
Abstract
Background:
Lateral patellar instability is common in young, active patients. Patients who fail conservative treatment may benefit from medial patellofemoral ligament (MPFL) reconstruction.
Indications:
Recurrent lateral patellar instability.
Technique Description:
Examination assesses patellar translation, eversion and range of instability. Diagnostic arthroscopy is performed for loose bodies, cartilage damage, trochlear dysplasia, and tracking. A longitudinal incision is made from superomedial to mid-body of the patella. The plane between the capsule and retinaculum is developed for palpation of the medial epicondyle and adductor tubercle. Electrocautery and rongeur are used to create a trough on the patella from centromedially to superomedially. Two suture anchors are placed at the proximal and distal trough. Fluoroscopy is utilized to identify Schöttle point with a perfect lateral radiograph. A 3-centimeter incision is made, and blunt dissection connects the 2 incisions in the developed plane. A guidepin is advanced at Schöttle point, and suture anchor sutures are shuttled through the plane, posterior to the guidepin. There should be loosening of tension with knee flexion. A semitendinosus allograft is whipstitched with terminal tapering. The whipstitched end is tunneled around the guidepin and brought back to the patella, so that both ends have an excess of 20 to 25 millimeters, and excess graft is trimmed from the free end prior to whipstitching. The doubled graft is sized. The midportion of the tendon is tagged and passed through both anchors. The graft is tensioned to the patellar trough and the graft ends are advanced through the developed plane. The femoral tunnel is reamed, and the graft is tensioned into the tunnel after nitinol wire placement with the knee in full extension. Isometry and lateral patellar translation are assessed, aiming for 1 quadrant with firm endpoint. The patella is proximalized and the tensioned graft is secured with an interference screw.
Results:
MPFL reconstruction is successful for the majority of patients, with 1.2% reporting instability, 3.6% apprehension, and 3.1% reoperation. Possible complications include patellar fracture, patellofemoral pain, and knee stiffness (loss of range of motion).
Discussion/Conclusion:
Lateral patellar instability is common, and MPFL reconstruction is typically successful for the majority of patients.
This is a visual representation of the abstract.
Keywords
Video Transcript
This video covers our technique for medial patellofemoral ligament reconstruction utilizing a hamstring allograft.
The authors disclosures are listed here as well as available online.
In general, lateral patellar instability is common in patients that are young and active and, when they fail conservative management, can benefit from surgical treatment, which most commonly involves reconstruction of the medial patellofemoral ligament.
Before we get into the medial patellofemoral ligament reconstruction technique, it is important to understand a few anatomy aspects to help guide our reconstruction. First, the medial patellofemoral ligament is part of the medial patellofemoral complex, which also includes the medial quadriceps tendon femoral ligament. This medial quadriceps tendon femoral ligament (MQTFL) has been described by Fulkerson, Corey Edgar, as well as Miho Tanaka, and is present on almost all specimens that were dissected in anatomic studies.
When looking at these the medial patellofemoral ligament (MPFL) inserts at the proximal half of the osseous component of the patella and the MQTFL inserts just proximal to patella extending 1 centimeter into the quadriceps tendon with all soft tissue attachment. It is important to understand the difference in the length changes of these 2 ligaments, as well as their relative biomechanical contribution.
When we look at the change in length between the femoral attachment in these 4 attachments seen to the left, we can see that at the distal most attachment at the midbody that patella from 0 to 90° of flexion, there’s only 2.5 millimeters of lengthening that occurs at this location. This is in contrast to the most proximal aspect of the MQTFL, which lengthens approximately 12 millimeters from 0 to 90° of flexion most notably these changes happen within the 1st 40° of flexion and so the more proximal grafts loosen to a higher extent and also more quickly. Based on this, the recommendation for our technique is to have each limb have separate isometric or anisometric changes. When we then add the biomechanical contribution looking at a sequential sectioning study seen here, we can see the MPFL under tension has more stout attachments that are more well defined, versus the MQTFL which has a larger band like broad insertion on the femur as well as in the quadriceps tendon.
When we look at the effect of sectioning and its relative effect from intact, the approach for this study was performed the lateral release, and there was increased lateral translation with a lateral release alone. When there was sectioning of the medial patellofemoral complex proximally, or the MQTFL, there was no significant increase in lateral translation. However, when the MPFL was sectioned in isolation, there was a significant increase in lateral translation. In the MQTFL, only increased lateral translation when the MPFL was also sectioned, demonstrating they likely have a synergistic effect.
