
Abstract
Background:
Differences in rotational range of motion (ROM) compared to humeral retrotorsion (HRT)–corrected rotational ROM exist in healthy baseball athletes, but it is unclear whether these differences exist in a pathological population.
Purpose/Hypothesis:
The purpose of this study was to determine if there are disparities between objectively measured differences in ROM and HRT-corrected deficits in injured baseball players. It was hypothesized that disparities would exist between (1) the side-to-side difference in glenohumeral external rotation (GER) and the HRT-corrected glenohumeral external rotation deficit (GERD) and (2) the side-to-side difference in glenohumeral internal rotation (GIR) and the HRT-corrected glenohumeral internal rotation deficit (GIRD).
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Data from 172 baseball players with shoulder or elbow injuries (45 shoulder, 127 elbow) were reviewed in July 2023. GER and GIR were measured on the injured and noninjured sides of all players, and diagnostic ultrasound was used to measure HRT. Dependent t tests were run to compare the side-to side differences in GER and GIR with the HRT-corrected GERD and GIRD, respectively.
Results:
In the players with a shoulder injury, there was a significant disparity between the side-to-side difference in GER and the HRT-corrected GERD (2°± 14° vs −13°± 15°, respectively) and between the side-to-side difference in GIR and the HRT-corrected GIRD (–14°± 8° vs 2°± 9°, respectively) (P < .001 for both). Similarly, players with an elbow injury had significant disparities between the side-to-side difference in GER and the HRT-corrected GERD (6°± 9° vs −10°± 9°, respectively) and between the side-to-side difference in GIR and the HRT-corrected GIRD (–12°± 8° vs 4°± 10°, respectively) (P < .001 for both).
Conclusion:
The results supported our hypothesis that there were disparities between objectively measured differences in GER and GIR compared with the HRT-corrected GERD and GIRD in injured baseball players. Consideration must be given to osseous adaptations that occur at the glenohumeral joint when evaluating and treating this population.
The throwing motion in baseball elicits large torques across the shoulder and elbow. 8 The supraphysiological demands required during the throwing motion render baseball athletes susceptible to shoulder and elbow injuries across different levels of baseball participation.1,18,26 An increase in shoulder and elbow moments during overhead throwing has been found to be associated with alterations in the clinical objective profiles of baseball athletes. 14 Biomechanical studies conducted on overhead throwing have shown excessive motion and torques, leading researchers to appreciate anatomic adaptations in the shoulder of the baseball athlete, including osseous, capsular, and soft tissue alterations.2,5 These adaptations of the shoulder in baseball athletes often manifest clinically as an increase in humeral retrotorsion (HRT), an increase in glenohumeral external rotation (GER) range of motion (ROM), a decrease in glenohumeral internal rotation (GIR) ROM, and a decrease in total range of motion (TROM) in the throwing arm compared to the nonthrowing arm (ie, side-to-side difference).2,5 While these adaptations may be normal, effort has been put into determining when these throwing adaptations raise concerns so that health care professionals treating these athletes know whether to restore GER or GIR.
Previous researchers have investigated glenohumeral rotational motion and identified clinical ROM thresholds that may contribute to shoulder and elbow abnormalities.19,24,27,28,37,38 Studies have shown that side-to-side differences in GIR of between 13° and 25°,27-29,37 in GER of <5°, 37 and in TROM of >5° may increase the risk of shoulder injuries in baseball players. 38 Additionally, differences in shoulder rotational motion have been associated with elbow injuries in high school, collegiate, and professional players.9,36 However, these objective ROM risk factors do not account for osseous anatomic adaptations (ie, HRT). Recent research suggests that the bony adaptation of HRT explains up to 65% of GIR ROM, 13 further indicating the importance of considering osseous adaptations when interpreting shoulder rotational motion.
Humeral torsion describes twisting about the long axis of the humerus, 6 and it is specifically defined as the angular difference between the orientation of the axis of the proximal humeral head and the epicondylar axis at the distal humerus. 17 In the throwing arm of baseball players, it is common for humeral torsion to present itself as HRT when the humeral head is oriented in a more posteromedial direction relative to the nonthrowing arm.5,35 Understanding the clinical implications of HRT is an important consideration in the care of baseball athletes, as previous studies have suggested that HRT could be an injury risk factor.20,34 At birth, both humeri are in a marked position of HRT, as represented by a large angle between the proximal humeral head and the epicondylar axis at the distal humerus. 7 During development from childhood to adolescence, a remodeling process occurs along the shaft of the humerus, resulting in less retrotorsion (smaller angle between the proximal humeral head and the epicondylar axis at the distal humerus).7,17 However, throwing by a skeletally immature athlete will delay the natural derotation process in the throwing arm. 10 This, in turn, leads to a side-to-side difference in HRT measurements (termed “relative HRT” in this study). The bony adaptation of HRT is likely to develop when throwing during the skeletal maturation process and influences shoulder ROM.24,32 Consequently, side-to-side differences in HRT are often present in baseball players. When researchers correct for relative HRT within the objective measurements of rotational motion, a shift in rotational deficits occurs. Thus, a glenohumeral internal rotation deficit (GIRD) does not always exist, and instead, a glenohumeral external rotation deficit (GERD) is more commonly present.22,25,33 These shifts in ROM have been documented in populations of healthy baseball players22,25,33; however, it is currently unknown if these same trends in ROM persist after correcting for HRT in a pathological population.
