
Abstract
Background:
Meniscal repair has been associated with long-term benefit in patients compared with meniscectomy. As a generalization, meniscal repair in older patients is less likely to be successful, leading to reduced adoption of meniscal repair compared with younger patients.
Purpose:
To establish the clinical performance of meniscal repair in “older” patients (age, ≥40 years) and compare it with performance in “younger” patients (age, <40 years).
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic literature review was performed in September 2021 using Embase and PubMed to identify published English-language studies that reported on a meniscal repair in >5 patients aged ≥40 years. Outcomes of interest were success/failure rate (as defined by the study), revision meniscal procedure rate, and patient-reported outcomes. Meta-analyses were used to synthesize outcomes across all studies in older patients. Meta-analyses were also used to compare outcomes between older and younger patients across studies, providing data on both age groups.
Results:
Fourteen studies were identified. Meniscal repair in older patients was determined to have a failure rate of 12% (95% CI, 7.3% to 19.4%) and a revision meniscal procedure rate of 9.8% (95% CI, 6.2% to 15.0%). The postoperative Lysholm score was 86.7 (95% CI, 81.7 to 91.7). No statistically significant differences were observed between older and younger patients in failure rate (relative risk [RR], 0.73 [95% CI, 0.44 to 1.21]; P = .2205), revision meniscal procedure rate (RR, 0.69 [95% CI, 0.41 to 1.16]; P = .1613), or Lysholm scores (mean difference, 2.3 [95% CI, –4.7 to 9.2]; P = .5278, 4 studies).
Conclusion:
Meniscal repair in selected patients aged ≥40 years resulted in good success rates and patient-reported outcome measures, which appear similar to those reported for patients aged <40 years. Therefore, meniscal repairs can be performed in at least a specific portion of “older” patients, and age per se should not be the sole determining factor in whether to perform a meniscal repair.
Meniscal tears are one of the most common soft tissue injuries of the knee.5,19 Historically, the standard of care for meniscal tears has been a total or partial meniscectomy; however, removing meniscal tissue results in a decreased joint contact area and increased joint contact pressures.18,27 These changes in joint biomechanics are believed to contribute to cartilage degeneration, leading to an increased risk of osteoarthritis and subsequent need for total knee arthroplasty.1,21,28,29,39,40,55 Consequently, an emphasis has been placed on preserving meniscal tissue through implementing meniscal repair, which has been demonstrated to maintain or restore normal joint biomechanics.18,27 Compared with meniscectomy, meniscal repair has been associated with a significantly lower risk of degenerative cartilage changes,40,55 lower risk of total knee arthroplasty, 49 and better patient-reported outcome measures (PROMs)28,55 in the longterm.
Meniscal repair appears to be more commonly accepted as the standard of care in younger patients.40,50 As a generalization, meniscal repair in older patients is less likely to be successful due to reduced vascularity across the meniscus and an increased likelihood of degenerative tears.32,41 There is also a belief that the long-term benefits of meniscal repair, stemming from minimizing degenerative cartilage changes, may not be as impactful in older patients, as they are more likely to present with degenerative changes in the knee. This thinking leads to many considering older age as a contraindication for meniscal repair in their surgical practice.
A European meniscus consensus, established by the European Society of Sports Traumatology, Knee Surgery, and Arthroscopy, identified that patient age does not appear to affect the failure rate of repair of a traumatic meniscal tear. 24 However, it was noted that the degeneration of the meniscal tissue in older patients should be considered. A systematic review reported a pooled meniscal repair failure rate of 10% across studies in patients aged ≥40 years, stating that this rate is similar to rates reported for younger patients. 16 A second systematic review reported that older age did not increase failure rates. 47 However, these previous systematic reviews were limited by a small sample size, an inconsistent definition of failure across studies, and a lack of meta-analytic techniques to pool data across studies in a valid manner.
