
Abstract
Background:
Anterior labrum periosteal sleeve avulsion (ALPSA) lesion of the shoulder is defined as a labral avulsion with an intact periosteum of the glenoid neck resulting in medial malattachment of the labrum, which is both nonanatomic and nonfunctional. It is relatively rare compared with Bankart lesions, and its results are usually reported in combination with other anterior labroligamentous lesions in the literature.
Purpose:
To (1) assess the size and scope of the literature on ALPSA lesions, (2) highlight the importance of this lesion, and (3) distinguish between ALPSA and Bankart lesions in diagnostic and treatment strategies.
Study Design:
Scoping review; Level of evidence, 4.
Methods:
The PubMed, Scopus, Embase, and Google Scholar databases were searched with the keywords “ALPSA,”“anterior labrum periosteal sleeve avulsion,”“anterior labral periosteal sleeve avulsion,” and “anterior labroligamentous periosteal sleeve avulsion” lesion. Duplicate articles and those that did not meet the inclusion criteria were excluded, resulting in the identification of 42 relevant articles. Their references were analyzed for further data curation.
Results:
This scoping review demonstrated that ALPSA lesions are difficult to clinically identify. Magnetic resonance angiography in the adduction internal rotation position is the most sensitive and specific imaging modality for identification. Optimal views are the anterosuperior portal for accurate identification and the anteroinferior portal for surgical repair during arthroscopy. Treatment begins with correctly identifying the labrum, in contradistinction to dense reactive fibrous tissue, and reattaching the labrum to the correct anatomic glenoid footprint. Chronic lesions with bone loss require either bone block or soft tissue augmentation procedures.
Conclusion:
There is paucity of exclusive literature on ALPSA lesions. It is important to distinguish this lesion from the Bankart lesion as it is associated with worse outcomes. The higher failure rates of ALPSA lesion repair indicate that the current repair techniques require further refinement to improve the outcomes to the standard of Bankart lesions.
Keywords
The anterior inferior glenohumeral ligament (IGHL) serves as the primary static restraint against anterior translation of the shoulder when the arm is in 90° of abduction and external rotation and also limits passive range of external rotation in the scapular plane. 21 Many authors have found that when the arm is placed at 90° of elevation in the scapular plane, increasing external rotation tightens the IGHL complex. 7 Studies have proven that shortening the capsular tissue within this area causes a decrease in external rotation. 37
The shoulder joint is the most dislocated joint in the body, with anteroinferior glenohumeral dislocation being the most prevalent type. 20 The labrum and capsuloligamentous structures (static stabilizers) along with the rotator cuff and pericapsular muscles (dynamic stabilizers) are avulsed and torn during such a traumatic injury.15,18 The lesions occurring due to anterior instability have been broadly termed anteroinferior labroligamentous lesions (Figure 1).

Pictorial representation of increasing soft tissue injury. ALPSA, anterior labrum periosteal sleeve avulsion; GLAD, glenoid labrum articular rim disruption.
The most common lesion is the Bankart lesion, followed by the less common Perthes lesion, anterior labrum periosteal sleeve avulsion (ALPSA) lesion, glenoid labrum articular rim disruption lesion, bony Bankart lesion, and humeral avulsion of the glenohumeral ligament lesion. A Bankart lesion, which is a capsulolabral pathology, is a capsular disruption in addition to an avulsion of anteroinferior labrum. 39 A Perthes lesion is a nondisplaced labral avulsion with an intact periosteum. An ALPSA lesion is similar to a Perthes lesion in that the periosteal sleeve remains in continuity. However, while remaining structurally intact, the whole anterior periosteal sleeve in the ALPSA leasion is stripped of its glenoid and anterior scapular attachment and heals in a nonanatomic and nonfunctional medial position on the glenoid neck. 2
The ALPSA lesion was first described by McLaughlin 24 in 1960, but it was explained by Neviaser 27 in a case of anteroinferior glenoid instability. The ALPSA lesion has no periosteal rupture 5 from the glenoid but is displaced medially and rotated inferiorly, unlike the Bankart lesion. Reports have identified ALPSA lesions as different pathological variants of the Bankart lesion, and both can occur in those with first-time and recurrent dislocations. Although literature on the Bankart lesion is abundant, there are only a few articles on ALPSA lesions. We set out to review the size and scope of the current literature on ALPSA lesions to highlight its importance and distinguish between ALPSA and Bankart lesions in diagnostic and treatment strategies. A scoping review can be defined as the gathering of knowledge by systematic and repetitive identification of literature on a given topic.
A scoping review is a kind of literature analysis that seeks to map and give an overview of the research that has already been done on a certain issue. To pinpoint the key ideas, hypotheses, sources of support, and research gaps in a specific topic, it entails methodically looking through, picking out, and summarizing pertinent works.
