
Abstract
Background:
Approximately 6% of people will report Achilles tendon pain during their lifetime, and one-third of these individuals will have Achilles insertional tendinopathy (AIT). For patients who have failed conservative treatment, surgical repair is performed. Achilles tendon repair can occur through various techniques, including a single-row or double-row repair.
Purpose:
To determine if there are significant advantages to double-row repair over single-row repair with respect to biomechanical and clinical outcomes.
Study design:
Systematic review; Level of evidence, 3.
Methods:
A systematic review of the literature was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. An electronic search of the EMBASE and PubMed databases was performed for all studies related to surgical treatment of AIT, which yielded 1431 unique results. These included both biomechanical and clinical studies. Clinical studies in which patients were not diagnosed with AIT, underwent surgery for repair of acute Achilles tendon rupture, or studies that included additional procedures such as a concomitant flexor hallucis longus transfer were excluded. Eligible studies were independently screened by 2 reviewers. A risk-of-bias assessment was conducted using the Cochrane Risk Of Bias In Non-randomized Studies–of Interventions and risk-of-bias tool for randomized trials tools.
Results:
A total of 23 studies were included, 4 of which were biomechanical studies and 19 were clinical studies. Biomechanical comparison found that there was a significant advantage to using double-row versus single-row fixation with respect to load at yield (354.7 N vs 198.7 N; P = .01) and mean peak load (433.9 N vs 212 N; P = .042). There was no significant difference between double-row and single-row repair with respect to load to failure. Significant heterogeneity of the studies did not allow for a statistical comparison of the clinical outcomes between double-row and single-row repairs.
Conclusion:
Although biomechanical studies favor double-row repair for AIT, the current data available on the clinical outcomes are not sufficient to determine if there is a clinical advantage of double-row repair. Larger, prospective randomized controlled trials utilizing validated outcome measures are needed to further elucidate whether the biomechanical advantages associated with double-row repair also translate into improved patient-reported outcomes.
Keywords
Achilles tendon pathology is common among athletes, active individuals, and adults who have impaired healing potential due to several different comorbidities. 24 Approximately 6% of people will report some form of Achilles tendon pain during their lifetime, and one-third of these individuals will have Achilles insertional tendinopathy (AIT). 17 Although the pathophysiology of AIT is not fully understood, degenerative changes within the Achilles insertion at the calcaneus is the hallmark of AIT. This can be associated with the formation of bone spurs and calcifications in the tendon at the insertion site, as well as enthesitis from seronegative diseases such as ankylosing spondylitis. 36
Nonoperative management of AIT involves various treatment modalities, including eccentric exercise, extracorporeal shock wave therapy, nonsteroidal anti-inflammatory medications, orthotics, laser therapy, platelet-rich plasma injections, corticosteroid injections, or sclerosant injection. 6 It is widely accepted that surgery should be considered only when conservative treatment for ≥6 months has failed or in cases of persistent pain and limitation in daily and sports activities.6,8 Debridement of the insertional portion of the Achilles tendon is the gold standard surgical treatment. 2 Once the pathologic tendon is debrided and excised, tendon reattachment is generally performed via either a single-row suture repair or a double-row suture repair. It has been hypothesized in the rotator cuff literature that double-row repair provides an advantage in restoring the anatomic footprint in larger tears 5 ; in the case of AIT, however, the decision on what type of repair to use is largely based on surgeon preference.
The purpose of this systematic review was to perform a comprehensive search of the current available literature to examine whether double-row repair provides a significant biomechanical advantage and improved clinical outcomes when compared with single-row repair for the surgical treatment of AIT. We hypothesized that the double-row technique would demonstrate a biomechanical advantage, but that this may not translate into significant improvement in clinical outcomes when compared with single-row repair.
