
Abstract
Background:
Patellar fracture, femoral physis injury, and recurrent instability are concerning complications in medial patellofemoral ligament (MPFL) reconstruction (MPFLR) techniques for recurrent patellar dislocation in children and adolescents.
Purpose:
To evaluate the outcomes of an anatomic all–soft tissue fixation technique for reconstruction of the medial patellofemoral complex (MPFC) using a double-bundle quadriceps tendon (QT) autograft for recurrent patellar dislocation in skeletally immature patients.
Study Design:
Case series; Level of evidence, 4.
Methods:
This retrospective study involved 24 skeletally immature patients (24 knees; 16 women and 8 men; age range, 9.5-15 years) with recurrent patellar dislocation who underwent MPFC reconstruction using a double-bundle QT autograft between September 2018 and January 2021. Only soft tissue suture fixation was used on the femoral and patellar sides of the 2 bundles of the QT. Radiographs, computed tomography, and magnetic resonance imaging were used to evaluate physeal status, lower limb alignment, patellar height and tilt, trochlear morphology, tibial tubercle-trochlear groove distance, and any associated knee pathology. Functional outcomes were assessed with the Kujala score, the visual analog scale (VAS) for pain, and the grading system of Insall et al.22
Results:
The mean follow-up time was 40 ± 9.6 months (range, 28-56 months). At the final follow-up, the Kujala and VAS pain scores showed a significant improvement versus preoperative scores (P < .001), and the passive lateral patellar glide showed a significant reduction (P < .001). All patients had negative apprehension and J signs. Of the 24 patients, 23 regained full range of motion, while 1 patient had a knee flexion deficit. The patellar tilt angle improved significantly at the final follow-up (P < .001). There was no patellar fracture, femoral physis injury, or recurrence of patellar dislocation. According to the grading system of Insall et al, the results were excellent in 15 knees (62.5%), good in 8 knees (33.3%), fair in 1 knee (4.2%), and no knees showed poor results.
Conclusion:
Reconstruction of the MPFC using a double-bundle QT autograft with an all–soft tissue fixation technique was an effective method for treating patellar instability in skeletally immature patients.
Keywords
Patellar dislocation is a relatively common and challenging acute knee injury, especially in skeletally immature patients.2,11,21,34,35,39 It has been found that skeletally immature patients have >2 times the risk of recurrent instability compared with skeletally mature patients. 30 Many factors contribute to instability, such as trochlear dysplasia, patella alta, valgus alignment, increased tibial tubercle-trochlear groove (TT-TG) distance, and increased patellar tilt. 9 Nonoperative treatment is the mainstay for primary dislocation; however, up to 30% to 50% of patients experience recurrent dislocation for which surgical intervention is required.21,33,52
The medial patellofemoral ligament (MPFL) is the primary static stabilizer for lateral patellar dislocation from full knee extension to 30° of knee flexion. It shares approximately 50% of the restraint for lateral patellar dislocation.3,6,8,10,36,58 The MPFL is injured in about 95% to 100% of patients after the first patellar dislocation; thus, MPFL reconstruction (MPFLR) is one of the main pillars in the surgical management of patellar instability, especially in skeletally immature patients.7,19,42,49 Recent studies have evolved with a description of a component of the MPFL, which is termed the medial quadriceps tendon femoral ligament (MQTFL),15,16,26 that has the same femoral origin as the MPFL; however, it inserts on the quadriceps tendon (QT) rather than the patella. A new term for the medial patellar soft tissue restraints has emerged, the medial patellofemoral complex (MPFC),24,55,56 which is the combination of both the MPFL and the MQTFL. Several MPFC reconstruction (MPFCR) techniques have recently evolved using different types of grafts and fixation implants.15,33,56,59
Many MPFLR techniques use either patellar bony tunnels or sockets that place the proportionately smaller patella in children and adolescents at higher risk of fracture1,28,44,48 and/or femoral tunnels that place the femoral physis at risk of injury. 50 Although the soft tissue pulley technique does not place open growth plates at risk, it does not allow for anatomic MPFLR and has inferior clinical results.31,40
Given this background, we aimed in the present study to evaluate the functional outcome of the anatomic all–soft tissue fixation technique for MPFCR using a double-bundle QT autograft for recurrent patellar dislocation in skeletally immature patients (Figure 1). We hypothesized that an implant- and drill-free reconstruction of the MPFC using a partial-thickness QT with an all–soft tissue patellar and femoral fixation could restore patellar stability and could avoid patellar fracture or femoral physis injury. This technique would allow for accurate anatomic femoral fixation using intraoperative anatomic landmarks. It would also restore the normal anatomy of the proximal medial patellar soft tissue restraint.

A postoperative schematic diagram of the knee joint showing all–soft tissue fixation technique for medial patellofemoral complex reconstruction. (A) A diagram in the absence of the VMO, with the MPFL and MQTFL grafts placed so that they mirrored each other medially. (B) A diagram in the presence of the VMO showing the 2 grafts being passed deep to the VMO; the yellow arrow points to the site where the 2 grafts were sutured to the anatomic femoral attachment. AMT, adductor magnus tendon; LCL, lateral collateral ligament; MPFL, medial patellofemoral ligament; MQTFL, medial quadriceps tendon femoral ligament; PT, patellar tendon; QT, quadriceps tendon; SMCL, superficial medial collateral ligament; VMO, vastus medialis obliquus.
Methods
Our institutional ethics committee approved the protocol for this retrospective study. A total of 71 skeletally immature patients with a history of recurrent patellar dislocation who underwent primary MPFLR at our arthroscopy and sports injury unit between September 2018 and January 2021 were identified. Immature patients were defined as those with radiological proof of open physes; age was not a primary inclusion criterion. A history of at least 2 dislocations of the patella, unimproved despite a nonoperative treatment program, and a minimum 2 years of follow-up were mandatory for inclusion. We also required preoperative and final follow-up full-length standing and true-lateral radiographs. Patella alta (Insall-Salvati ratio >1.2; Caton-Deschamps index >1.2) and increased TT-TG distance (>20 mm) were not considered contraindications for inclusion. We excluded 47 patients according to the following criteria: use of grafts other than the QT autograft for reconstruction (n = 21), single-bundle MPFLR with a QT autograft (n = 15), and incomplete follow-up (n = 2; however, none of these cases had experienced recurrent instability at the most recent follow-up), incomplete records and radiographs (n = 3), ipsilateral cruciate ligament injury (n = 1), Down syndrome (n = 1), and patients who underwent bony procedures for correction of coronal plane deformities (n = 4).
