
Abstract
Background:
Concussions make up a significant proportion of sports injuries. This study aimed to describe the mechanisms of injury and associated symptoms of pediatric patients diagnosed with concussions (age range, 4-17 years) from contact sports.
Hypothesis:
Mechanisms of injury would differ based on sex and age, with female athletes and younger athletes aged 4 to 11 years sustaining fewer concussions from player-to-player contact.
Study Design:
Descriptive epidemiology study.
Methods:
The National Electronic Injury Surveillance System was queried for all contact sport concussions presented to United States emergency departments. The sports analyzed included basketball, football, soccer, hockey, rugby, and lacrosse. Descriptive data, mechanisms of injury, and associated symptoms were analyzed for each sport. Differences in the number of concussions sustained by year and sport, the severity of the injury, and associated symptoms were compared using chi-square test, and differences in proportion were calculated for mechanisms of injury stratified by sex and age.
Results:
A total of 12,602 youth athletes sustained concussions between 2012 and 2021. Most patients were male (78.5%), with a mean age of 13.48 years. Football concussions were the most common, with 45.32% of the concussions. The mechanism of injury was largely sport-specific, with player-to-player contact the most common overall. Older male athletes were more likely to have concussions from player-to-player contact, whereas younger athletes were more impacted by head-to-ground mechanisms. Symptom presentation was not sport-specific, and headache and dizziness were the most common presentation at 41.2% and 26.2%, respectively.
Conclusion:
The most important overall mechanism of injury was player-to-player contact, especially in older male youth athletes, whereas younger athletes were more likely to be concussed due to head-to-ground injuries.
Keywords
Concussions make up a significant proportion of contact sports injuries among youth athletes.24,26 The long-term effects. are not fully understood in young athletes, and the potential consequences of mismanagement, reinjury, or misdiagnosis are significant. 31 With significant future implications for youth athletes and increased prevalence, there is heightened concussion awareness in youth contact sports.
Youth team contact sports, such as football, hockey, rugby, lacrosse, basketball, and soccer, are popular among young people and are the leading cause of concussions. 2 There have been varying reports of incidence rates for sports-related concussions in youth; nonetheless, sports with a higher degree of physical contact have higher rates than noncontact sports.22,32 Currently, most studies of youth concussions focus on descriptive data and incidence rates.1,7,10,25 These studies have indicated that there are sex- and age-specific differences in incidence rates among youth concussions, with females having higher rates than males. 30
However, little research has looked at specific mechanisms of injury in youth contact sports. Several mechanisms of injury can contribute to a concussion, whether it is related to mechanical trauma after contact with another person or object or repetitive subconcussive trauma. 8 It remains unclear how concussion mechanisms of injury differ among children and adolescents based on sport, age, and sex. This gap is important because concussion diagnosis often carries specific, state-based regulations regarding return-to-play criteria relevant to sports-related mechanisms. 35 Furthermore, understanding the circumstances and mechanisms of injury can provide insights for targeting intervention efforts.
Our objective was to provide a comprehensive epidemiological analysis of mechanisms of injury for concussions using a nationwide database. The utility of studying mechanisms of injury for pediatric concussions in a large national database is that it provides an opportunity to understand the entire spectrum of sports-related concussions and identify and implement preventative strategies.10,25 To accomplish this objective, we aimed to (1) categorize the broad mechanisms of injury for contact sports concussions sustained by youth 4 to 17 years old; (2) assess how variables including age, sex, and sport impact mechanisms of injury; and (3) describe the number of sports-related concussions by sport and describe associated symptoms of concussion. We hypothesized that both sex and age would have unique differences in mechanisms of injury in youth concussions.