Therefore, this study aimed to establish the failure rate and PROMs after meniscal repair in “older” (≥40 years old) patients and how these outcomes differed from those in younger (<40 years old) patients. Meniscal repair failure was defined per each study as in prior systematic reviews16,47 but also defined as the need for a second meniscal surgery on the same meniscus, providing a consistent measure of failure across studies. The use of 40 years of age as a threshold was implemented based on the precedent set in a previous systematic literature review. 16
Methods
This systematic review of the literature with meta-analysis was performed and written in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 38
Search Strategy
This systematic literature review was performed using 2 previously published systematic literature reviews,16,47 which investigated the effect of older age on meniscal repair outcomes considering articles published up to 2017, followed by an updated systematic literature search. 12 The updated systematic literature search was performed using PubMed and Embase on September 29, 2021, with a search string of “("meniscus repair" OR "meniscal repair") AND (age OR old OR older)” and limits set to consider publications from 2017 in the English language. Reference lists of included studies and systematic literature reviews were also considered.
Articles identified during the execution of the search strategy, both from previous systematic literature reviews and the updated literature search, were screened for suitability: first based on the title and abstract and second based on the full text. For a study to be considered relevant for inclusion, it had to report on the outcomes of a group of patients (n >5) with all patients aged ≥40 years undergoing meniscal repair of a meniscal tear (excluding repair of a root tear), with or without concomitant cartilage or ligament surgery. Outcomes of interest were the success (or failure) rate as defined by the individual study, the rate of revision meniscectomy or meniscal repair, and PROMs. Both comparative and noncomparative study designs were included. In addition, for a study to be included, it had to be a full-text publication and an original piece of primary research.
Data Extraction
For all articles identified for inclusion, data associated with the study, patient, and surgical procedure characteristics, along with outcome data, were extracted into a predefined data extraction table by 1 reviewer and checked for accuracy by a second reviewer (M.J.S., C.S.). Study characteristics included author name, year of publication, study design, and sample size. Patient characteristics included age at the time of surgery, along with type, location, and chronicity of meniscal tear. A small/large tear was classified using a 2-cm long threshold, and an acute/chronic tear was considered using a 6- to 10-week threshold. Surgical characteristics included meniscal repair technique, meniscal repair device, and concomitant procedures. The incidence of meniscal repair success and failure—as defined by the individual study, incidence of revision meniscal surgery (meniscal repair and/or meniscectomy), and measure of central tendency and spread for PROMs (Lysholm)—were extracted. In addition, the study definition of success/failure and follow-up time were extracted.
Quality Assessment
Each included study's risk of bias was assessed. For studies in the analysis of outcomes between patients aged ≥40 years and <40 years, the Risk Of Bias In Non-randomized Studies - of Exposure was utilized. 45 For all studies in the analysis associated with outcomes in patients aged ≥40 years, only the Institute of Health Economics Quality Appraisal for Case Series Studies Checklist was utilized. 43
Data Analysis
Meta-analysis was performed in R Version 4.0.2 (R Foundation for Statistical Computing) using the “meta” package. Statistical significance was set at an alpha level of 0.05. Meta-analysis was performed to pool meniscal repair outcomes in “older” patients across studies, providing a mean and 95% CI. Meta-analysis was also performed to compare meniscal repair outcomes between the “older” and “younger” patients reporting a mean difference (PROMs) or relative risk (failure) and 95% CI. The heterogeneity of included studies was assessed using the I 2 statistic. A random effects model was utilized throughout because of heterogeneity between studies. 14 Forest plots were used to display individual studies and heterogeneity visually.
Where data on the mean and standard deviation were not provided but an alternative measure of central tendency and spread was available, these data were transformed to the mean and standard deviation using validated methods. 59 Where no measure of the spread of data was available, standard deviations inputted as the mean of other standard deviations within the analysis, as has been done by others previously. 31
Brelin et al 7 defined failure as revision surgery, including subsequent meniscal repair or meniscectomy, and also meniscal transplant and total knee arthroplasty; however, because the latter 2 procedures only accounted for <1% of subsequent surgeries, this study was considered valid to be included in the analysis.
Sensitivity and publication bias analyses were performed to assess the robustness of the meta-analyses. Sensitivity analysis was conducted through leave-one-out analysis to ensure the robustness of findings. In addition, data extracted from Brelin et al 7 considered an age threshold of 45 years, and sensitivity testing also considered an age threshold of 35 years. The potential for publication bias was assessed through funnel plots and the Egger test.
In addition, the proportion of meniscal repairs and failure rate were established for the given patient, as well as the surgical characteristics in “older” patients. Characteristics included meniscus laterality, tear type, tear size, chronicity of injury, tear location, repair technique, and anterior cruciate ligament (ACL) status. Where a case or failure could not be attributed to a characteristic, it was identified as unclassified.