Ultimately, 24 knees in 24 patients were eligible for inclusion (16 women and 8 men), with a mean age of 12.4 ± 1.6 years (range, 9.5-15 years). Included were 14 right and 10 left knees. Figure 2 shows the flowchart of patient eligibility and inclusion.
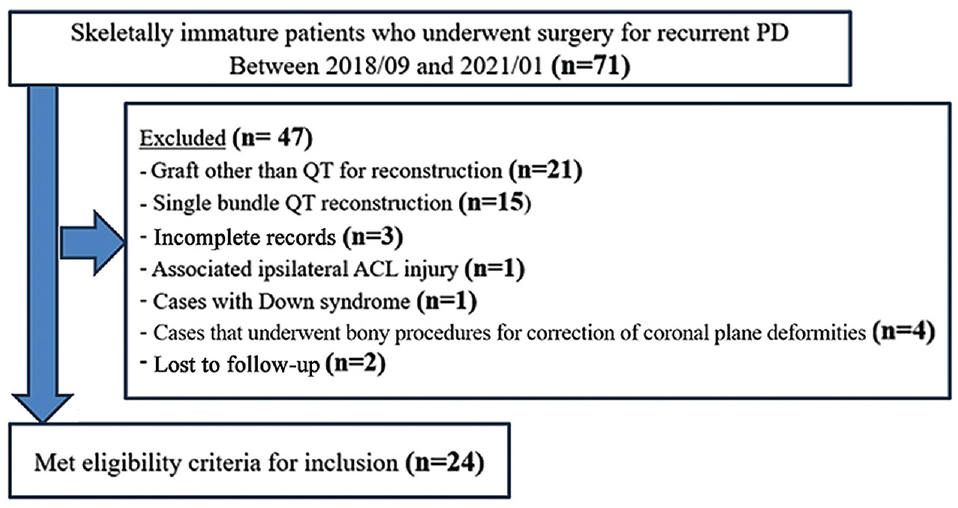
Flowchart of patient inclusion and exclusion in the study. PD, patellar dislocation; QT, quadriceps tendon.
Surgical Technique
All surgeries were performed by a single senior surgeon (A.M.N.Z.). For this study, we adopted the treatment technique described by Zein and Hassan. 59 In brief, an arthroscopic knee examination was performed and included management of any intra-articular meniscal or chondral pathology as well as evaluation of patellar tracking. A partial-thickness QT autograft was harvested through a midline skin incision, measuring 7 to 8 cm long, 10 to 15 mm wide, and 2 to 3 mm thick. The QT graft was released proximally and left attached distally, a few millimeters above the upper pole of the patella (Figure 3).
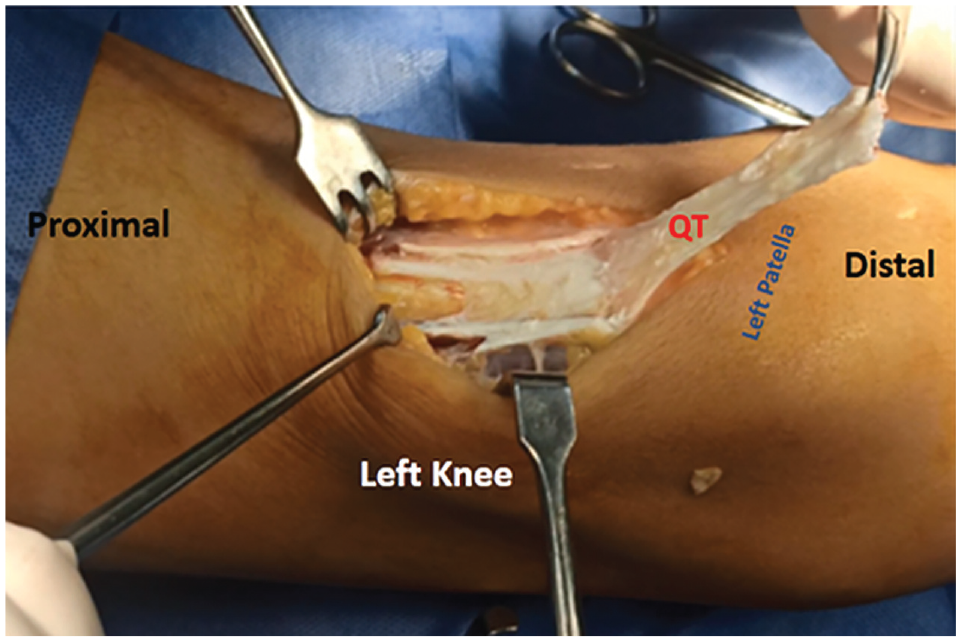
An intraoperative photograph of a left knee showing a partial-thickness QT graft being harvested. The graft was left intact, just a few millimeters above the proximal pole of the patella. QT, quadriceps tendon.
The QT graft was then divided into 2 bundles: a medial and a lateral bundle. The medial bundle (planned for MQTFL reconstruction and referred to hereafter as the “MQTFL graft”) was left attached to the QT just proximal to the upper border of the patella. It was never released further distally, and it was firmly secured to the QT just above the upper border of the patella with a nonabsorbable stitch. The lateral bundle (planned for MPFLR and referred to hereafter as the “MPFL graft”) was dissected more distally from the proximal pole of the patella, moving its distal attachment site to just above the middle of the anterior surface of the patella. It was secured to the soft tissue on the anterior surface of the patella by a nonabsorbable stitch (Figure 4).