It is important to understand true glenohumeral rotational deficits so that appropriate interventions can be implemented to combat shoulder rotation loss that may become pathological. The purpose of this study was to determine whether disparities exist between (1) the side-to-side difference in GER and the HRT-corrected GERD and (2) the side-to-side difference in GIR and the HRT-corrected GIRD in baseball players with a shoulder or elbow injury. We hypothesized that there would be significant disparities between objectively measured differences in GER and GIR compared to the HRT-corrected GERD and GIRD in this population.
Methods
Study Design
The protocol for this study was approved by our institutional review board, and all participants signed an electronic informed consent/assent form before study enrollment. Data for this study were retrospectively obtained from a single-surgeon database within a multisurgeon prospective clinical data registry. Prospective data collection started on March 10, 2022, and is currently ongoing. To answer these specific research questions, data were exported on July 20, 2023. All data were collected during the participant's initial visit using REDCap (Research Electronic Data Capture). REDCap is a secure, web-based platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture, (2) audit trails for tracking data manipulation and export procedures, (3) automated export procedures for seamless data downloads to common statistical packages, and (4) procedures for data integration and interoperability with external sources.11,12
Study Participants
We reviewed the records of injured baseball players who reported either a shoulder or elbow injury to a single surgeon in the clinical registry. Athletes were included if (1) they were unable to participate in baseball with a primary complaint of shoulder or elbow pain in the throwing arm and (2) they were between the ages of 9 and 24 years. The age range selected for study inclusion was set to accommodate athletes at the youth, high school, and collegiate levels of play: 9 years reflects the age at which observable differences in humeral torsion become apparent, and 24 years covers a normal 4-year course of play for collegiate athletes, expanded to accommodate those who had extra years via redshirt, graduate transfer, and COVID-19. Participants were excluded if they reported both a shoulder injury and an elbow injury, bilateral shoulder or elbow pain, or an injury in the nonthrowing arm.
Included were 172 players: 45 players with shoulder injuries and 127 players with elbow injuries. All participants began competing in baseball at a young age when the effects of humeral torsion on the throwing arm were high (mean age, 6 ± 2 years).16,23,30
Clinical Evaluation
All participants reported to our outpatient sports medicine clinic for a clinical evaluation by a board-certified, fellowship-trained, orthopaedic surgeon (J.E.C.). Patient characteristics as well as objective measurements of shoulder rotational ROM and HRT were collected during this initial evaluation before the development of a plan of care by the surgeon. Objective measurements of GIR, GER, and HRT were obtained by 2 examiners (N.L.M. and S.M.K.). The examiners were not blinded to the throwing arm in this study.
Before data collection, the interrater reliability for each of the 3 measurements was established. The intraclass correlation coefficients (ICCs) with 95% CIs and standard errors of measurement (SEMs) were calculated for objective GIR (ICC2,1 = 0.96 [95% CI, 0.81-0.99]; SEM = 1.05°), objective GER (ICC2,1 = 0.96 [95% CI, 0.86-0.99]; SEM = 1.30°), and HRT (ICC2,1 = 0.94 [95% CI, 0.85-0.97]; SEM = 1.96°) and were found to be excellent.
GIR and GER
Objective GIR and GER were assessed passively in both arms utilizing a digital inclinometer, as similarly described by Wilk et al. 39 Participants were placed supine on a treatment table in a hook-lying position with the legs set on a bolster to promote comfort. A rolled towel was placed under the participant's humerus to maintain a scapular position in the coronal plane for standardization of testing. Examiner 1 stood at the head of the participant while moving the arm into 90° of shoulder abduction and 90° of elbow flexion and also stabilizing the scapula. The scapula was stabilized by grasping the coracoid process anteriorly and the spine of the scapula posteriorly for both GIR and GER. 39 Examiner 1 determined the ROM for GIR and GER from the first point of scapular movement, and examiner 2 utilized a digital inclinometer to document the measurement, aligning the inclinometer just below the shaft of the ulna. The inclinometer was zeroed to the vertical plane before the measurement. For each participant, GER was measured first, followed by GIR. Each motion was measured twice, and the mean of the 2 values was used for final analysis (Figure 1). If there was a wide discrepancy in the 2 measurements (>3°), a third measurement was performed to ensure consistency.
