFAS scores (MD, 0.72), FAOS Pain scores (MD, –0.91), FAOS Symptoms scores (MD, –0.79), FAOS Sports scores (MD, 2.53), FAOS Quality of Life scores (MD, –1.05), FAOS Activities of Daily Living scores (MD, 1.22), anterior translation (MD, 0.10), talar tilt (MD, 0.14), total complication rate (OR, 2.29), superficial peroneal nerve injury rate (OR, 3.42), or knot irritation rate (OR, 3.57). Only postoperative K-P scores were significantly different, with the IER reinforcement group showing superior scores compared with the nonreinforcement group (MD = 6.22 [95% CI, 2.17-10.26]; P = .003; I2 = 0%).
Until recently, there has been controversy with regard to whether additional IER augmentation is essential in arthroscopic ATFL repair. Our study demonstrated that the postoperative outcomes of both surgical approaches are generally consistent, with the only notable difference being in the postoperative K-P scores, where the IER reinforcement group is superior to the group without IER reinforcement. The K-P score was introduced in 1991 to assess ankle joint function, explicitly focusing on ankle instability. Despite its widespread use, the validity of the K-P score has not been subjected to the same rigorous scrutiny as the AOFAS score. 23 As one of the most commonly employed clinician-based measures, the AOFAS score offers the advantage of being easily understood by nonclinicians. However, additional validation studies are still required to establish the reliability and clinical significance of the AOFAS score, especially in the context of minimal clinically important differences.
A recent study showed no significant differences in AOFAS, K-P, and visual analog scale for pain between patients who underwent arthroscopic ATFL repair with or without IER reinforcement. 13 This is partially consistent with our results. Some studies support the reinforcement of IER during the arthroscopic repair of ATFL. In a retrospective study, Lee et al 24 included 30 patients with chronic ankle instability who all underwent IER reinforcement surgery. The mean follow-up time was 10.6 years, and the mean AOFAS score was 91, with only 2 patients receiving a fair result and 28 patients restored to their preinjury activity levels. At the final follow-up, the mean anterior translation values were 6.9 mm on the ipsilateral and 6.1 mm on the contralateral sides. Furthermore, the mean talar tilt angles were 3.0° on the ipsilateral side and 2.5° on the contralateral side. Pacheco et al 32 reported that concurrent injuries to both the ATFL and the CFL result in poorer clinical outcomes compared with isolated ATFL injuries.
The CFL plays a crucial role in maintaining ankle stability. Ko et al 22 reported that repairing only the ATFL with simultaneous reinforcement using the IER yielded similar clinical outcomes as repairing both the CFL and the ATFL in cases of concurrent ATFL and CFL injuries. The IER originates from the lateral surface of the calcaneus, traverses the subtalar joint, and envelops the tendons of the anterior compartment. 12 A study indicated that the anatomic vector of the IER is similar to the vector sum of the ATFL and CFL. 24 In other words, reinforcing the IER during surgery can simulate the reparative effects of the CFL. 24 The incorporation of the IER was introduced to enhance the force vector for correcting talar tilt. Therefore, when there are simultaneous injuries to both the ATFL and CFL, it is crucial to perform only ATFL repair arthroscopically with IER augment to compensate for the function of CFL. In our study, we exclusively included patients with ATFL injuries and did not include any CFL injuries. Our results demonstrated that the clinical outcomes of arthroscopic ATFL repair with or without IER augment are similar. When there is only ATFL injury, arthroscopic IER reinforcement is unnecessary.
Biomechanical studies using cadaveric models have investigated the efficacy of IER reinforcement after the Broström procedure. Aydogan et al 5 demonstrated that implementing additional IER augmentation is a technically straightforward procedure that causes minimal disruption to the surrounding anatomic structures. Moreover, it confers protective benefits to the primary ATFL repair, suggesting the potential for broader clinical applications of this augmentation technique. In several studies, researchers have utilized arthroscopically assisted IER reinforcement techniques, which have yielded favorable clinical results, particularly emphasizing the restoration of ankle joint mechanical stability in patients.3,21,30,31
On the contrary, several studies have shown that obtaining favorable postoperative outcomes can be achieved without the use of IER reinforcement. Broström 8 performed ATFL repair without IER reinforcement and observed that 58 out of 60 patients exhibited improvement or marked alleviation of symptoms. In a 26-year postoperative follow-up study of patients with chronic ankle instability who did not undergo IER reinforcement, Bell et al 7 reported that these patients experienced favorable clinical outcomes. Scranton et al 36 conducted the Broström procedure on 35 patients diagnosed with chronic ankle instability, with postoperative follow-up assessments demonstrating good outcomes (AOFAS scores, 90-91 out of 100). Additionally, Karlsson et al 19 presented an anatomic repair technique similar to the Broström procedure but without IER reinforcement. According to their 6-year follow-up results, 89% of patients achieved a good or excellent outcome.