Instead of assessing the merit of individual studies or synthesizing the findings, the main goal of a scoping review is to investigate the volume, breadth, and type of current literature on a certain issue. It aids researchers in comprehending the range of present research, identifying significant themes or areas of consensus, and pinpointing areas in need of more study.
Methods
The PubMed, Scopus, Embase, and Google Scholar databases were searched for the keywords “ALPSA” OR “anterior labrum periosteal sleeve avulsion” OR “anterior labral periosteal sleeve avulsion” OR “anterior labroligamentous periosteal sleeve avulsion” lesion. The inclusion criteria were as follows: PubMed, Scopus, Embase and Google scholar databases (PRISMA Chart) were searched for keyword ALPSA OR “anterior labrum periosteal sleeve avulsion” OR “anterior labral periosteal sleeve avulsion” OR “anterior labroligamentous periosteal sleeve avulsion"lesion. Articles written in a language other than English were excluded. Duplicate articles as well as those with repetitive literature were also excluded. Additionally, articles that had incomplete data or no new relevance or no literature related to ALPSA lesions were excluded. A total of 42 relevant articles were identified, and their references were reviewed for further relevant publications. Figure 2 shows a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of the studies included and excluded according to the criteria.
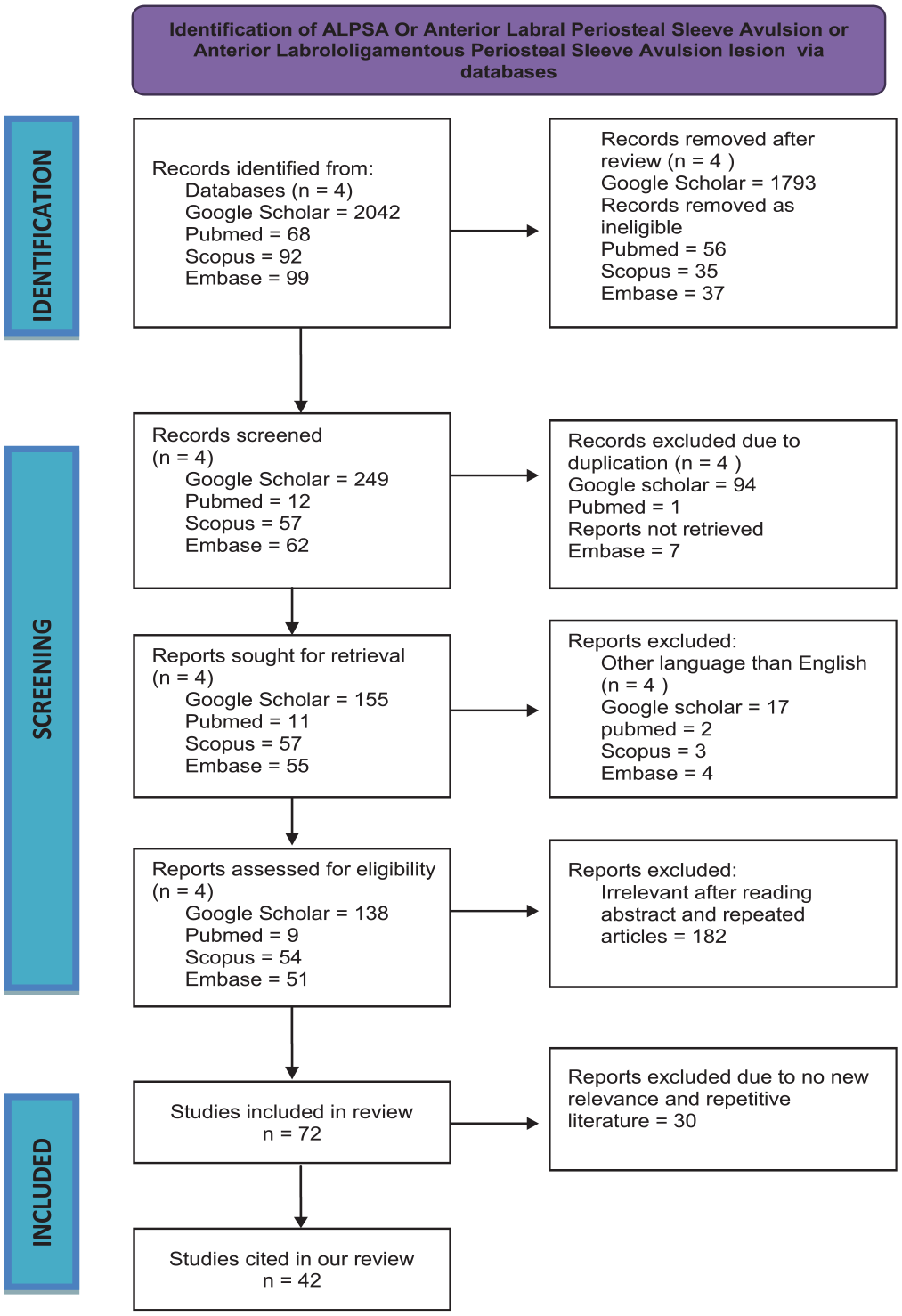
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart.