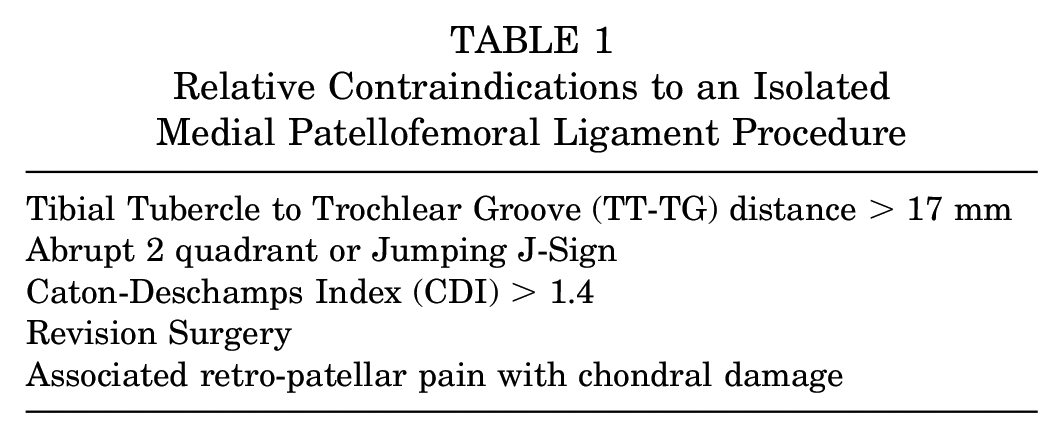
The ways that this information guides our surgical reconstruction is that the proximal distal extent to the medial patellofemoral complex have significantly different length changes, and we’d like to have those sets separately within the surgical technique when we use a 2-limb reconstruction. The longest distance for all points is in full extension, therefore we set the length of the graft in full extension in the operating room. We know that the MPFL is the primary restraint to lateral patellar translation, and so this technique will cover an osseous based MPFL reconstruction (Table 1).
Relative Contraindications to an Isolated Medial Patellofemoral Ligament Procedure
The procedure starts with an examination under anesthesia looking at lateral and medial translation, as compared with the contralateral side. We also evaluate for medial and lateral eversion. We look to see where instability disappears, as we flex the knee which gives us an idea of associated osseous pathology. We start with the diagnostic arthroscopy looking for loose pieces and cartilage damage. Here we extend the knee while in the notch to look at overall trochlear dysplasia, which demonstrates a hypoplastic medial trochlea in this situation.
After this is complete we then start our open approach, which we based on the mid-body of the patella and the superior medial corner, and we inside sharply through skin here using the superior half of the patella as our landmark. After we incise through skin we use blunt and sharp dissection to get down to layers 1 and 2, which we eventually will incise using a 15-blade knife. This is done utilizing a tourniquet so that we can easily visualize these planes. We then dissect superficial to the capsule and deep to the retinaculum in an anterior to posterior fashion, making sure that we stay extra capsular and keep the retinacular layers separate.
In the setting of an ossicle in this area or revision, sometimes a knife is necessary to develop these planes. We should have an entry large enough to place your finger to be able to palpate the medial epicondyle, as well as the adductor tubercle. We then bovie down on the superomedial aspect of the patella, taking care to make sure that we know where the articular surface in the anterior aspect of the patella lies. Once we have this defined, we use a rongeur to develop a trough between the 2 planned anchor sites.
Here we’re using 3-millimeter peek knotless anchors where we drill making sure we feel where the lateral edge of the patella is so we are not exiting anteriorly or deep into the cartilage. Here we can see that at the 50 yard line, and we place the second anchor at the superior medial pole of the patella so that we can span the native osseous insertion of the medial patellofemoral complex, which is where the medial patellofemoral ligament lies. We then place a second knotless anchor and pull to make sure that these have excellent fixation.
After this is complete, we that move on to our femoral component where we use for fluoroscopy to localize the anatomic location based on a perfect lateral radiograph. It’s crucial to make sure that we have the correct rotation, as well as overall coronal alignment to first get posterior condylar overlap and then posterior proximal condylar overlap. We then utilize Schöttle point to localize our skin incision using the landmarks described in the figure above. We check fluoroscopic location using a hemostat and we localize a 3 centimeter incision in this area. We dissect sharply, then use 1 dissection from the plan we had previously developed to connect these 2 areas.