Results
Study Characteristics
A total of 14 relevant articles were included in this systematic literature review (Figure 1). ¶ Of the 11 articles previously included in the systematic review by Everhart et al, 16 4 were not included, as they lacked a sufficient sample size.20,54,56,58 Of the 5 articles previously included in the systematic review by Rothermel et al, 47 3 were not included, as they were duplicates already considered,2,51,54 and 1 was not included because of insufficient sample size. 25 Six articles were included from the updated systematic literature search.7,9,22,30,42,46 Two articles may appear to meet the inclusion criteria; however, they were excluded due to 15% of “older” cases being root tears.15,17
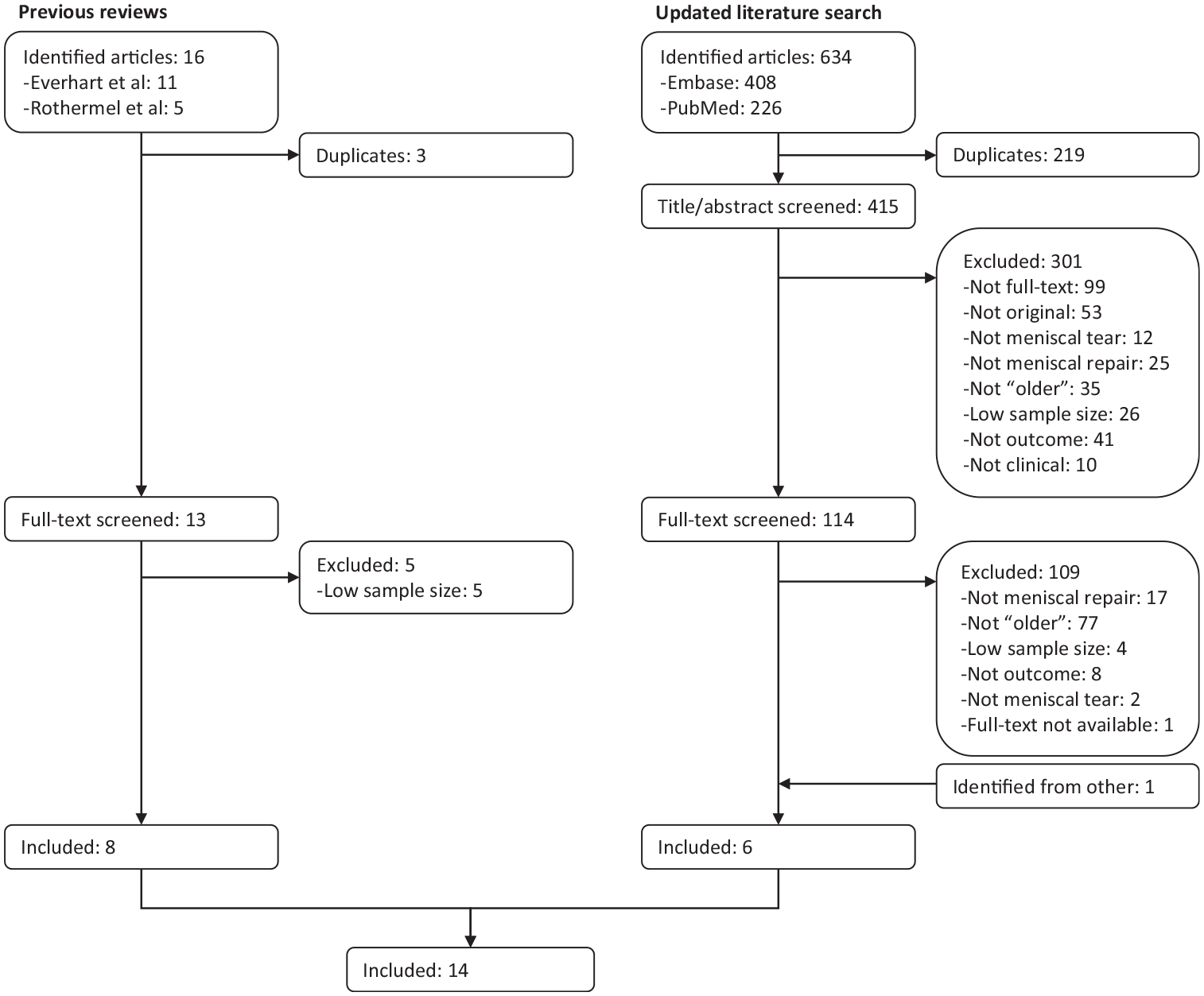
Study selection flowchart.