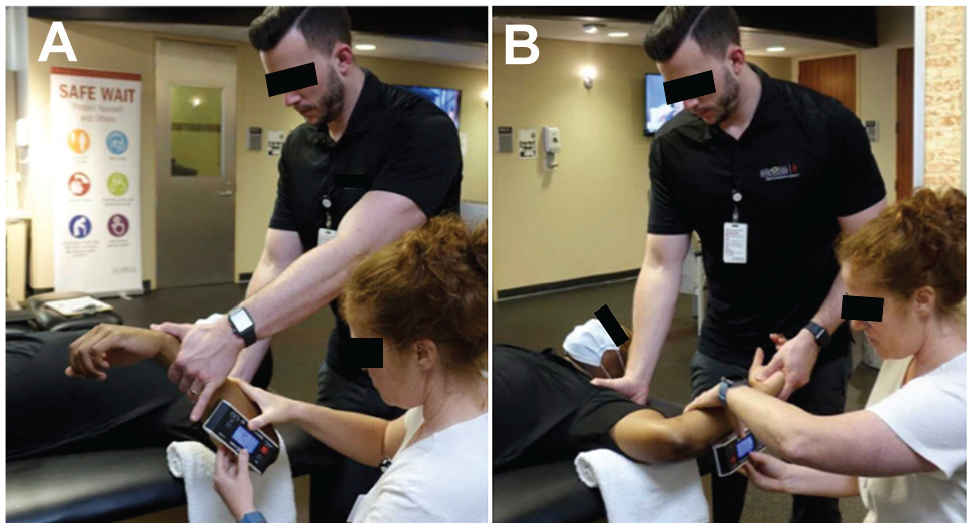
Measurement of objective (A) glenohumeral internal rotation and (B) glenohumeral external rotation.
Humeral Retrotorsion
HRT was assessed utilizing an indirect ultrasonographic technique described 24 and validated by previous researchers. 21 Each participant was placed supine in a hook-lying position on a standard treatment table with the legs set on a bolster. Ultrasound gel (Cardinal Health) was placed on a straight ML16-15 probe connected to a Venue Go R3 (GE HealthCare) ultrasound machine. Examiner 1 placed the participant's shoulder at 90° of abduction with the elbow at 90° of flexion and positioned the probe over the anterior aspect of the participant's glenohumeral joint. A rolled towel was placed under the participant's humerus to maintain the scapula in the coronal plane. The probe was aligned perpendicular to the long axis of the humerus in the frontal plane. With the probe level (as designated by a bubble level on the face of the probe), examiner 1 rotated the humerus until the deepest part of the bicipital groove was visualized and the apexes of the greater and lesser tuberosities were parallel to the horizontal plane (Figure 2). Examiner 1 then asked examiner 2 to place the digital inclinometer just below the shaft of the ulna and record the degrees of inclination. The digital inclinometer was zeroed to the vertical plane before the measurement. This process was repeated in both arms. The mean of the 2 values was used for final analysis; a third measurement was performed if there was a wide discrepancy (>3°) between the first 2 measurements.

(A) Measurement of humeral retrotorsion using a linear ultrasound probe placed over the anterior shoulder, and (B) visualization of the deepest portion of the bicipital groove while the lesser and greater tuberosities remained parallel.
Data Reduction
The raw data for both objective GIR and GER as well as HRT were reduced. Calculations utilized in this study were adapted from previous research 25 and are described in Table 1. It is important to note that the injured arm always represents the throwing arm in this study. When interpreting relative HRT, a negative value indicates greater HRT in the injured (throwing) arm compared to the noninjured (nonthrowing) arm. In addition, when interpreting the HRT-corrected GIRD and GERD, a negative value indicates a deficit, while a positive value indicates greater motion in the injured arm.
Calculations for GIR, GER, and HRT a

GER, glenohumeral external rotation; GERD, glenohumeral external rotation deficit; GIR, glenohumeral internal rotation; GIRD, glenohumeral internal rotation deficit; HRT, humeral retrotorsion; ROM, range of motion; TROM, total range of motion.
Statistical Analysis
Post hoc power analysis was performed using G*Power (Version 3.1) with power set at 0.80 (1 –b) and an alpha level of .05 (2-tailed). The effect size was calculated using the means and standard deviations of objective side-to-side differences in GER and the HRT-corrected GERD from the elbow injury group (n = 127). This revealed an acceptable calculated power of 1.00 for our study.