Methods
A systematic review of the literature was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A computerized search of the EMBASE and PubMed databases was performed to identify studies involving the surgical treatment of AIT. The search was not conducted in consultation with a research librarian, and a gray literature search was not conducted. The search terms used included: “Achilles tendinopathy,”“Achilles insertional tendinopathy,”“heel pain,”“tendon repair,”“tendon reconstruction,”“Haglund deformity,”“single row repair,” and “double row repair.” Search limits included English-language studies only, with no limit to date of publication. Title and abstract screening and full-text screening was performed in duplicate by 2 independent reviewers (L.R. and S.D.), and conflicts were resolved in collaboration with the senior author (S.S.P.). Data extraction was performed using a standardized data extraction tool. Pooled mean patient age, follow-up, and outcome scores for each repair technique were calculated, and statistical significance (95% CI, 2 to –2) between the 2 repair techniques was to be assessed using an independent 2-sample t test. Heterogeneity between the studies was assessed qualitatively for categorical variables (ie, postoperative protocols) and quantitatively with independent 2-sample t tests for nominal variables such as patient age and follow-up time (alpha level = 0.05; RevMan 5.4; Cochrane). Due to significant heterogeneity in the clinical studies, statistical analysis was ultimately not performed.
Inclusion and Exclusion Criteria
The inclusion criteria were all studies that involved the surgical treatment of AIT with a single-row or double-row repair. This included both biomechanical and clinical studies. The clinical studies included in the review used either complete or partial detachment of the tendon based on the severity of the tear on a case-by-case basis. Additionally, all studies included ensured that a Haglund deformity was excised if present. The studies did not specify how a diagnosis of Haglund deformity was determined. Clinical studies in which patients were not diagnosed with AIT, underwent surgery for repair of acute Achilles tendon ruptures, or studies that included additional procedures such as a concomitant flexor hallucis longus (FHL) transfer for repair of AIT were excluded. Since most studies did not include any comorbidity data, a comment could not be made on whether patients were excluded based on comorbidities in the individual studies. Individual case reports were also excluded. If there was any ambiguity with respect to the precise surgical method used, the primary author of the study of interest was contacted for clarification, and classification was made in consultation with the senior author of the current study.
Risk-of-Bias Assessment
A risk-of-bias assessment was conducted using the Cochrane Risk Of Bias In Non-randomized Studies–of Interventions and risk-of-bias tool for randomized trials tools to assess the internal validity of the clinical studies used in the final analysis.34,35 Each of the studies was analyzed in the different domains outlined in the tools and was identified as having a low, moderate, or high risk of bias in each domain. An overall risk-of-bias assessment was assigned to each study based on the internal validity of the study in each of the domains.
Results
A total of 27 studies were identified following the literature search, with 4 biomechanical studies3,16,19,28 and 23 clinical studies †† (Figure 1). Of the 23 clinical studies, 4 studies21,32,33,38 were excluded, as they reported unique clinical outcome measures that were not used in any of the other studies. As a result, a total of 19 clinical studies ‡‡ and the 4 biomechanical studies (N = 23) remained for analysis. The characteristics of the included studies are illustrated in Table 1.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 27 diagram displaying the results of the literature search conducted.
Study Characteristics and Outcome Data a

Data are presented as mean ± SD unless otherwise indicated. AOFAS, American Orthopaedic Foot and Ankle Society Ankle-Hindfoot Score; FAAM, Foot and Ankle Ability Measure; FAOS, Foot and Ankle Outcome Score; FFI, Foot Function Index; MFS, Maryland Foot Score; N/A, not applicable; SF-36 PF, 36-item Short Form Health Survey Physical Function domain; VAS, visual analog scale.
Flexor hallucis longus transfer group not included in analysis.
Biomechanical Studies
Four biomechanical studies were identified in the final analysis (Table 2). All studies utilized fresh-frozen cadaveric specimens. Beitzel et al 3 compared load at yield and peak load, among other outcomes, in 9 sets of paired cadaveric Achilles tendons treated with single-row or double-row repair. The mean load at yield for tendons repaired with a single-row technique was 198.7 N (±39.5 N), compared with 354.7 N (±106.2 N) for tendons repaired via the double-row technique (P = .01). The mean peak load was 212 N (±49.7 N) for single-row tendons and 433.9 N (±84.3 N) for double-row repaired tendons (P = .042). 3 Kelsey et al 16 examined the load to failure for 7 cadaveric Achilles tendons repaired with a double-row suture technique and found a mean load to failure of 181.6 N (±62.8 N). 11 Lakey et al 19 assessed load to failure and ultimate failure load in 6 sets of paired cadaveric Achilles tendons. The mean load to failure was 161.2 N (±44.5 N) in single-row repaired tendons and 199.6 N (±57.4 N) in double-row repaired tendons (P = .064). The mean ultimate failure load was 344.5 N (±92.8 N) for single-row repaired tendons and 462.5 N (±94.7 N) for double-row repaired tendons (P = .066). 19 Last, Pfeffer et al 28 assessed ultimate failure load in 7 cadaveric Achilles tendons that were repaired via single-row technique, and the mean ultimate failure load was measured at 742.1 N (±187.7 N). 28
Study Characteristics and Outcome Data for the Biomechanical Studies

Data are presented as mean ± SD unless otherwise indicated. N, Newtons. Dashes indicate no available data.