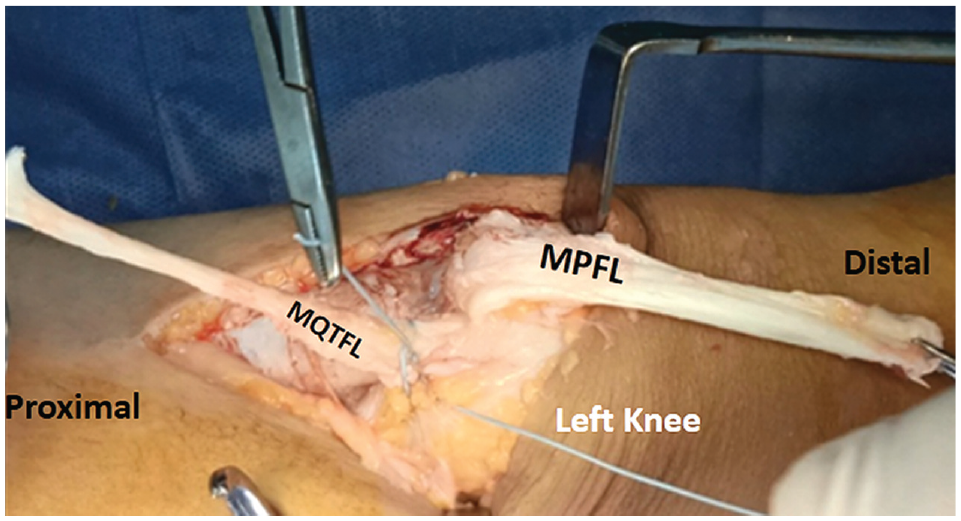
An intraoperative photo of a left knee. The QT graft was divided into 2 bundles: a medial bundle for MQTFL reconstruction and a lateral bundle for MPFLR. The MQTFL graft was left attached to the QT just proximal to the upper border of the patella, and it was never released further distally. The MQTFL graft was securely fixed to the QT with a nonabsorbable stitch. The MPFL graft was dissected more distal over the patella, and its lateral border was dissected more distal than its medial side to facilitate its placement on the medial side of the knee. The attachment of the MPFL graft was moved from the upper pole of the patella to just above the midline of the patella, and it was securely fixed to the soft tissue on the anterior surface of the patella with a nonabsorbable stitch. MQTFL, medial quadriceps tendon femoral ligament; MPFLR, medial patellofemoral ligament reconstruction; MQTFL, medial quadriceps tendon femoral ligament; QT, quadriceps tendon.
Both bundles were placed side by side on the medial side of the knee, with the MQTFL graft lying proximal to the MPFL graft, to evaluate the adequacy of their length (Figure 5). The lengths of the 2 grafts were considered sufficient if they extended beyond the adductor magnus tendon (AMT).

(A) An intraoperative photo of a right knee. The MQTFL and MPFL grafts were placed on the medial side of the knee to evaluate their lengths. The MQTFL graft was attached to the QT just proximal to the upper pole of the patella, while the MPFL graft was attached to the proximal part of the patella. (B) Schematic presentation of a right knee showing the normal anatomic arrangement of the 2 bundles of the medial patellofemoral complex (MQTFL and MPFL). AT, adductor tubercle; MPFL, medial patellofemoral ligament; MQTFL, medial quadriceps tendon femoral ligament; QT, quadriceps tendon; SMCL, superficial medial collateral ligament; VMO, vastus medialis obliquus.
Through a 2- to 3-cm skin incision centered on the adductor tubercle (AT), the AMT was identified near its insertion in the AT, and it was used as an intraoperative anatomic landmark for the accurate localization of the femoral attachment of the MPFL, which lies just distal and anterior to the AT5,29 (Figure 6).

(A) An intraoperative photograph of a left knee identifying the AMT at its femoral insertion. The blue dot represents the anatomic femoral attachment of the MPFL, which is distal and anterior to the adductor tubercle. (B) A photograph of a right femur on a Sawbones model shows the anatomic bony landmarks and the femoral attachment of the MPFL on the medial side of the medial femoral condyle. The blue dot represents the MPFL and the back dots represent the AT, GT, and ME. AMT, adductor magnus tendon; AT, adductor tubercle; GT, gastrocnemius tubercle; ME, medial epicondyle; MPFL, medial patellofemoral ligament.
Then, the 2 grafts were passed medially deep to the vastus medialis obliquus muscle (VMO) with care to remain extra-articular. The MPFL graft was placed overlaying the anatomic femoral attachment point, which is distal and anterior to the AT. The MQTFL graft was first passed deep to the AMT, which acts as a pulley. Then, it was turned toward the MPFL graft to overlay the anatomic femoral attachment point as well. A nonabsorbable suture was used to secure the 2 grafts to the soft tissue and periosteum at this anatomic point with the knee at 40° to 60° of flexion (Figure 7).

(A) An intraoperative photo of a left knee showing the AMT at its femoral insertion. The MPFL graft was placed overlaying the anatomic femoral attachment point, which is distal and anterior to the AMT insertion. The MQTFL graft was first passed deep to the AMT, which acts as a pulley. (B) An intraoperative photo of a left knee showing the MQTFL graft turned toward the MPFL graft to overlay the anatomic femoral attachment point. A nonabsorbable suture was used to secure the 2 grafts to the soft tissue and periosteum at this anatomic point with the knee at 40° to 60° of flexion. The blue dot represents the site of securing both grafts to the anatomic femoral attachment.
Postoperative Rehabilitation
Postoperatively, the patients were immobilized for 2 weeks using hinged knee braces locked in extension. Isometric quadriceps muscle exercises, active ankle exercises, and partial weightbearing were initiated immediately. Full range of motion and full weightbearing exercises were encouraged under the protection of the brace at 3 weeks. The brace was removed at 6 weeks postoperatively.