To confirm the study hypothesis, 4 dependent t tests were utilized. The independent variables were the elbow and shoulder injury groups. The dependent variables consisted of objective differences in GIR and GER as well as the HRT-corrected GIRD and GERD. All assumptions were met, and all data were analyzed using statistical software SPSS (Version 29; IBM). Cohen d effect sizes were estimated for each pairwise comparison, with values interpreted as small (0.2), moderate (0.5-0.6), or large (0.8-1.0). 4 P < .05 was considered significant for all statistical analyses.
Results
The characteristics of the 172 players according to injury group are documented in Table 2, and playing experience and participation times are summarized in Table 3. The diagnoses documented by the primary physician (J.E.C.) during the initial encounter are shown in Appendix Table A1. Overall, 61 players (10 with a shoulder injury, 51 with an elbow injury) underwent a surgical intervention after the objective measurements and initial evaluation.
Participant Characteristics (n = 172) a
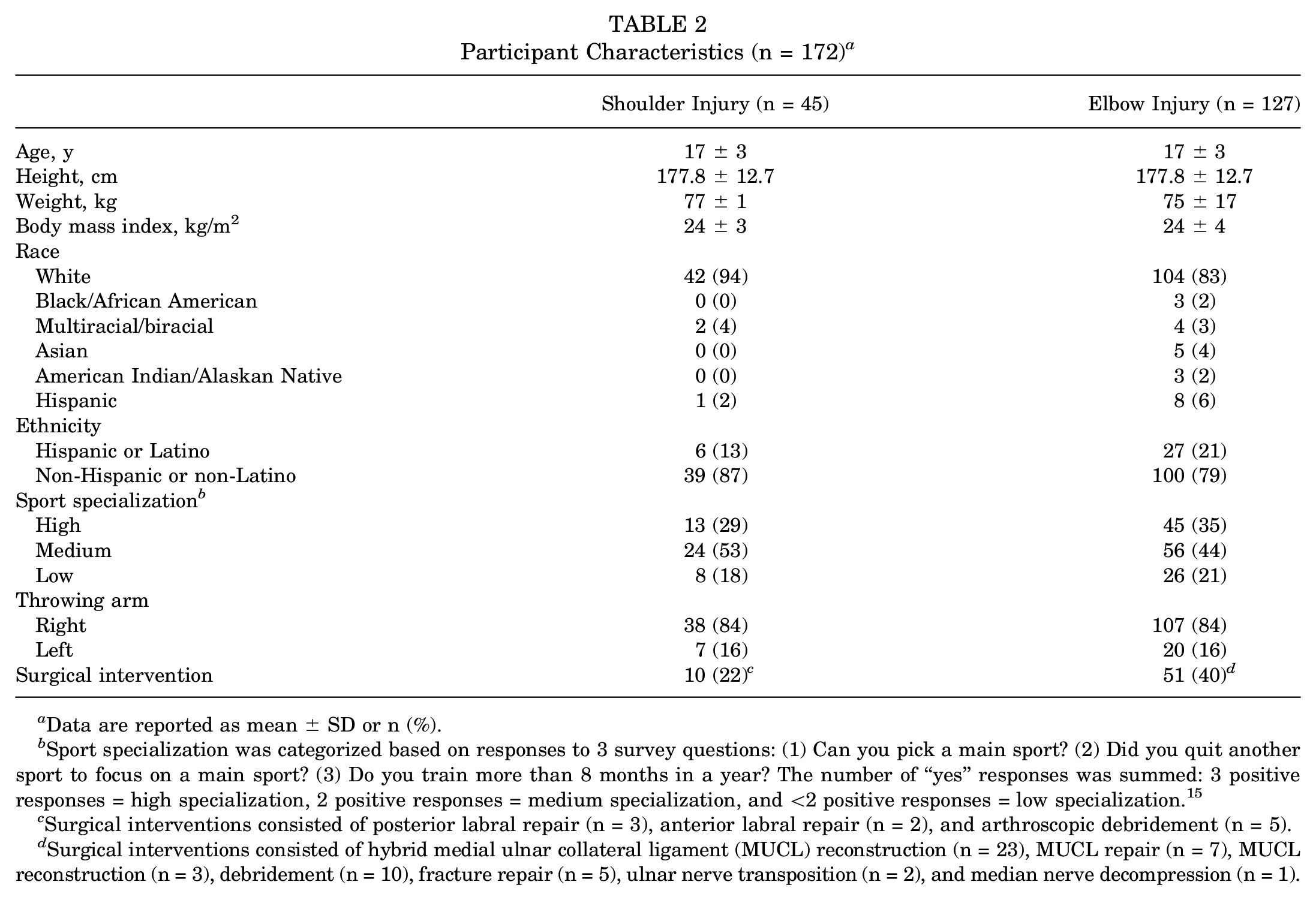
Data are reported as mean ± SD or n (%).