Clinical Studies
A total of 17 of the 19 clinical studies included in the analysis were retrospective cohort studies. §§ The other 2 clinical studies were a case series 37 and a randomized controlled trial (RCT). 13 It is important to note that in the RCT included, patients were randomized into 2 treatment arms that included either an FHL transfer in addition to a single-row repair or solely a single-row repair. 13 Since FHL transfer was identified as an exclusion criterion, only the data reported with the single-row repair alone were included. Of the 17 retrospective cohort studies, 3 studies divided cohorts based on postoperative rehabilitation strategy, 1 age, 29 and tendon-splitting approach, 17 respectively. No study directly compared a cohort of patients who underwent single-row repair and double-row repair.
All the clinical studies reported a combination of 3 commonly used outcome scores: American Orthopaedic Foot and Ankle Score (AOFAS), visual analog scale (VAS), and 36-item Short Form Health Survey (SF-36) Physical Function domain. Fourteen out of 19 studies reported AOFAS scores, 14 out of 19 studies reported VAS scores, and 5 out of 19 studies reported SF-36 Physical Function scores.
A total of 186 patients underwent a single-row Achilles tendon repair, while a total of 349 patients underwent a double-row repair. The pooled mean patient age, follow-up, and outcome scores are shown in Table 3.
Summary of Cohort-Specific Characteristics and Clinical Outcome Scores a

Data are presented as mean ± SD unless otherwise indicated. AOFAS, American Orthopaedic Foot and Ankle Society Ankle-Hindfoot Score; VAS, visual analog scale; SF-36 PF, 36-item Short Form Health Survey Physical Function domain.
Although the data were pooled for a comparative analysis to be performed, significant clinical heterogeneity between studies did not allow for a statistical analysis. Specifically, the patient cohorts differed with regard to age (P < .01), follow-up time (P < .01), medical comorbidities (as the majority of studies failed to report comorbidity data), and utilization of differing nonstandardized postoperative rehabilitation protocols.
Risk-of-Bias Assessment
The results of the risk-of-bias assessment are displayed in Figure 2 and Figure 3. Thirteen studies (68%) were deemed to have some concern of bias (“moderate”), while 6 studies (32%) were deemed to have a high concern of bias (“serious”). 34 Most studies were deemed to have a risk of bias in the domain of confounding, as they were nonrandomized studies. Additionally, all studies were deemed to have risk of bias in the measurement of outcomes, as the design of the studies did not allow for blinding of outcome assessors. On the other hand, all studies were deemed to have a low risk of bias in classification of interventions, as the surgical technique performed for each patient was documented and explicitly defined.