Data Collection
Preoperative data—including age, sex, laterality, medical and surgical history, family history, and history of dislocations—were retrieved from the patients’ medical records. Pre- and postoperative knee assessments were undertaken by 3 senior surgeons (A.M.N.Z., A.F.A.A., and A.Z.M.H.), who have >18 years of experience in the fields of orthopaedic surgery and sports medicine. These included an assessment of the patients’ symptoms and clinical evaluation of gait, limb alignment, presence of the J-sign, patellar apprehension, and range of motion. Generalized ligamentous laxity was evaluated preoperatively using the Beighton score, 4 and documentation in the clinical chart was available if the patient had ligamentous laxity (defined as a Beighton score of ≥4), but specific Beighton scores were not noted; thus, only the presence of ligamentous laxity was documented. Patellar tilt was evaluated clinically by the passive patellar tilt test. 17 The lateral patellar glide test was employed to assess lateral patellar displacement before and after MPFCR, in which the patella was divided into 4 vertical quadrants. A normal lateral patellar glide should not exceed 2 quadrants of lateral patellar translation. 25
All included patients underwent pre- and postoperative radiographic examinations, magnetic resonance imaging, and 3-dimensional computed tomography (CT). Different radiographic evaluation parameters were used in this study. A full-length standing radiograph for each patient was essential to assess lower limb alignment. A standard protocol for taking full-length films was ensured for every included patient, including taking the whole lower limbs from hips to ankles on a single film. Both lower extremities were oriented with each patella facing forward, regardless of the foot position (patella centered on the femoral condyles), and with each knee maximally extended. A magnification marker was positioned in the film; the central x-ray beam was aimed between the knees and was perpendicular to the x-ray cassette.
The mechanical axis of the lower limb was evaluated, and the mechanical axis deviation (MAD), which is the perpendicular distance from the mechanical axis line of the lower limb in the frontal plane to the center of the knee joint line, was measured (Figure 8). The distal femoral physis integrity was evaluated by comparing the preoperative and final follow-up values of the mechanical lateral distal femoral angle (mLDFA) and the posterior distal femoral angle (PDFA) to assess coronal and sagittal plane deformities, respectively. True-lateral radiographs were used to measure the PDFA, trochlear dysplasia using the Dejour classification, and the patellar height using the Caton-Deschamps index and the Insall-Salvati ratio. For a perfect lateral view, it was essential to have a perfect superimposition of the 2 posterior condyles with the knee at 30° of flexion (Figure 9). Two authors (A.F.A.A. and A.Z.M.H) calculated the radiographic parameters, and interrater reliability was measured. The means of the measurements between the 2 reviewers were used in the statistical comparison of the pre- and postoperative parameters.

Full-length standing radiographs were used to assess limb alignment: (A) the mechanical axis of the lower limb and the MAD and (B) the mLDFA. AP, anteroposterior; LDTA, lateral distal tibial angle; LPFA, lateral proximal femoral angle; LT, left; MAD, mechanical axis deviation distance; MED, medial; mLDFA, mechanical lateral distal femoral angle; MPTA, medial proximal tibial angle; RT, right.
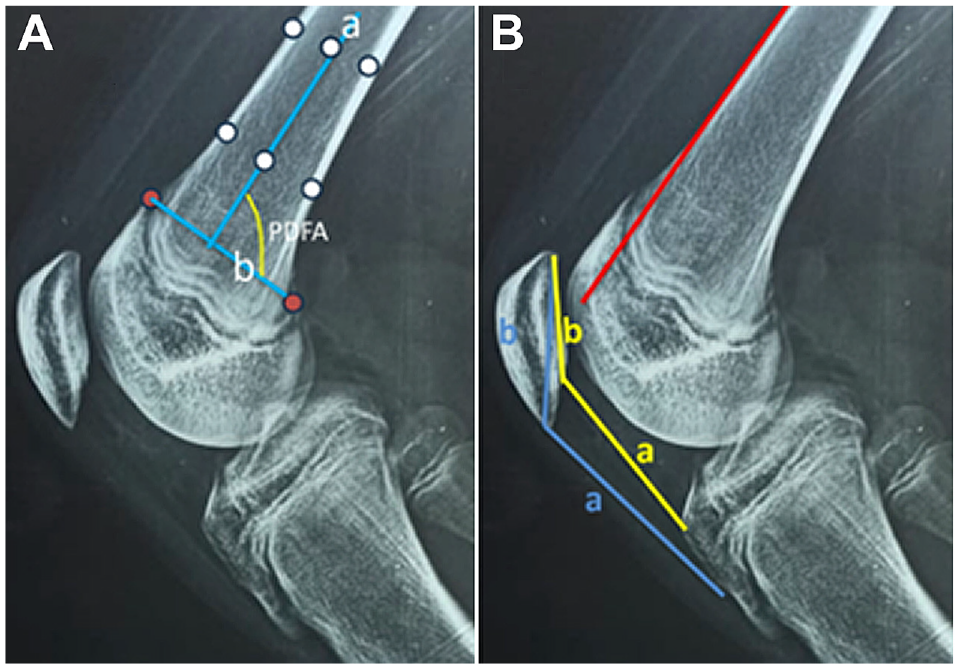
Measurements on lateral radiographs of the knee joint. (A) The PDFA was measured preoperatively and at the final follow-up to assess any deformity in the sagittal plane. The joint orientation line of the distal femur (blue line b) is the line that connects the anterior and posterior exit points of the distal femoral physis (red circles). The anatomic axis of the distal femur (blue line a) connects the 2 central diaphyseal points (middle white circles; one proximal and the other distal). Each of the central points represents the center of a line that connects an anterior and a posterior cortical point (the 4 cortical white circles). The PDFA is the posterior angle created by the intersection of line b and line a. (B) The patellar height was calculated using the Caton-Deschamps index and the Insall-Salvati ratio. The Caton-Deschamps index was measured as the ratio of the distance between the inferior articular surface of the patella and the anterosuperior angle of the tibia (yellow line a) to the length of the articular surface of the patella (yellow line b). A ratio of ≤0.6 indicated patella baja and a ratio of ≥1.2 indicated patella alta. The Insall-Salvati ratio was measured as the ratio between the length of the patellar tendon (blue line a) and the longest sagittal diameter of the patella (blue line b). A ratio of <0.8 indicated patella baja, and a ratio >1.2 indicated patella alta. The Dejour classification system was used to measure trochlear dysplasia; Dejour type B is demonstrated in the above radiograph, with a supratrochlear spur (femoral condyle extends beyond the anterior femoral cortex, red line) and a crossing sign (trochlear groove line passes lateral condylar line). PDFA, posterior distal femoral angle.