Sport specialization was categorized based on responses to 3 survey questions: (1) Can you pick a main sport? (2) Did you quit another sport to focus on a main sport? (3) Do you train more than 8 months in a year? The number of “yes” responses was summed: 3 positive responses = high specialization, 2 positive responses = medium specialization, and <2 positive responses = low specialization. 15
Surgical interventions consisted of posterior labral repair (n = 3), anterior labral repair (n = 2), and arthroscopic debridement (n = 5).
Surgical interventions consisted of hybrid medial ulnar collateral ligament (MUCL) reconstruction (n = 23), MUCL repair (n = 7), MUCL reconstruction (n = 3), debridement (n = 10), fracture repair (n = 5), ulnar nerve transposition (n = 2), and median nerve decompression (n = 1).
Baseball Playing Experience and Participation (n = 172) a
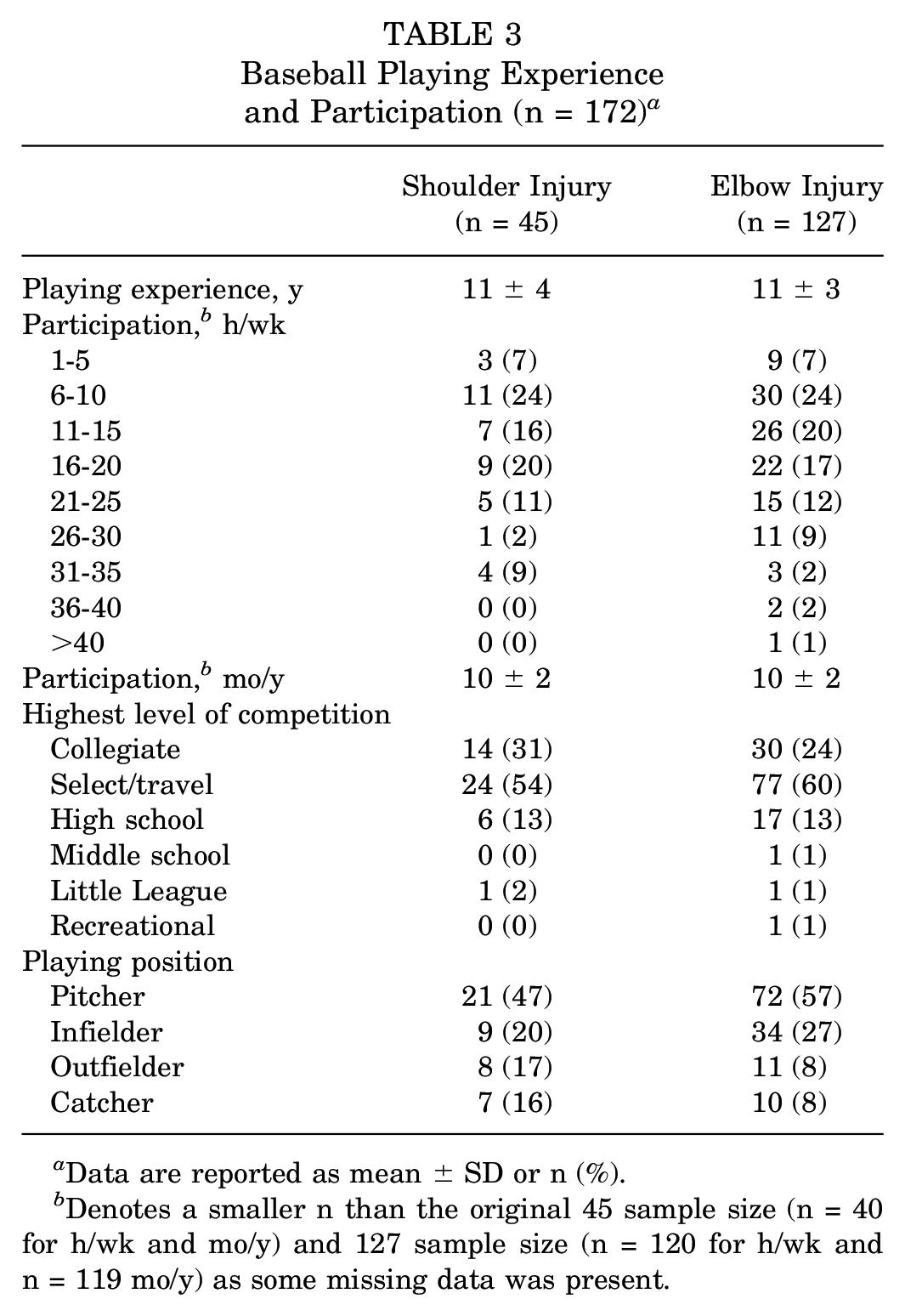
Data are reported as mean ± SD or n (%).