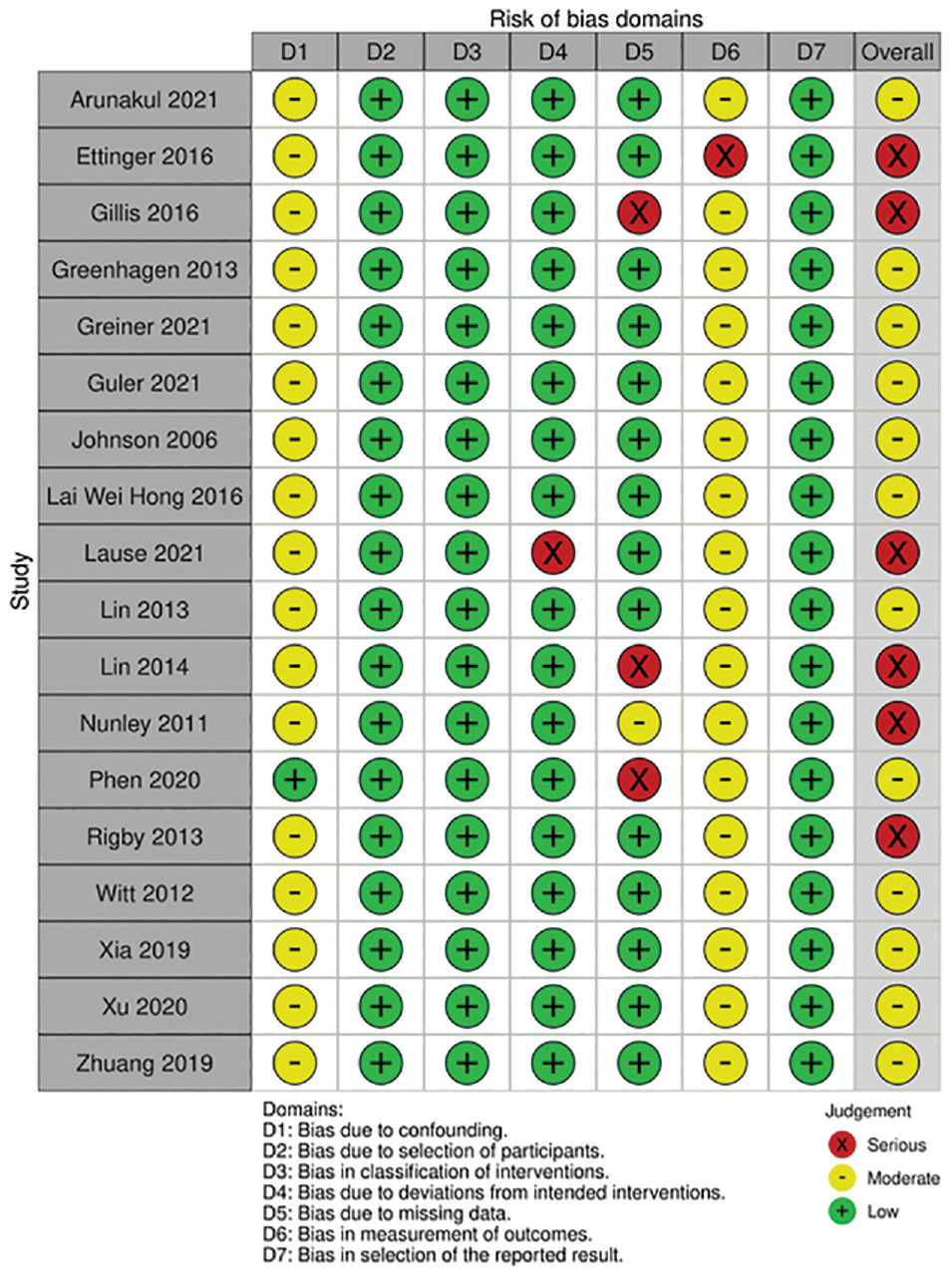
Outcomes of risk-of-bias assessment for nonrandomized clinical studies. 25

Outcomes of risk-of-bias assessment for randomized clinical study. 25
Discussion
This systematic review examined if there were advantages in biomechanical and clinical outcomes of double-row repairs over single-row repairs for AIT. Double-row repairs resulted in significantly greater mean load at yield (354.7 N vs. 198.7 N; P = .01) and mean peak load (433.9 N vs. 212 N; P = .042). 3 Double-row repairs were also associated with greater load to failure (199.6 N vs 161.2 N; P = .064) and ultimate failure load (462.5 N vs 344.5 N; P = .066); however, these findings were not statistically significant (P > .05). 19 Although the results of this systematic review found that the double-row technique is superior from a biomechanical perspective, there were insufficient scientific data to determine whether this translated to superior clinical outcomes.
The double-row repair technique has been hypothesized to generate an increased footprint and greater stability, and to provide biomechanical advantages over the single-row repair technique. 30 Beitzel et al 3 demonstrated a significant biomechanical advantage to double-row fixation when compared with single-row fixation, while Lakey et al 19 demonstrated a clear biomechanical advantage that was not statistically significant, likely due to their study being underpowered. In the study conducted by Pfeffer et al, 28 the technique that was used to measure ultimate failure load was different than that used by Kelsey et al and Lakey et al, and as a result, these findings could not be compared against one another. It is also important to note that the cadavers used in the biomechanical studies were not from patients with AIT exclusively. So far, there has not been any study that has examined whether the same biomechanical findings would hold true in degenerate, tendinopathic cadaveric specimens.