The patellar tilt angle (PTA), which is the angle between a line defining the maximal patellar width and the femoral posterior condylar line, was measured on axial CT scans (Figure 10). The TT-TG distance was also measured on axial CT scans.

(A) Preoperative axial CT scans of a left knee in a patient showing lateral patellar subluxation and a PTA of 24.6°. (B) CT scans of the same patient at the final follow-up showing an improved PTA of 4.5° and a centralized patella. The top row shows an axial cut of the patellofemoral joint where the patella has the maximal width; the bottom row shows an axial cut of the distal femur where the intercondylar notch appears like a Roman arch (reference cut where the line tangent to the posterior femoral condyles was taken). CT, computed tomography; PTA, patellar tilt angle.
The functional outcomes were assessed preoperatively and at the final follow-up using the Kujala score, 27 pain on a 10-point visual analog scale (VAS) (0 indicating no pain and 10 indicating maximum pain), and the grading system of Insall et al, 22 in which outcomes were categorized as excellent (no pain or instability, normal function including return to sports), good (mild pain, no instability, and normal function), fair (moderate pain, occasional instability, mildly limited function), or poor (moderate to severe pain and instability including redislocation).
Statistical Analysis
Data analysis was performed using SPSS statistical software Version 25 (IBM). The normality of the data was tested using the Shapiro-Wilk test. Data were expressed as mean ± SD and range for parametric quantitative data and median and interquartile range for nonparametric quantitative data, in addition to both number and range for qualitative data. Preoperative and final postoperative values were compared for nonparametric quantitative data using the Wilcoxon signed-rank test. The interrater reliability of the radiological measurements between the 2 reviewers was calculated using the intraclass correlation coefficient (ICC). For all statistical comparisons, P < .05 was considered statistically significant.
Results
The characteristics of the patients are summarized in Table 1, and the clinical and functional outcomes for each patient are shown in Appendix Table A1. The mean postoperative follow-up was 40 ± 9.6 months (range, 28-56 months). None of the included patients had undergone previous knee surgery, and none were identified as having generalized ligamentous laxity preoperatively on Beighton score screening.
Characteristics of the Study Patients (N = 24) a

F, female; L, left; M, male; PTA, patellar tilt angle; R, right.
Concomitant procedures were performed in 9 patients (37.5%). Three patients had tight lateral structures with a positive patellar tilt test and a patellar tilt angle of >20°. One patient underwent arthroscopic lateral release, and 2 patients underwent lateral retinacular lengthening. Two patients underwent patellar chondroplasty, and 2 patients underwent repair for medial meniscus tears (Tables 1 and 2).
Type and Distribution of Concomitant Procedures

Preoperative physical examinations showed a positive apprehension sign in almost all patients and a positive J-sign in 8 patients—Dejour type B in 6 patients and type D in 2 patients. At the final follow-up, all patients had negative apprehension and J-sign. All of the knees had excessive lateral patellar glide preoperatively; however, at the end of the follow-up, all patients had a normal passive lateral patellar glide, showing a significant improvement (P < .001) (Table 3). At the final follow-up, 23 knees regained full range of motion equal to the contralateral knee, but 1 knee had incomplete knee flexion. A total of 23 patients regained full quadriceps muscle power and size, while 1 patient had quadriceps muscle wasting (10 mm compared with the noninjured side).
Comparison of Lateral Patellar Glide and Functional Outcome Scores From the Preoperative to the Final Follow-up a

Bold P values indicate statistically significant differences between the preoperative and final follow-up scores (P < .05). IQR, interquartile range; PLG, passive lateral patellar glide; Preop, preoperative; VAS, visual analog scale.
Functional outcomes of the Kujala and VAS pain scores showed significant improvements at the final follow-up (P < .001) (Table 3). According to the grading system of Insall et al, 22 the results at the final follow-up were excellent in 15 knees (62.5%), good in 8 knees (33.3%), fair in 1 knee (4.2%), and no knees showed poor results.
The overall ICC for the interrater reliability of the radiographic measurements was >0.90, indicating excellent agreement. The mean patellar height was 1.1 ± 0.2 (range, 0.8-1.4) by the Insall-Salvati ratio and 1.1 ± 0.1 (range, 0.9-1.5) by the Caton-Deschamps index. The mean TT-TG was 14.7 ± 4.3 mm (range, 6-24 mm). According to the Dejour classification of trochlear dysplasia, the trochlea was normal in 3 (12.5%) patients, type A in 9 (37.5%) patients, type B in 6 (25%), type C in 4 (16.7%), and type D in 2 (8.3%) patients. The mean MQTFL length was 70.7 ± 6 mm (range, 64-84 mm), and the MPFL length was 80.6 ± 5.8 mm (range, 74-93 mm).
Regarding the main radiographic outcomes, there were no significant changes in the MAD, mLDFA, and PDFA between the preoperative and final follow-up values. The PTA showed a significant improvement (P < .001). The preoperative and final follow-up data for these parameters are summarized in Table 4.
Comparison of Main Radiographic Parameters From the Preoperative to the Final Follow-up a

The bold P value indicates a statistically significant difference between the preoperative and final follow-up scores (P < .05). IQR, interquartile range; MAD, mechanical axis deviation; mLDFA, mechanical lateral distal femoral angle; PDFA, posterior distal femoral angle; Preop, preoperative; PTA, patellar tilt angle.