Denotes a smaller n than the original 45 sample size (n = 40 for h/wk and mo/y) and 127 sample size (n = 120 for h/wk and n = 119 mo/y) as some missing data was present.
Descriptive glenohumeral ROM data for both the elbow and shoulder injury groups are documented in Table 4. In the players with a shoulder injury, there was a disparity between objective differences in GER and the HRT-corrected GERD (t(44) = −12.99 [95% CI of the difference, −18.36° to −13.43°]; P < .001; d = −1.94); likewise, there was a disparity between objective differences in GIR and the HRT-corrected GIRD (t(44) = 12.99 [95% CI of the difference, 13.43° to 18.36°]; P < .001; d = 1.94) (Figure 3A). Similarly, in the players with an elbow injury, there was a disparity between objective differences in GER and the HRT-corrected GERD (t(126) = −20.05 [95% CI of the difference, −17.47° to −14.33°]; P < .001; d = −1.78) as well as a disparity between objective differences in GIR and the HRT-corrected GIRD (t(126) = 20.05 [95% CI of the difference, 14.33° to 17.47°]; P < .001; d = 1.78) (Figure 3B).
ROM Findings a

Data are reported as mean ± SD (in degrees). The injured arm always represents the throwing arm. GER, glenohumeral external rotation; GERD, glenohumeral external rotation deficit; GIR, glenohumeral internal rotation; GIRD, glenohumeral internal rotation deficit; HRT, humeral retrotorsion; ROM, range of motion; TROM, total range of motion.
A negative value indicates greater HRT in the injured (throwing) arm versus the noninjured arm.
A negative value indicates a deficit, while a positive value indicates greater motion in the injured arm.
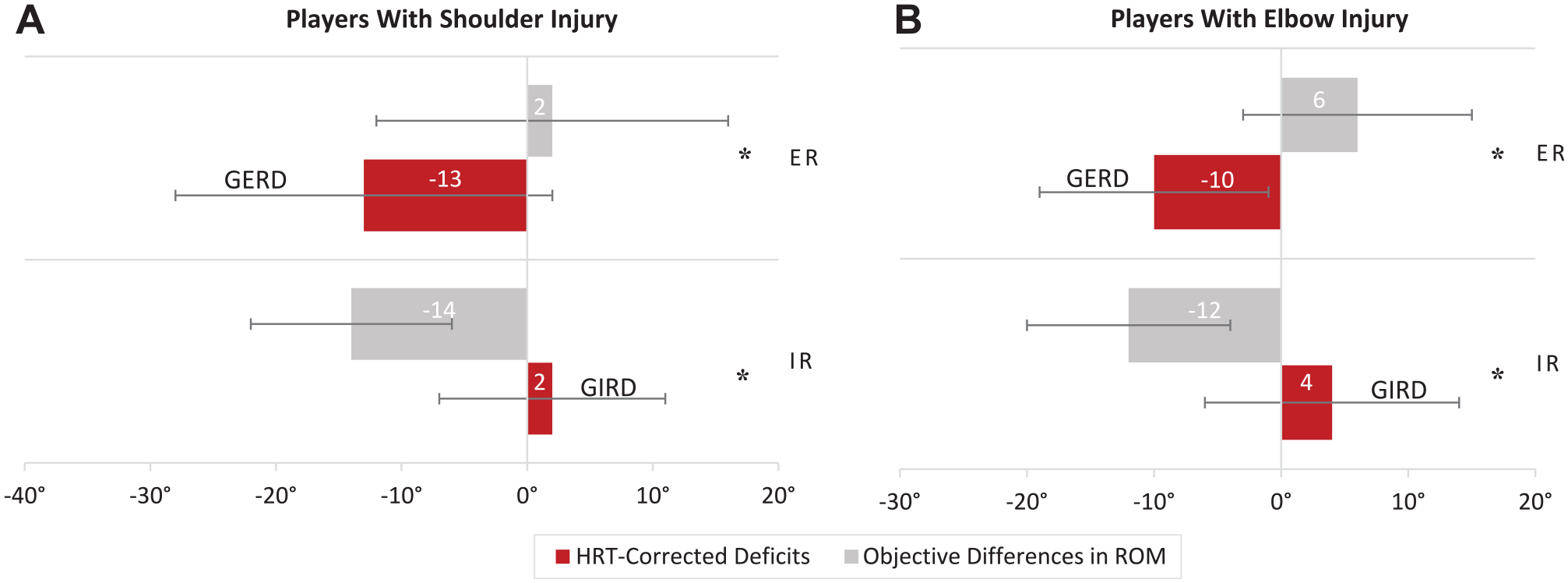
Objective glenohumeral range of motion (ROM) and humeral retrotorsion–corrected ROM in the (A) players with a shoulder injury (n = 45) and (B) players with an elbow injury (n = 127). *Statistically significant difference (P < .001). ER, external rotation; GERD, glenohumeral external rotation deficit; GIRD, glenohumeral internal rotation deficit; IR, internal rotation.