Some biomechanical studies also do not support the use of IER reinforcement. Behrens et al 6 demonstrated that adding IER reinforcement to the traditional Broström repair did not result in significant biomechanical changes in the initial ankle joint stability, as evidenced in cadaveric models. Furthermore, they indicated that incorporating IER as an additional reinforcement during the ankle's lateral ligament complex repair might result in minor improvements during the surgical procedure. In a prior biomechanical study examining suturing methods similar to the modified lasso-loop stitch, researchers reported a strength of 150 N, comparable with that of the normal anterior talofibular ligament. 27 In another biomechanical study, Giza et al 14 concluded that reinforcing the IER does not increase strength and stiffness.
According to the existing literature,1,11 the IER can exhibit thinness and fragility in specific instances, and its anatomic attributes are not universally uniform. Several researchers have undertaken cadaveric studies to explore the anatomic structure of the IER. In their study, Dalmau-Pastor et al 12 observed that an X-shaped structure commonly characterizes the IER. However, they emphasized that the oblique superolateral band within the IER represents a weak tissue that offers limited reinforcement to ankle stability, even after augmentation. Abu-Hijleh and Harris 1 conducted an anatomic study using 14 lower limb cadaveric specimens, in which they observed the thickened bands of deep fascia over the extensor regions of the ankle, including the IER. The findings indicated considerable complexity and variability in these bands’ shape, width, and thickness. Another point of consideration is the use of IER, which deviates slightly from an anatomic repair due to its calcaneal attachment being situated 10 mm anterior to that of the CFL, potentially affecting the complete plantarflexion of the ankle. 39 Guelfi et al 16 observed that IER augmentation limited >10° of plantarflexion in 20% of cases.
Regarding complications, our study results showed no significant difference between the reinforcement and nonreinforcement groups. This conclusion requires careful consideration. The observed higher trend of overall complications in the reinforcement group (11.3%) compared to the nonreinforcement group (5.4%) raises some concerns. Additional research is essential to thoroughly examine and compare the complication rates of both surgical techniques. The intermediate dorsal cutaneous branch of the superficial peroneal nerve traverses over the IER, making it an important structure susceptible to damage during repair.2,11 Consequently, the potential for superficial peroneal nerve injury becomes a significant concern when utilizing suture passage for IER reinforcement. However, the exact relationship between IER reinforcement and the risk of nerve damage remains unclear. Of 2 previous studies using IER for augmentation, no neurologic complications were reported in one of the studies as summarized in a systematic review, 30 whereas the other showed neurologic complications in 2 of 55 patients (3.6%). 10
In addition, complications concerning the superficial peroneal nerve during all-arthroscopic repair with IER augmentation have not been consistently documented, showing incidence rates ranging from 4.54% 28 to 13.3%. 20 Among 3 studies without IER reinforcement, 2 of the studies documented no instances of neurologic complications,26,41 whereas the third study observed superficial peroneal nerve symptomatology in 1 patient (4.2%) out of 24. 42 Furthermore, IER augmentation with extracorporeal knot tying may lead to conspicuous suture knots, and the knot-tying suture anchor technique is more likely to cause knot irritation than the knotless suture anchor technique. In our included studies, some research utilized the knotless suture anchor technique, and our results demonstrated no significant difference in knot irritation rates between the reinforcement and nonreinforcement groups.16,18,25 Cao et al 9 described the modified percutaneous inferior extensor retinaculum augmentation technique, demonstrating a significant improvement in functional outcomes for patients with chronic ankle instability and a low incidence of complications. Currently, there is limited literature on the utilization of this technique, and further research involving a larger cohort of patients is needed to investigate its efficacy.
Limitations
There are some limitations to this study. First, our review only included 1 RCT and did not include more randomized controlled studies of higher methodological quality. The quality and quantity of the studies included in our analysis impose limitations on the potential value of our meta-analysis. The level of available evidence limits the value of the statistical analysis performed. This review suggests the need for conducting RCTs in a multicenter setting to obtain more definitive conclusions. Second, our study did not perform a subgroup analysis on patient weight and ligament injury severity, which may have influenced the results. Third, the meta-analysis included studies with follow-up periods of varying length, which introduces a potential source of heterogeneity. Fourth, we do not know what clinical examinations were done (tilt, anterior translation, etc) as a standardization, and there may be different postoperative protocols between the studies. These factors may affect the reliability and stability of the conclusions drawn from our systematic review and meta-analysis.
Conclusion
Based on the current evidence, our systematic review and meta-analysis suggests that arthroscopic IER reinforcement may not be necessary for achieving satisfactory postoperative outcomes in CLAI when only the ATFL is ruptured. Therefore, IER enhancement may not be required during the arthroscopic repair of ATFL for CLAI. Further research is required to investigate the impact of ligament injury severity, body weight, and concomitant CFL injuries on the results.
Footnotes
Acknowledgements
The authors extend their gratitude for the funding support provided for this study.
Final revision submitted January 16, 2024; accepted February 13, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Beijing Key Clinical Specialty Project. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.