Complications
Few complications were observed in the present series. Intraoperatively, there was 1 patient with a short MQTFL; in this patient, we did not loop the MQTFL around the AMT to save length, and we simply sutured the 2 grafts directly, just distal and anterior to the AMT insertion. This patient had a good outcome. One patient had chronic knee effusion due to postoperative trauma that resulted in the limitation of knee flexion (flexion deficit of 15°). This patient needed to return to the operating room for an arthroscopic synovectomy and manipulation under anesthesia. Two patients had mild discomfort at the suture site on the patella that did not require any interference. A partial avulsion of the MPFL from the anterior surface of the patella occurred due to the forceful pull of the bundle into the medial side of the knee. The bundle was securely sutured to the soft tissue on the patella, and care was taken not to repeat this mistake in subsequent cases. Three patients had a painless hypertrophic wound scar that did not require any interference. No patellar fracture, coronal physeal injury, or recurrence of patellar dislocation were seen in this series.
Discussion
The results of this study showed the effectiveness and safety of the proposed technique, with a significant improvement in the Kujala and VAS pain scores from preoperatively to the final follow-up (P < .001 for both). Patellar stability was restored in all patients. No patellar fracture, physeal injury, or recurrence of patellar dislocation were seen in this series. Also, 23 of 24 patients had satisfactory results. One patient had fair results due to trauma 6 months postoperatively, which resulted in chronic knee effusion and moderate pain with incomplete knee flexion. Arthroscopic synovectomy and manipulation under anesthesia were performed for this patient.
In their anatomic study, Kang et al 24 found that the MPFL is composed of 2 functional bundles from its patellar insertion: an inferior-straight bundle and a superior-oblique bundle with an angle of 15.1°± 2.1° in between; however, the 2 bundles had 1 femoral origin. They reported that the inferior-straight bundle was the main static soft tissue restraint, while the superior-oblique bundle associated with the VMO served as the main dynamic soft tissue restraint. The construct of the 2 bundles in our proposed technique is close to the anatomic description of the MPFL, as in the study by Kang et al. 24
Wang et al 57 and Kang et al23,24 found that both single- and double-bundle MPFLR can restore the stability of the patella. However, they reported that double-bundle reconstruction has an angular synergy effect that simulates the MPFL's wide footprint in the patella. This enables the patella to have a greater capacity to resist dislocation before it enters the femoral trochlea at a smaller flexion angle. Wang et al 57 reported a rate of recurrent instability with double-bundle grafts of 4.54% compared with 26.9% with single-bundle grafts and also noted that the Kujala scores were better with double-bundle grafts compared with single-bundle grafts (92.86 vs 80.46).
To our knowledge, nearly all double-bundle reconstruction techniques had 2 fixation points on the patella. Our study is one of the very few that was conducted for graft placement on both the patella and QT to anatomically reconstruct the proximal medial patellar restraints. In the present study, all patients regained patella stability with no recurrence of dislocation.
Patellar fracture is a great concern when performing MPFLR, especially in skeletally immature patients who have a relatively smaller patella. Patellar fractures have been reported as a devastating complication in many studies as a result of the formation of patellar tunnels or sockets.44,48 Furthermore, making a tunnel or tunnels in a small patella is a technical challenge and could potentially violate the patellar articular cartilage.39,40,48,51 In their study, Parikh et al 44 reported 6 (3.4%) patellar fractures in which patellar fixation was achieved through patellar tunnels. In the present study, we did not report any cases of patella fracture. Our described technique is a hardware- and drill-free technique, as we use the superficial strip of the QT, leaving its distal attachment intact. Consequently, the common complications encountered with patellar drilling and fixation were avoided.
A biomechanical study by Herbort et al 20 showed that the superficial strip of the QT was thin, broad, and sheet-like; therefore, they used a partial-thickness QT graft for MPFCR with satisfactory results. Taking only the superficial strip of the QT helps preserve quadriceps muscle function and improves postoperative rehabilitation and recovery.12,14,20,39,40 In the present study, 23 patients of 24 regained full quadriceps muscle power and size, while 1 patient had quadriceps muscle wasting (10 mm compared with the sound side). This patient sustained postoperative trauma with chronic knee effusion, for which arthroscopic synovectomy and manipulation under anesthesia were performed.
In their anatomic study, LaPrade et al, 29 reported that the mean length of the MPFL was 65.2 mm. In the present study, the mean MQTFL length was 70.7 ± 6 mm (range, 64-84 mm), and the MPFL length was 80.6 ± 5.8 mm (range, 74-93 mm), which was sufficient for reconstruction. The length of the graft can be assessed intraoperatively. If it is short, the QT (being broad) can be lengthened intraoperatively, even to double its length, by splitting it longitudinally and turning one-half 180°. There is no need for any preoperative measurements regarding the graft length, provided that, when harvesting the QT graft, it should be released as proximal as possible to gain the maximum possible length of the tendon.
In skeletally immature patients, the femoral origin of the MPFL is variable in its relation to the growth plate and is in close proximity to the growing femoral growth plate.13,18,41,45,46,47,53 Consequently, there is a challenge in localizing the MPFL femoral origin during reconstruction, with the high risk of injuring the growing growth plate if a femoral tunnel is made. Seitlinger et al 50 reported a case of femoral physis injury during MPFLR in a skeletally immature patient. Our described technique is a hardware- and drill-free technique, as we rely on soft tissue fixation at the femoral side. The grafts were simply sutured to the soft tissue and periosteum, with great care not to perform any aggressive soft tissue dissection to avoid iatrogenic growth plate injury. Consequently, we did not report any physeal injuries in the present study. Comparison between our preoperative and final postoperative radiographic measurements of the MAD, mLDFA, and PDFA showed a nonsignificant change. This denotes a nonsignificant change in the limb alignment both in the coronal and sagittal planes.
Most of the anatomic studies described the MPFL femoral origin as being in the “saddle” between the AT and medial epicondyle, or within 1 cm distal to the AT.29,43 In the present study, the femoral attachment point of both grafts was distal and anterior to the AT. We used the AMT insertion as an intraoperative landmark to precisely locate the femoral attachment of the native MPFL even without fluoroscopy. We found it a reproducible method that helps to overcome the problem of person-to-person variability in the femoral attachment point of the MPFL and also avoids the errors of localization when relying on radiography only. In their cadaveric study, Ziegler et al 61 emphasized the importance and accuracy of anatomy rather than radiography for precise localization of the anatomic femoral origin of the MPFL.