Discussion
The results of the present study indicated that baseball athletes with either shoulder or elbow injuries demonstrated significant disparities between objective side-to-side differences in glenohumeral ROM and HRT-corrected motion. These findings supported our hypothesis that there were disparities between objectively measured differences in GER and GIR motion compared to the HRT-corrected GERD and GIRD in a population of injured baseball players. More specifically, injured baseball players demonstrated a paradoxical shift in ROM profiles when comparing objectively measured differences in motion to HRT-corrected motion. Without the context of HRT, injured baseball athletes demonstrated greater objective GER motion and less objective GIR motion on the injured side compared to the noninjured side; however, when accounting for HRT, the rotational profiles shifted, and a deficit in GER (GERD) became present. These results suggest that osseous changes must be considered to determine the direction in which true motion loss at the shoulder is occurring in injured baseball athletes.
Our findings are similar with past research conducted in healthy populations of baseball players. Myers et al 22 investigated a group of 29 collegiate baseball players compared to age-matched controls and calculated retrotorsion-corrected internal rotation and external rotation to be 3° and −13°, respectively. Likewise, Reuther et al 25 investigated 30 professional baseball pitchers and reported 6° of internal rotation and −9° of external rotation when correcting for HRT. It should be noted that sample sizes were smaller in these studies compared with the current study, and different measurement techniques were implemented for GIR motion, 22 as stabilization occurred at the acromion process and no scapular stabilization occurred during GER motion. 25 The inclusion of scapular stabilization allows for the assessment of true glenohumeral motion and improves the reliability of the measurement. 39 Our findings, in conjunction with prior investigations, suggest that when correcting for HRT, a GIRD is oftentimes not present, and interventions aimed toward improving the GIRD may not be indicated. In contrast, a deficit in external rotation (GERD) is often present when correcting for retrotorsion, and interventions aimed toward restoring this deficit in motion should be implemented. This is an important finding, as previous research has demonstrated that professional baseball players presenting with a side-to-side difference in external rotation <5° were more likely to be on the injured list and have time loss to undergo a surgical intervention at the shoulder. 37 This finding is specific to professional baseball players and has yet to be investigated in a population of adolescent baseball players. Baseball athletes presenting with an HRT-corrected GERD may benefit from clinical interventions aimed at improving GER motion to reduce the risk of time loss from shoulder injuries. Because of the differences in methodologies for assessing shoulder ROM and calculating HRT-corrected ROM, clinicians are urged to use caution when interpreting results between studies of healthy and injured baseball athletes.
It is important to note the finding for side-to-side differences in TROM in the present study. A previous study demonstrated an increased risk for throwing-related injuries when the side-to-side difference is >5°. 38 On average, injured baseball players in both the shoulder and elbow injury groups demonstrated a >5° loss of TROM in the throwing limb, warranting a clinical intervention to restore lost ROM (dependent on HRT-corrected GERD and GIRD calculations). However, the wide standard deviation suggests that not all baseball players evaluated presented with a loss of TROM. In the absence of TROM loss, we urge clinicians to use sound clinical judgment when determining whether interventions aimed at increasing shoulder ROM are appropriate.
The cumulative results regarding the interpretation of objective rotational motion and HRT-corrected motion in both injured and uninjured baseball athletes suggest a shift in the paradigm to screen for and treat ROM loss in this athletic population.22,25,33 We encourage future investigators and practicing clinicians to consider the effects of HRT on glenohumeral ROM profiles when evaluating baseball athletes. We are confident that the methods for investigating HRT described in this study are reproducible for clinicians who have access to a diagnostic ultrasound device and undergo appropriate training to reliably measure HRT. Clinicians who do not have access to a diagnostic ultrasound device may benefit from utilizing a validated algorithm for predicting humeral torsion that was published by Bullock et al 3 in 2021. This equation allows clinicians with limited resources to calculate an athlete's HRT based on a number of clinical objective and demographic variables. This prediction model, in combination with the proposed calculations in this study for determining retrotorsion-corrected motion, can be used to assess how retrotorsion affects ROM in baseball athletes. These methods will allow clinicians to implement appropriate intervention strategies to ameliorate any observed HRT-corrected motion deficits. If internal rotation loss is observed after correcting for retrotorsion, known interventions targeting the posterior shoulder should be implemented. However, if external rotation loss is documented after correcting for torsion, interventions targeting the larger anterior muscles of the shoulder should be incorporated into the care plan.