Methods
All data were collected using The United States Consumer Product Safety Commission National Electronic Injury Surveillance System (NEISS) between January 2012 and December 2021. The NEISS database is a nationally representative probability sample of 100 emergency departments in the United States and its territories. All participating NEISS hospitals have at least 6 beds and a 24-hour emergency department where information on descriptive data, injury, and treatment information is collected. From data collected by the NEISS hospitals, national estimates are made of the total injuries treated in US emergency departments. 11
The NEISS database was queried for all concussions (injury code: 52, location code: 75) in athletes 4 to 17 years old related to team contact sports—including basketball, football, hockey, lacrosse, rugby, and soccer using the respective product codes 1205, 1211, 3272, 1215, 3234, and 1267. Information on descriptive data, injury sustained, diagnosis, and narrative describing how the injury occurred and how the patient presented to the emergency department was collected. Our analysis included information on the mechanism of injury and associated symptoms collected from the narrative section. Two separate authors (A.G. and M.A.) independently coded mechanisms of injury and related symptoms, with a third author resolving (JJC) any discrepancies. All injuries were filtered for injuries that occurred at school or a place of recreation to capture injuries sustained in an organized sports setting. Any data points that did not include mechanisms of injury were excluded from the analysis.
Data Analysis
Descriptive analysis was performed for each year and stratified by sport. Mechanisms of injury were stratified based on the 5 mechanisms of injury as follows: (1) player-to-player; (2) head-to-ball; (3) head-to-ground; (4) head-to-other object; and (5) unspecified. Loss of consciousness (LOC) and associated symptoms were collected based on the narrative provided for each case. Differences in the number of concussions sustained by year and sport, the severity of the injury, and associated symptoms were compared using chi-square test, with an alpha of .05 indicating statistical significance. Differences in proportion were calculated for mechanisms of injury with further stratification by sex and age-group (age, 4-11 years and 11-17 years) using the chi-square test for proportions. All statistical analyses were performed using R Studio Version 4.01.
Results
The total number of concussion cases between 2012 and 2021 in the NEISS database was 73,940. After excluding concussed patients for reasons outside of contact sports, the total number of athletes aged 4 to 17 years was 12,602. Concussions sustained by male athletes (9889 [78.5%]) made up a significant proportion of the total concussions, and the mean age was 13.48 years (Table 1). There were significantly fewer concussions in athletes aged 4 to 11 years than in older athletes aged 11 to 17 years (P < .001).
Descriptive Data Stratified by Sport 2012-2021 a
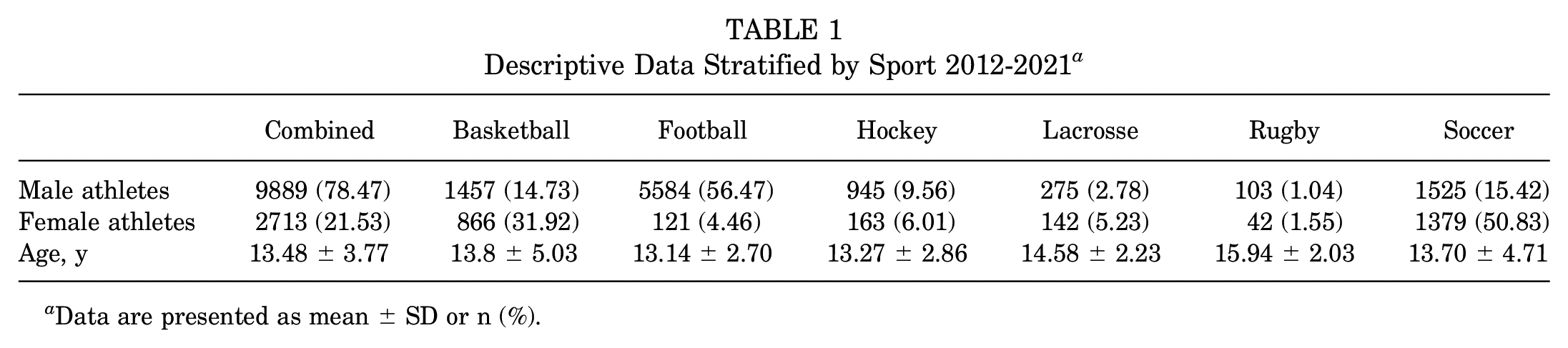
Data are presented as mean ± SD or n (%).
Football made up the greatest number of concussions across all years, with a total of 5705. The next most common was soccer (n = 2904), followed by basketball (n = 2323) and hockey (n = 1108). Among female athletes, soccer was the most common cause of concussion, followed by basketball (Figure 1). Rugby and lacrosse had the smallest number of concussions in this time frame, with 145 and 407, respectively (Figure 1). A significantly smaller number of concussions was found between 2020 and 2021 compared with 2012 and 2019 in all sports analyzed (Figure 2).