The femoral fixation method of the MPFL in skeletal immature patients, whether dynamic 38 or static,15,40 is a matter of great debate, as each method has its own advantages and disadvantages. In the present study, the 2 bundles were passed deep to the VMO. The MPFL graft was placed overlaying the anatomic femoral attachment point, which is distal and anterior to the AT. The MQTFL graft was first passed deep to the AMT, which acts as a pulley. Then, it was turned toward the MPFL graft to overlay the anatomic femoral attachment point. A nonabsorbable suture was used to secure the 2 grafts to the soft tissue and periosteum at this anatomic point with the knee at 40° to 60° of flexion. In this way, we think that we had a static soft tissue femoral fixation, which would be more forgiving than the static osseous fixation and, at the same time, more anatomic than the dynamic sling fixation.
A biomechanical study by Mountney et al 37 showed that suture fixation for MPFL repair or reconstruction is weaker than bony fixation. However, the biomechanical difference does not indicate a clinical difference. In a systematic review, Shah et al 51 found more complications in reconstruction using bone tunnels, but suture fixation in their study had a higher reported rate of recurrent instability. Sillanpää et al 54 reported excellent clinical results with suture fixation. Lind et al 32 conducted a randomized controlled study and reported that there is no difference in outcomes between femoral soft tissue and screw graft fixation for the reconstruction of the MPFL. They also concluded that soft tissue femoral graft fixation does not result in inferior clinical outcomes compared with screw fixation, and it can be used safely for MPFLR. In the present study, suture fixation was sufficient to fix the grafts on the femoral and patellar sides with no recurrence of dislocation.
Patellar tilt is a reflection of the soft tissue imbalance associated with lateral patellar dislocation. The patellar tilt angle was taken as an important radiological parameter for the restoration of soft tissue balance by the proposed technique. The results of this study showed a significant decrease in the patellar tilt angle. This indicates that the tension developed in the reconstructed MPFC positively influenced the tilt moment as well as patellar tracking. In the studies of Monllau et al 36 and Zhang et al, 60 the patellar tilt angle was taken as the main radiographic parameter to assess their results of MPFLR, and they reported significant improvements in the PTA at the final follow-up. However, the decreased patellar tilt angle could be a result of medial overconstraint rather than a balanced soft tissue. In the present study, all the patients had a normal passive lateral patellar glide, denoting no medial overconstraint.
Limitations
The present study has some limitations. It was retrospective and noncomparative, and due to the short follow-up duration, patellofemoral osteoarthritis could not be evaluated. Therefore, further studies with a larger sample size and a longer follow-up duration are needed.
Conclusion
Reconstruction of the MPFC using a double-bundle QT autograft with an all–soft tissue fixation technique is an effective method for the treatment of patellar instability in skeletally immature patients. It has the advantage of being an anatomic, reproducible, simple, safe, and cost-effective procedure.