After this has been open you can easily palpate the medial epicondyle and adductor tubercle and you can use this to temporarily place your guide pin the planned location. After this is placed we check this on fluoroscopy. We then take the sutures posterior to the pin coming from the patella, and as we go through the range of motion we should see obvious loosening with flexion. We then prepare a semitendinosis graft on the back table using a whip stitch on a single end of the tendon making sure it’s very well tapered. After the stitches are in place we then bring the tendon over to the body where we bring it underneath the guide pin that we had already placed and even though the looped end will be on the patella in the end, we bring the looped end around the pin and overlap at least 20 to 25 millimeters of tendon over the patella and mark this with a pen. This will tell us how much tendon we should have within our tunnel and after we reem our tunnel, we then trim the tendon to this length. We taper the tendon as well and use another whipstitch with a nonabsorbable suture making sure that we have extremely easy graft passage.
If this is a snug 7, then we will drill at 8. If it is a very easy 7 then we will drill 7. Making sure that it’s very easy to get the graft in the tunnel helps prevent over constraint. We then mark the midportion of the tendon, as this looped and will be placed on the patellar side. We use a free needle to use the knotless suture in a simple suture configuration going around as much graft tissue as possible. After both of these are placed, this tissue stitch is then brought into the knotless suture loops that will pass the tissue stitch through the anchor. These sutures and anchor configuration are very robust. A knotted anchor can also be used. Also, all suture anchors have also been utilized in the patella. However, the authors recommend bodied anchors due to the improved reliability of their deployment and overall fixation strength.
After both of these are passed we then pull each of these sequentially to bring the graft down to the patella, so that the central component is now draped over the trough that we had rongeured. We then take the sutures from the free ends of the graft keeping them separate; they pull them through the femoral insertion; knowing which graft is slightly larger is the one that will pass through the tunnel first.
Here we can be seen reeming the graft tunnel on the femur making sure the aperture is very forgiving. We place a passing stitch, as well as the nitinol wire, where screw will eventually be screwed over this, making sure that we stay within the tunnel. It’s important to put the nitinol wire in place before the graft has passed. We then take the graft sutures and the passing stitch and pass these through for the eventual insertion of the graft into the femoral tunnel. These should be pulled sequentially again starting with the bulkier end of the graft. Once these are placed this is done in full extension with the patella proximalized to try to put the graft at its longest position; after this is placed, we then take the knee through a full range of motion to make sure that if any mistakes were made we allowed the graft to get to the lowest common denominator.
We should feel 1A of lateral translation we proximalize the patella and then placed a in this case 7 by 23 peak interference screw for the final fixation. Arthroscopic examination then demonstrates the graph should be 2 bundles and extra articular as planned.
Postoperatively patients are allowed weight bearing with a brace locked in extension until their quadriceps is strong enough to allow them to walk with the brace unlocked. We start physical therapy immediately and try to get a minimum of 15° of flexion per week, and we discontinue the brace at 6 weeks. Working on running and more cutting in pivoting activities at 3 to 4 months after surgery, with hope to return to full activity at 4 to 6 months after surgery.
When we look at the outcomes, the overall risk of recurrent instability after medial patellofemoral ligament reconstruction is 1.2%. Having apprehension still postoperatively on examination is just over 3%. And the overall reoperation rate is again 3%. This demonstrates that the overall success of isolated MPFL reconstruction is very high.
When we start to look at outcomes relative to risk factors and recurrent surgery or redislocation after isolated medial patellofemoral ligament reconstruction, one of the factors that seems to be the most significantly associated with failure is unaddressed trochlear dysplasia, even more so than an incorrect femoral tunnel placement, specifically in regard to recurrent instability. However multiple studies have shown different risk factors that could be relevant though each study did not control for the same factors.
When we look at return to sport there is a time-based improvement, where the further out the patients are the more likely they are to have returned to sport and most commonly return to sport was observed at 6 months after surgery.
References for this presentation can be seen here.
Thank you very much for allowing us to present this technique on medial patellofemoral ligament reconstruction with hamstring allograft.
Footnotes
Submitted October 26, 2021; accepted March 18, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.B.Y. received grants from Organogenesis and Vericel; received grants from Arthrex, Inc., and Aastrom Biosciences Inc. outside the submitted work; received personal fees from JRF Ortho,Olympus, and CONMED Linvatec; received non-financial support from Smith and received non-financial support and other from Patient IQ. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.