Despite a demonstrated biomechanical advantage of double-row repairs for the surgical management of AIT, this review could not determine if there were similar advantages seen in the clinical outcomes. A comparative statistical analysis could not be performed due to the limitations of the current literature. Significant heterogeneity was seen across the studies. For instance, standardized postoperative protocols were not followed, but rather patients were placed in protocols based on the standard practice at the respective institutions. The risk-of-bias assessment also showed significant deficiencies in the current clinical data. Thirteen (68%) of the clinical studies were found to have a moderate risk of bias, while 6 (32%) were found to have a serious risk of bias. All studies except one 29 failed to report any comorbidity data on the patients assessed in their respective studies, and due to the designs of the studies included, outcome assessors were not blinded to intervention status in any of the studies. The study by Rigby et al 31 was flagged as having a serious risk of bias for a unique reason, as the secondary authors of the study were paid consultants for the company that manufactured the bone anchors and sutures used in the study. This potential conflict of interest was declared by the study authors.
It should be noted that the biomechanical advantage of double-row repair techniques does not necessarily translate into improved clinical outcomes. This is exemplified in the rotator cuff literature. Chen et al 5 performed a systematic review and meta-analysis of the clinical outcomes of single-row versus double-row rotator cuff repair and found that although the double-row repair provided a significantly greater rate of intact tendon healing compared with single-row repair, this benefit did not translate into clinically confirmed functional improvement. Another meta-analysis performed by Ponugoti et al 30 had similar findings and reported that there was no significant difference between single-row and double-row repair techniques for full-thickness rotator cuff tears in any of the observed outcomes they assessed. Unfortunately, the significant heterogeneity of the data in the current Achilles literature did not allow for comparison of the clinical outcomes of patients undergoing single-row repair versus double-row repair for AIT. As such, the clinical advantages of double-row repair in AIT remain unclear.
Another important observation noted in this systematic review that merits discussion is the lack of use of validated scores when assessing functional outcomes in patients undergoing surgery for AIT. The VAS and SF-36 scores are nonspecific to Achilles tendon pathology. Additionally, although the AOFAS questionnaire is widely used for the evaluation of hindfoot pathology, it has not been shown to be a validated score and some authors have raised concerns about its association to the SF-36. 4 Furthermore, the AOFAS questionnaire is not specific to the Achilles tendon. The most specific and thoroughly validated score to assess Achilles tendon pathology is the Victorian Institute of Sport Assessment for Achilles (VISA-A). This score specifically focuses on symptoms and function of the Achilles tendon, investigating the influence that these features may have on gait and normal habits. 15 None of the 19 clinical studies assessed in this review utilized the VISA-A score, despite the consensus of its validity in assessing patients with Achilles tendon pathology. With that, there may be merit in conducting prospective comparative studies using the VISA-A score to more accurately assess if there is a clinical difference or advantage of double-row repairs over single-row repairs.
The key strengths of this review include the comprehensive and rigorous search and article screening process, as well as a clearly stated objective to answer a focused question of clinical relevance. Although there has been a handful of narrative reviews published about the management of AIT, this review expands on the current literature by addressing a relevant issue with respect to the surgical management of patients with AIT. Another strength of this review is that it highlights where the gaps in the current literature surrounding the surgical management of AIT exist and proposes a recommendation as to how those gaps could potentially be addressed.
Overall, the lack of comparative studies and great heterogeneity of confounding factors across studies in the literature are the main limitations when assessing the significance of the results of this systematic review. In addition, all studies included in this review were deemed to have some threat to internal validity, thereby affecting the quality of the evidence presented in this review. Another key limitation to this review is the fact that the outcome measures used to determine the effect size were all nonvalidated and nonspecific to Achilles tendon pathology, thereby raising concerns about the external validity of the findings of this review.
Conclusion
Although there may be a biomechanical advantage to double-row repair in the surgical management of AIT, the translation of this biomechanical advantage into clinically significant outcomes remains unclear. Therefore, further research, particularly with comparative studies and RCTs using validated outcome scores such as the VISA-A, is warranted to establish if there is a superior surgical technique in the surgical management of patients with AIT.
Footnotes
Final revision submitted November 9, 2023; accepted February 2, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.S.P. received a fee for speaking and for organizing an educational program (DePuy Synthes). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.