Footnotes
Appendix
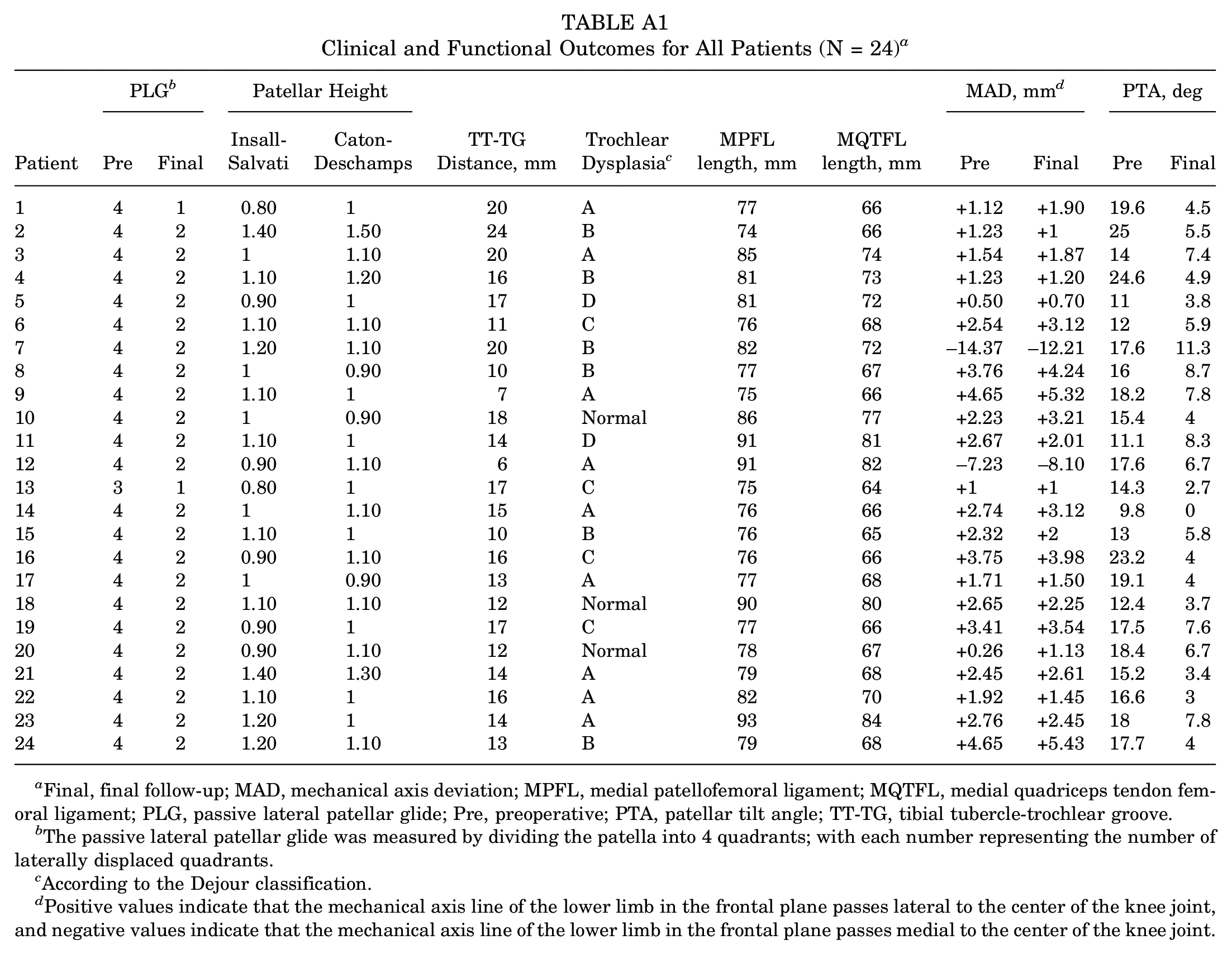
Clinical and Functional Outcomes for All Patients (N = 24) a
| Patient | PLG b | Patellar Height | TT-TG Distance, mm | Trochlear Dysplasia c | MPFL length, mm | MQTFL length, mm | MAD, mm d | PTA, deg | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Final | Insall- Salvati | Caton- Deschamps | Pre | Final | Pre | Final | |||||
| 1 | 4 | 1 | 0.80 | 1 | 20 | A | 77 | 66 | +1.12 | +1.90 | 19.6 | 4.5 |
| 2 | 4 | 2 | 1.40 | 1.50 | 24 | B | 74 | 66 | +1.23 | +1 | 25 | 5.5 |
| 3 | 4 | 2 | 1 | 1.10 | 20 | A | 85 | 74 | +1.54 | +1.87 | 14 | 7.4 |
| 4 | 4 | 2 | 1.10 | 1.20 | 16 | B | 81 | 73 | +1.23 | +1.20 | 24.6 | 4.9 |
| 5 | 4 | 2 | 0.90 | 1 | 17 | D | 81 | 72 | +0.50 | +0.70 | 11 | 3.8 |
| 6 | 4 | 2 | 1.10 | 1.10 | 11 | C | 76 | 68 | +2.54 | +3.12 | 12 | 5.9 |
| 7 | 4 | 2 | 1.20 | 1.10 | 20 | B | 82 | 72 | −14.37 | −12.21 | 17.6 | 11.3 |
| 8 | 4 | 2 | 1 | 0.90 | 10 | B | 77 | 67 | +3.76 | +4.24 | 16 | 8.7 |
| 9 | 4 | 2 | 1.10 | 1 | 7 | A | 75 | 66 | +4.65 | +5.32 | 18.2 | 7.8 |
| 10 | 4 | 2 | 1 | 0.90 | 18 | Normal | 86 | 77 | +2.23 | +3.21 | 15.4 | 4 |
| 11 | 4 | 2 | 1.10 | 1 | 14 | D | 91 | 81 | +2.67 | +2.01 | 11.1 | 8.3 |
| 12 | 4 | 2 | 0.90 | 1.10 | 6 | A | 91 | 82 | −7.23 | −8.10 | 17.6 | 6.7 |
| 13 | 3 | 1 | 0.80 | 1 | 17 | C | 75 | 64 | +1 | +1 | 14.3 | 2.7 |
| 14 | 4 | 2 | 1 | 1.10 | 15 | A | 76 | 66 | +2.74 | +3.12 | 9.8 | 0 |
| 15 | 4 | 2 | 1.10 | 1 | 10 | B | 76 | 65 | +2.32 | +2 | 13 | 5.8 |
| 16 | 4 | 2 | 0.90 | 1.10 | 16 | C | 76 | 66 | +3.75 | +3.98 | 23.2 | 4 |
| 17 | 4 | 2 | 1 | 0.90 | 13 | A | 77 | 68 | +1.71 | +1.50 | 19.1 | 4 |
| 18 | 4 | 2 | 1.10 | 1.10 | 12 | Normal | 90 | 80 | +2.65 | +2.25 | 12.4 | 3.7 |
| 19 | 4 | 2 | 0.90 | 1 | 17 | C | 77 | 66 | +3.41 | +3.54 | 17.5 | 7.6 |
| 20 | 4 | 2 | 0.90 | 1.10 | 12 | Normal | 78 | 67 | +0.26 | +1.13 | 18.4 | 6.7 |
| 21 | 4 | 2 | 1.40 | 1.30 | 14 | A | 79 | 68 | +2.45 | +2.61 | 15.2 | 3.4 |
| 22 | 4 | 2 | 1.10 | 1 | 16 | A | 82 | 70 | +1.92 | +1.45 | 16.6 | 3 |
| 23 | 4 | 2 | 1.20 | 1 | 14 | A | 93 | 84 | +2.76 | +2.45 | 18 | 7.8 |
| 24 | 4 | 2 | 1.20 | 1.10 | 13 | B | 79 | 68 | +4.65 | +5.43 | 17.7 | 4 |
Final, final follow-up; MAD, mechanical axis deviation; MPFL, medial patellofemoral ligament; MQTFL, medial quadriceps tendon femoral ligament; PLG, passive lateral patellar glide; Pre, preoperative; PTA, patellar tilt angle; TT-TG, tibial tubercle-trochlear groove.
The passive lateral patellar glide was measured by dividing the patella into 4 quadrants; with each number representing the number of laterally displaced quadrants.
According to the Dejour classification.
Positive values indicate that the mechanical axis line of the lower limb in the frontal plane passes lateral to the center of the knee joint, and negative values indicate that the mechanical axis line of the lower limb in the frontal plane passes medial to the center of the knee joint.
Acknowledgements
Assem Mohamed Noureldin, the corresponding author, thanks his parents, Rania Ali Moharam, Ahmed Assem, Shady Assem, and Lareen Assem, for their great help and support in editing this article.
Final revision submitted March 19, 2024; accepted April 16, 2024.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Minia University (ref No. 872/10/2023).