To expand the clinical applicability of HRT and the results of this study, we provide a clinical example using a 17-year-old baseball player with a right shoulder injury. This player has a GER difference of 5°, a GIR difference of −15°, and a TROM difference of −10°. In this scenario, a decision would likely be made to improve GIR motion in the injured throwing arm to regain TROM symmetry. However, rotational motion needs to be interpreted within the context of HRT. Thus, relative HRT in this case is −15° (indicating more retrotorsion in the injured arm compared to the noninjured arm). Consequently, someone would expect the throwing arm to have 15° more external rotation and 15° less internal rotation. Within the context of HRT, there is an HRT-corrected GERD of −10° and an HRT-corrected GIRD of 0° present in this athlete. Therefore, the athlete is missing motion in the direction of GER, and interventions to improve GER should be implemented.
Limitations
This study is not without limitations. There was a wide range of shoulder and elbow injury diagnoses in this cohort of baseball athletes. Future researchers should aim to determine if these results are similar in a cohort of participants with similar diagnoses (eg, ulnar collateral ligament tear, superior labral anterior-to-posterior tear). The majority of baseball players in this study were White; however, previous research has indicated that, on average, Latin American–born players demonstrate greater HRT than their North American–born teammates. 31 Future studies comparing HRT-corrected motion between geographic regions would be of interest to determine if there are larger deficits present in corrected external rotation. Participants included in this study were nonprofessional baseball players, with approximately half identifying their main position as pitcher. As such, differences in these results between level of play and position should be investigated, as throwing frequency at a young age may contribute to a baseball player's relative HRT. 3 These data were analyzed retrospectively and interpreted at a single time point after a shoulder or elbow injury. We encourage future researchers to prospectively determine the odds of sustaining an injury utilizing the HRT-corrected GERD and GIRD to account for the osseous changes that occur with throwing. Lastly, it would be valuable for future researchers to consider the effect of therapy on the HRT-corrected GERD and GIRD.
Conclusion
Baseball players with a shoulder or elbow injury demonstrated significant disparities between objective differences in GIR and GER compared to the HRT-corrected GIRD and GERD. Consideration needs to be given to the osseous adaptations that occur at the glenohumeral joint due to the repetitive nature of throwing when evaluating and treating an overhead athlete. Objective ROM in a thrower should be interpreted within the context of relative HRT. In the absence of HRT measurements, the health care team can only make inferences on side-to-side differences in motion. To determine rotational deficits, relative HRT must be taken into account and will help guide the direction in which the injured player should be stretched. This information provides a baseline for the clinician to properly evaluate and treat potential losses of shoulder ROM in a baseball player with a shoulder or elbow injury.
Footnotes
Appendix
Injury Diagnoses During Initial Surgeon Visit (n = 172) a

| No. of Players | |
|---|---|
| Elbow | |
| MUCL sprain | 43 |
| MUCL tear | 20 |
| Little League elbow | 13 |
| Osteochondritis dissecans | 13 |
| Compression of ulnar nerve | 6 |
| Impingement of olecranon | 6 |
| Neurogenic TOS | 5 |
| Medial epicondyle avulsion fracture | 4 |
| Compression of median nerve | 3 |
| Pronator teres syndrome | 3 |
| Elbow pain | 2 |
| Fracture of olecranon | 2 |
| Osteochondral lesion | 2 |
| Brachial plexus neuropathy | 1 |
| Fracture of distal humerus | 1 |
| Muscle strain | 1 |
| Salter-Harris fracture, type 1 | 1 |
| Stress reaction of sublime tubercle | 1 |
| Shoulder | |
| Internal impingement | 8 |
| Little League shoulder | 6 |
| Subacromial impingement | 6 |
| Shoulder instability | 5 |
| Dynamic posterior instability | 4 |
| Shoulder pain | 4 |
| Labral tear, posterior | 3 |
| Salter-Harris fracture, type 1 | 3 |
| Neurogenic TOS | 2 |
| Labral tear, anterior | 1 |
| Nerve-related injury | 1 |
| Salter-Harris fracture, type 2 | 1 |
| SLAP tear | 1 |
MUCL, medial ulnar collateral ligament; SLAP, superior labral anterior-to-posterior; TOS, thoracic outlet syndrome.
Final revision submitted December 8, 2023; accepted January 10, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.E.C. has received education payments, nonconsulting fees, and royalty or licenses from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Texas Health Science Center at Houston (ref No. 247197).