Sex distribution of pediatric concussions in pediatric contact sports between 2012 and 2021.

The number of pediatric concussions per year presenting to United States NEISS, with significant decreases in 2020 and 2021. NEISS, National Electronic Injury Surveillance System.
Mechanism of Injury
Overall, the most common mechanism of injury was player-to-player contact, with 6543 (51.9%) concussions. Player-to-player contact was the most frequent mechanism of injury in football, rugby, and soccer. Head-to-ground was the most common mechanism of injury in basketball and hockey. The head-to-other object made up a significant proportion of injuries in lacrosse and hockey (Figure 3).

Sport-specific mechanism of injury in pediatric contact sports between 2012 and 2021.
When stratified by sex, female athletes were significantly less likely to sustain concussion by player-to-player contact in soccer (P = .014) and football (P = .0012) (Table 2). However, female athletes were significantly more likely to sustain a concussion due to the mechanism of ball-to-player than male athletes (P = .002) in soccer and head-to-ground in football (P = .02) (Table 3).
Mechanism of Injury Stratified by Sport and Sex for Pediatric Concussions in Contact Sports 2012-2021 a

Data are presented as n or n (%). The percentage represents the percentage of participants experiencing varying mechanisms of injury within each sport. This breakdown provides insight into the distribution of injury mechanisms among sexes across different sports.
Mechanism of Injury Stratified by Sport and Age-Group for Pediatric Concussions in Contact Sports 2012-2021 a

Data are presented as n or n (%). The percentage represents the percentage of participants experiencing varying mechanisms of injury within each sport.
When stratified by age, young athletes aged 4 to 11 years were significantly less likely to be concussed due to player-to-player contact in soccer (P = .024) and basketball (P = .004). Athletes aged 4 to 11 years were significantly more likely to have head-to-ground concussions in soccer (P = .021), hockey (P = .007), and basketball (P = .006).
Injury Characteristics
Overall, 857 (6.8%) of concussions led to LOC, with football making up a significant proportion of these concussions (361 [42.1%]) (Table 4). Soccer had 206 concussions with LOC, followed by basketball with 140. Rugby made up the lowest percentage of total concussions but reported the highest rate of LOC at 19.3%. Basketball had the lowest rate of LOC at 2.5%.
Treatment Location and LOC Information a
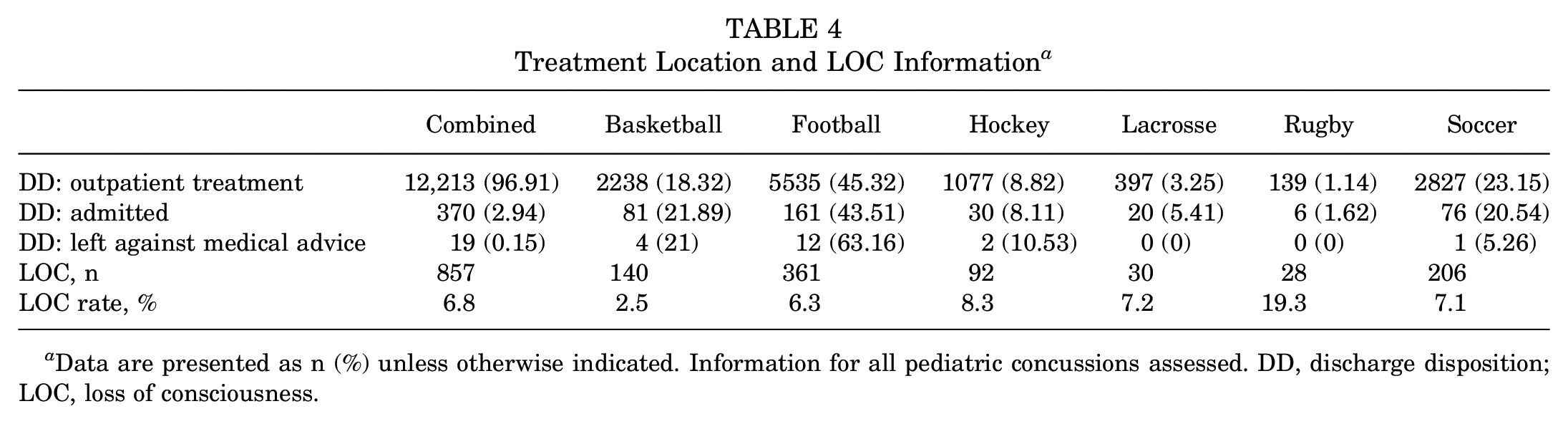
Data are presented as n (%) unless otherwise indicated. Information for all pediatric concussions assessed. DD, discharge disposition; LOC, loss of consciousness.