Two articles had minor overlap in patients (one “older” patient and 3 “younger” patients)52,53 and were considered independent studies. Finally, Brelin et al 7 reported on an age threshold of 45 years for “older” patients and was included in the analysis.
Six articles were of a retrospective cohort design,7,22,30,42,46,51 5 were of a retrospective case-series design providing individual patient data sufficient to compare “younger” and “older” patients,2,23,44,52,53 and 3 articles were prospective case-series only considering “older” patients.6,9,36 Individual study characteristics are presented in Table 1 and further expanded in Supplemental Table S1.
Characteristics of Included Studies a

ACL, anterior cruciate ligament; ACLR, concomitant anterior cruciate ligament reconstruction.
Provided individual patient data to allow for within study comparison between “younger” and “older” patients.
Risk of Bias
Eleven studies compared outcomes between older and younger patients after meniscal repair.2,7,22,23,30,42,44,46,51-53 Risk of bias is presented in Supplemental Table S2. A high risk of bias due to confounding may be apparent across studies with limited data on patient characteristics between younger and older patient groups that may affect outcomes. Furthermore, there may be some concerns about the risk of bias due to the selection of participants, such that the decision to perform meniscal repair may be based on different criteria for younger and older patients, affecting outcomes.
All studies provided a case-series to evaluate the outcome in older patients. The quality of these case-series is presented in Supplemental Table S3. Common areas of concern across the studies were a lack of prospective designs, a lack of multicenter data collection, a lack of complete inclusion and exclusion criteria, and that each case-series showed high heterogeneity in characteristics, suggesting patients may not have entered each study at a similar disease point. There was also a lack of clarity around the intervention, with many simply referring to meniscal repair.
Meniscal Repair and Revisions in Older Patients
Across the studies, 466 “older” patients were identified as having undergone meniscal repair (Table 2). In addition, Lyman et al 30 reported on “older” patients who underwent meniscal repair; however, the patient number could not be ascertained. The mean age range of “older” patients across the studies ranged from 44.2 years 6 to 52.5 years, 44 with the maximum ages reported ranging from 50 years 6 to 70 years. 51
Distribution of Meniscal Repairs and Revision Rates in Older Patients a

Data are presented by patient, tear, and surgery characteristics. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; NC, not calculable; RR, red-red zone; RW, red-white zone; WW, white-white zone.
Table 2 summarizes the characteristics of “older” patients receiving meniscal repair. There was a larger number of repairs performed on the medial menisci compared with the lateral menisci (74.9% vs 22.9%), vertical/longitudinal tears to complex/horizontal and radial tears (86.5% vs. 9.5% vs 4%), and tears in the vascularized zone than with an avascular portion or solely in an avascular zone (red-red zone 57.7% vs red-red zone with avascular portion 22.8% vs red-white zone 17.5% vs white-white zone 2.1%). Repairs were most common using an inside-out approach (64.3%) and in patients with either an intact ACL or those who underwent concomitant ACL reconstruction (55.2% and 42.7%). There was a substantial volume of undefined meniscal repairs such that 31% to 92% of patients were not accounted for in each characteristic.
Success/Failure as Defined by Individual Study
The definitions of meniscal repair failure varied across the included studies. Meniscal repair failure definitions included clinical failure determined through physical assessment,6,9,23 failed meniscus healing determined through magnetic resonance imaging (MRI) or second-look arthroscopy,2,9 the need for subsequent surgery,7,22,30,46,51 poor PROMs postoperatively,44,53 a combination of meniscus healing and subsequent surgery, 42 a combination of clinical symptoms and meniscus healing, 36 and a combination of PROMs and subsequent surgery. 52 MRI or second-look arthroscopy leading to the definition of failed meniscus healing was most commonly performed in symptomatic patients,2,36,42 with only Buyukkuscu et al 9 performing radiographic imaging systematically across all patients. Using the studies’ definitions of failure, a total of 58 meniscal repair failures were reported across the studies for the “older” patients, and proportional meta-analysis revealed a mean meniscal repair failure rate of 12% (95% CI, 7.3%-19.4%) (Figure 2). Meta-analysis of comparative studies showed a lower risk of a meniscal repair failure in “older” than younger patients; however, this failed to reach statistical significance (relative risk [RR], 0.73 [95% CI, 0.44-1.21]; P = .2205) (Figure 2).