Severe injuries defined by admission to the hospital were rare, with only 370 (2.94%) of concussions requiring hospital admittance. Football made up a significant proportion of these 161 (43.51) followed by soccer 76 (20.54) (Table 4). Outpatient treatment was the most common discharge disposition among the athletes (12,213 [96.9%]).
Associated Symptoms
The most common associated symptoms reported in pediatric concussions were headache (793 [41.2%]) and dizziness (504 [26.2%]). Regardless of sport, headaches and dizziness were the most associated symptoms. Nausea and contusions/bruising were also common symptoms (Table 5). Vomiting, blurred vision, altered mental status, and lethargy were also cited as associated symptoms.
Sport-Stratified Presentation of Symptoms in Concussion a
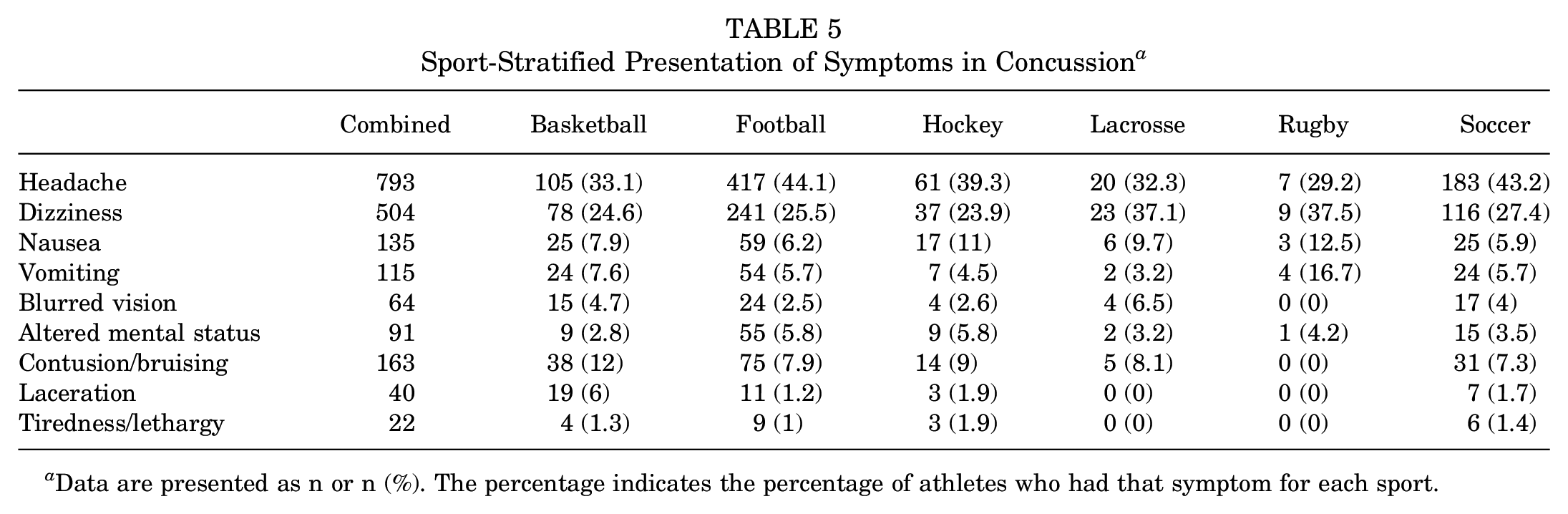
Data are presented as n or n (%). The percentage indicates the percentage of athletes who had that symptom for each sport.
Discussion
Our findings indicated that the mechanism of injury in pediatric concussions varies depending on age and sex. The most important overall mechanism of injury was player-to-player contact, especially in older male athletes, and younger athletes were more likely to be concussed due to head-to-ground injuries. Furthermore, head-to-ball mechanisms of injury were more common in female than male athletes.
In older males (age, 11-17 years), player-to-player contact was the most significant mechanism of injury. These differences may have been due to differences in playing style, where males are more likely to have an aggressive and rough style of play compared with females. 27 Furthermore, older athletes are bigger and stronger with more intense gameplay and greater contact forces. 19 Our findings are consistent with those of other studies using alternative surveillance methods from athletic trainers’ data, high school reporting information in online databases, and hospital databases.21,29 We recommend giving priority to player-to-player contact when developing preventative strategies because it is the most common mechanism of injury in pediatric sports. These strategies include rule changes that prohibit high-risk contact, such as helmet-to-helmet contact in football and body checking in soccer and hockey.14,15 In addition to new rule changes, increasing emphasis should be placed on player education from a young age. 16
Concussions due to player-to-player contact were less prevalent in athletes aged 4 to 11 years; therefore, mechanisms including head-to-ground are more important to consider in preventative strategies. Previous studies indicated that younger youth athletes are more likely to experience head-to-ground injuries, which may be caused by biological differences in younger athletes compared with adolescent athletes.9,27 These biological differences include decreased neck strength, head size, head-neck length, and balance differences that reduce younger athletes’ ability to withstand external forces and increased displacement when contacting the ground.13,23
Our study presented an update to current knowledge on the epidemiology of concussions on a nationwide scale and looked at trends over time for pediatric concussions in addition to common symptom presentation. Our study indicated that football accounted for the greatest number of concussions between 2012 and 2021, unchanged from previous years.4,7,19,26,29,33 Sports—including soccer, wrestling, and basketball—have the second largest number of concussions, but the specific ranking of these sports varies among studies7,19,26,29,33 and by sex.
Across all the sports analyzed, no unique pattern in symptom presentation was found, regardless of sport. Concussions can present with a wide array of symptoms that can range from nonspecific findings to LOC. In the pediatric population, headache has been noted as the most common symptom that patients with a concussion will experience, and this was supported by our data.6,12 In addition to headaches, dizziness, head bruising, contusion, and nausea are other common symptoms in pediatric patients.4,12,20,28 The overall rate of LOC found in this study was similar to that in other studies.3,18 However, we reported a much higher rate of LOC in rugby than all other sports, with a rate of 19.3%, similar to rates reported in elite athletes and warrants further study. 5
There was a statistically significant decrease in the incidence of concussion between 2020 and 2021 compared with 2012 and 2019 (P < .001). The significantly smaller number of patients who presented to the emergency department for a concussion between 2020 and 2021 could be attributed to the COVID-19 pandemic. During that time, social restrictions were put in place that prohibited in-person learning and many extracurricular activities. With a decrease in athletic events, including practices and games, there were likely fewer high-risk situations that would have resulted in player injury.17,34 Further research needs to identify whether the decrease in the number of concussions reported by emergency departments was due to a decreased number of concussions sustained or patients with concussions being less likely to seek medical care due to social restrictions from COVID-19. We hypothesize that both occurred, which may indicate a portion of youth athletes with concussions not receiving proper medical care. 34
Limitations
Although this study highlights the common injury mechanisms, symptoms, and situational information regarding pediatric concussions among 6 different contact sports, there are limitations. This retrospective study relies on self-reported injury mechanisms and symptoms, which may not capture all relevant information regarding the injury and associated symptoms. Furthermore, variability in documentation among different emergency departments means not all charts contain each data point. Finally, the population is also limited, as we could only analyze patients who presented to the emergency department and we had no information on discharge instructions and discharge disposition. Some patients may see an alternative provider other than an emergency department physician, or they may not seek medical attention at all. It is possible that patients who did present to the emergency department had more severe concussions with a greater number of symptoms.
Conclusion
The most important overall mechanism of injury was player-to-player contact, especially in older male youth athletes, whereas younger athletes were more likely to be concussed due to head-to-ground injuries. Addressing player-to-player contact presents the greatest potential when developing preventative strategies, including rule changes to limit illegal and high-risk contact, better rule enforcement, and adequate education in proper technique for young athletes.
Footnotes
Final revision submitted November 11, 2023; accepted February 12, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: V.W. has received education payments from Arthrex and Reel Surgical; nonconsulting fees from Arthrex; and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Central Florida (ref No. STUDY00005122).