(A) Meniscal failure rate, as defined by individual studies, in “older” patients and (B) in comparison with “younger” patients. RR, relative risk.
Table 2 presents pooled failure rates in “older” patients by characteristic. Meniscal repair failures were more common when the medial meniscus was repaired over the lateral meniscus (19.8% vs 11.5%) and when the repair was of a horizontal/complex tear than a vertical/longitudinal tear (41.7% vs 15.6%, respectively). Failure rates were lower for repair of tears in the vascular (red-red) zone only or with an avascular portion (10.4% and 12.9%, respectively) compared with tears in lower vascularity zones (red-white zone, 21.4% and white-white-zone, 50%). Smaller tears and acute tears had lower failure rates than longer tears and chronic tears (10% vs 17.6% and 9.8% vs 26.1%, respectively). Meniscal repair performed in conjunction with ACL reconstruction had a lower failure rate than when the ACL was intact, and in turn, both repairs had higher failure rates than when the ACL was deficient and not addressed (7.1% vs 23.9% vs 40%, respectively). A substantial number of failures were missing data and, therefore, unable to be associated with specific factors (45% to 91% of failures); thus, statistical analyses were deemed inappropriate.
Success/Failure as Defined by Revision Meniscal Repair or Meniscectomy
Nine studies provided sufficient information to consider failure specifically as a revision meniscal repair or meniscectomy in meta-analysis.2,6,7,22,36,42,46,51,52 Meta-analysis identified a repeat meniscal repair incidence rate of 9.8% (95% CI, 6.2%-15.0%) in “older” patients (Figure 3). Seven comparative studies also provided data amenable for meta-analysis comparing failure rates between older and younger patients and revealed there were trends for older patients to be less likely to experience failure; however, this difference did not reach statistical significance (Figure 3) (RR, 0.69 [95% CI, 0.41-1.16]; P = .1613).2,7,22,42,46,51,52

(A) Meniscal failure rate, as defined by meniscus reoperation, in “older” patients and (B) compared with “younger” patients. RR, relative risk.
In addition, Lyman et al 30 reported on relevant data that were not amenable to meta-analysis, observing that patients aged ≥40 years were less likely to experience failure (ie, were less likely to require future meniscectomy) compared with patients aged <20 years after an isolated meniscal repair (hazard ratio [HR], 0.53 [95% CI, 0.40-0.70]; P < .001) but not after meniscal repair with concomitant ACL reconstruction (HR, 0.99 [95% CI, 0.71-1.37]; P = .927). Analysis was not performed on patients aged ≥40 years and other age categorizations.
Patient-Reported Outcome Measures
Lysholm score was the most common measure present in 4 studies.9,22,23,51 Proportional meta-analysis identified a mean postoperative Lysholm score of 86.7 (95% CI, 81.7 to 91.7) in older patients. Meta-analysis performed on postoperative Lysholm scores identified no statistically significant difference between older and younger patients (mean difference, 2.3 [95% CI, –4.7 to 9.2]; P = .5278).
Sensitivity and Publication Analysis
Funnel plots on failure rates were broadly symmetrical and, when combined with nonsignificant Egger tests (P > .05), suggested a low probability of publication bias (Supplemental Figures S1 and S2). Studies reporting on meniscal repair failure, as defined by each individual study, tended to demonstrate relatively high failure rates in small case-series and low failure rates in larger case-series. This was not observed for meniscal repair failure defined as a revision procedure.
Leave-one-out sensitivity analysis had minimal impact on the aggregated failure rates in “older” patients. The meniscal repair failure rate, as defined by individual studies and as revision, was between 11.3% and 14.2% and between 8.6% and 12.7%, respectively. Furthermore, including patients aged ≥35 years as older from Brelin et al 7 had minimal effects on meniscal repair failure rate as defined by individual studies or as revision (13.4% and 9.5%, respectively). Finally, sensitivity analysis had minimal effect on effect sizes when comparing “older” patients to “younger” patients.
Discussion
The most important finding of this systematic literature review was that the failure rates of meniscal repair in patients aged ≥40 years were 12.6% and 9.8% when failure was defined per each study or, more specifically, as a need for a second meniscal procedure, respectively. The likelihood of failure was also not statistically different in patients aged ≥40 years compared with those aged <40 years. These results indicate that meniscal repair can be performed in “older” patients through diligent patient selection.
The observed failure rate of meniscal repair in older patients is in line with, or at the lower end of, rates reported in systematic reviews considering the wider population.4,11,13,26,33-35,37,48 These previous reviews13,35,37,48 have reported failure rates across all tear types of 12% to 23%, bucket handle tears4,11 of 15% to 29%, horizontal cleavage tears26,34 of 12% to 26%, and radial tears 33 of 8%. The present systematic literature review also identified the rate of meniscal repair failure to be lower, but not statistically different, in “older” patients than “younger” patients. Data on patient activity levels were poorly reported across the included studies; however, the observed low failure rates may be a consequence of confounding with “older” patients being less physically active than their “younger” counterparts, placing the meniscus under less stress and, thus, minimizing the opportunity for failure. In addition, a common limitation identified across the included studies was a risk of selection bias, such that a more stringent surgeon selection process to determine which patients receive a meniscal repair may have been present for “older” patients, which could lead to a higher likelihood of success. Surgeons are likely more aggressive in their decision-making to perform meniscal repair in younger patients and reserve meniscal repair in older patients when there is high confidence in meniscal healing. The chondroprotective benefits and reduced risk of future knee arthroplasty associated with meniscal repair over meniscectomy may be more impactful in younger patients over older patients who are more likely to present with degenerative changes in the knee. Notably, the avoidance of knee arthroplasty in younger patients is critical, as joint survivorship is known to be reduced. 3 Despite the view that meniscal repair may be less successful in “older” patients, the present review demonstrates that meniscal repairs can be performed in at least a specific portion of “older” patients and that age per se should not be a determining factor in whether to perform a meniscal repair. Instead, other factors associated with the patient, such as their knee and tear, should be considered.
The present review observed quantitatively lower failure rates in “older” patients when the repair was performed on a lateral meniscal tear, a small tear, an acute tear, a tear in a high vascularity zone, and a vertical/longitudinal tear. Lower failure rates were also apparent in patients undergoing meniscal repair using an all-inside technique and undergoing a meniscal repair with a concomitant ACL reconstruction. Blood supply is recognized as needed for meniscus healing and successful outcomes. This may account for the lower failure rate observed for repairs in the lateral meniscus, 49 the red-red zone, and concomitant ACL reconstruction. However, previous systematic literature reviews have not identified any significant difference in failure rates based on meniscus laterality, tear type, tear chronicity, tear vascularity, or ACL status.35,48 In addition, research has observed that the entire meniscus, including the white-white zone, has a level of vascularity and resident mesenchymal progenitor cells, indicating the potential for meniscal repair even in the white-white zone. 10 Schweizer et al 48 observed a higher failure rate with all-inside techniques; however, when only modern all-inside devices are considered, failure rates are not significantly different from those associated with inside-out repair.35,57 Decisions based on these potentially influencing characteristics should be made cautiously because of substantial missing data to allocate tear characteristics with failure and a large reliance on between-study comparisons. Therefore, future research would be valuable to investigate determinants of meniscal repair failure in older patients covering a heterogeneous population to inform effective patient selection providing greater clarity on who is a good candidate for repair.
The method of determining meniscal repair failure across individual clinical studies and systematic literature reviews shows substantial variation, including observation of meniscus healing via MRI or second-look arthroscopy, return of clinical symptoms indicative of a meniscal tear, or reoperation (any or specific to the area of the original tear). These heterogeneous methods may explain some of the variation in rates reported across studies, and their amalgamation has previously been identified as a limitation of previous systematic reviews.16,47 Also, the definition of meniscal repair failure used by an individual study may determine outcomes, with a recent study documenting complete healing to be significantly higher in “younger” patients; however, differences were not evident when considering failed healing. 13 As patients may not demonstrate healing but may be asymptomatic with good function, focusing on successful outcomes based on the need for meniscal reoperation and PROMs may be pertinent.
This systematic literature review identified a mean postoperative Lysholm score of 86.7 in older patients, respectively. This Lysholm score is in line with the mean score reported across 488 participants with no history of injury or surgery and a mean age of 41 years. 8 Furthermore, meta-analysis identified no statistical difference in postoperative Lysholm score between “older” and “younger” patients. While some studies did report differences in postoperative scores, differences were not apparent after controlling for confounding factors (namely, preinjury activity level) and the known effect of age on the outcome measures. 16
The paradigm shift toward meniscus preservation has been driven by the observation that the high risk of osteoarthritis and knee arthroplasty after meniscectomy is to be minimized through meniscal repair.40,50 Older patients are naturally more likely to be further along the degenerative process and consequently have cartilage damage or osteoarthritis during meniscal surgery; thus, the benefit of meniscal repair may be smaller in these patients. Two studies reported no changes in osteoarthritis grading, including in patients with abnormal cartilage, after meniscal repair in the “older” patients at a mean follow-up time of 24 months (range, 16-36 months) 9 and 31.1 months (range, 12-100 months). 36 Therefore, the chondroprotective effect of meniscal repair may also be observed in these populations.
Limitations
The evidence used in this systematic literature review is not without limitations. First, the included studies typically had lower levels of evidence in the form of retrospective cohort analysis and case-series; however, they represent the best available evidence to inform clinical practice related to meniscal repair in “older” populations. Second, the included studies were identified to have the potential risk of selection bias and, consequently, confounding bias, which may lead to low failure rates in older patients. Associated with this, there was a lack of data on potentially confounding factors, including articular cartilage status, body mass index, activity level, alignment, and tear characteristics, limiting the ability to understand which patients specifically are likely to have a successful meniscal repair and contrasting results between individual studies. Third, most included studies included relatively small sample sizes. These small sample sizes may limit the ability to sensitively detect failure rates, with a single event having a large impact on study observations. These small sample sizes limit deeper analysis of factors other than age, which may affect failure rates. Fourth, although data on the benefit of meniscal repair were apparent in studies in the form of patient-reported outcomes, they were limited to a small number of studies, and data demonstrating the chondroprotective effects were even sparser. Fifth, the included articles may be from a select pool of experienced surgeons who select and repair meniscal tears in older patients, such that a level of publication bias cannot be eliminated and the results may not be generalizable to all surgeons. Further, the methods used in this systematic literature review are also not without limitation. Although an attempt was made to standardize the definition of failure as a revision meniscal procedure, this may introduce a risk of bias with a different surgeon- and patient-induced threshold between younger and older patients to return to the operating room for such a procedure. Despite these limitations, this study is offered to raise awareness and encourage further research in the growing field of meniscal preservation to ensure that all patients receive the best treatment.
Conclusion
Meniscal repair can be performed successfully with a low failure rate and good PROMs in “older” patients. It is unclear if these outcomes are equivalent to those in “younger” patients, as selection bias in surgeon decision-making may confound observations; nonetheless, it is apparent that successful meniscal repair procedures can be performed in this age group through diligent patient selection. Therefore, age per se should not be a primary or sole factor in deciding whether to perform meniscal repair.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241258974 – Supplemental material for Systematic Review and Meta-analysis of Clinical Outcomes Following Meniscus Repair in Patients 40 Years and Older
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241258974 for Systematic Review and Meta-analysis of Clinical Outcomes Following Meniscus Repair in Patients 40 Years and Older by Matthew J. Sedgwick, Christopher Saunders and Alan M.J. Getgood in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgements
The authors would like to thank Anna Brynskikh, a paid employee of Smith+Nephew, who provided editorial support for the final manuscript.
Final revision submitted December 5, 2023; accepted January 1, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.M.J.G. is a paid consultant of Smith+Nephew and received funds for the completion of this work; received reimbursement from Smith+Nephew for attending a symposium; received a fee from Smith+ Nephew for speaking or for organizing an educational program; received a payment to write a paper from Smith+Nephew; received funds for research from Smith+Nephew; received funds for Clinical Fellow from Smith+Nephew; received royalties or fees for consulting from Smith+Nephew; receives research support from Ossur; owns stock of LinkX Robotics, Ostesys Robotics, and Spring Loaded Technologies, as well as Precision OS stock options. M.J.S. is a paid employee of Smith+Nephew. C.S. is a paid employee of Smith+Nephew. No sponsorship was received for this work; however, the work was performed as normal work of M.J.S. and C.S. as paid employees of Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.