ALPSA Definition and Pathology
ALPSA lesions are more commonly found in younger patients (younger than 25 years old), and they result in more episodes of dislocation preoperatively as well as have a higher chance of recurrence after arthroscopic surgery. The cause for these lesions is unknown, but the increased rate of recurrence may be because of the lack of a “periosteal hinge” along the neck of the glenoid. In an ALPSA lesion, the periosteal hinge either is missing or has collapsed, which can increase instability and reduce available surface for healing.
Neviaser 27 reported a specific pathological condition in which the IGHL, labrum, and periosteum are displaced medial to the glenoid rim without tearing the scapular periosteum; this has been termed an “anterior labroligamentous periosteal sleeve avulsion lesion.” This nonanatomic healing of the labroligamentous complex onto the neck of the scapula interferes with the normal glenoid concavity and integrity of the IGHL and capsular complex. It is essential to correctly identify and differentiate Bankart from ALPSA lesions for proper reconstruction. Failure to differentiate them can result in imperfect restoration and stability of the glenohumeral joint.
The pathogenesis of the ALPSA lesion remains unclear, with some authors considering it as a progressive Perthes lesion occurring secondary to multiple dislocations. 15 Studies have reported that the incidence of an ALPSA lesion in first-time dislocations is in the range of 7.9% to 39% and up to 31% in recurrent shoulder dislocations. 32
Results and discussion
Our scoping review screened 42 articles with 7167 patients, 1272 of whom had an ALPSA lesion. Earlier publications (early 1990s) were of varied pathology, such as Bankart and Perthes lesions. However, the lesion gained interest in 1993 when ALPSA was explained by Neviaser. 27 With the further advent of magnetic resonance angiography (MRA) and advances in arthroscopic procedures, it was easy to identify the lesion, and more publications on ALPSA gained momentum. Levels of evidence have also increased in the last 3 years to more level 1 systematic reviews,31,40 from 9 studies with levels of evidence 4 and 5 between 2011 and 2020. Of all the articles, 5 were cadaveric studies1,7,21,37,42 spanning 45 cadavers. Two articles27,31 exclusively studied ALPSA lesions.
Our scoping review differs from other systematic reviews in that we were able to delineate ALPSA lesions from other shoulder lesions in all aspects from diagnosis until management. We accept that the level of evidence is lower than that in a systematic review. In a recent systematic review by Reiter et al, 31 only the associated injuries and postoperative outcomes of the ALPSA lesion were studied. Our scoping review details the nonanatomic healing position of labral tissue, classification types, the lesion’s easy diagnosis by MRA and anterior arthroscopic portals, the repair techniques for adequate soft tissue healing, and the postoperative physical therapy protocol for achieving good outcome and preventing recurrent dislocation.
Yiannakopoulos et al 41 found that 78% of patients with acute dislocations had Bankart lesions, while 97% with chronic dislocations had either Bankart or ALPSA lesions; all the ALSPA lesions were in the chronic group. Patients with ALPSA typically show reduced external arm rotation at 90° of abduction because of IGHL shortening from reattachment in an inferomedial position on the glenoid neck. 9
Patients with ALPSA lesions showed more than double the glenoid bone loss during arthroscopic surgery compared with those without ALPSA lesions and also had more instability events. 6 Habermeyer et al 15 found ALPSA lesions to be a time- and recurrence-dependent result of Bankart or Perthes lesions and that they did not present within 2 weeks of an initial dislocation. 36 Ozbaydar et al 29 reported a higher number of dislocations in patients with ALPSA lesions compared with those with Bankart lesions.
Lee et al 22 found that patients with ALPSA lesions had a higher likelihood of developing larger Hill-Sach defects, more glenoid erosion, and lesions extending to the 2-o’clock position compared with those with Bankart lesions. These factors make patients with ALPSA lesions more prone to recurrent dislocations, suggesting preference to primary surgical intervention.
Investigation for ALPSA
Hammond 16 highlighted cases in which ALPSA lesions with heterotopic ossification were misdiagnosed as bony Bankart lesions. Proper diagnosis is crucial to avoid incorrect surgical decisions. Surgeons should be aware of the symptoms and use computed tomography scans to distinguish between the 2 conditions.
Magnetic resonance imaging using gadolinium contrast is more sensitive and specific for identifying complex lesions like ALPSA lesions compared with other imaging methods. 26 Preoperative identification of these lesions is key to reducing postoperative recurrence. ALPSA repair has a higher failure rate (up to 12.9%) compared with Bankart repair,29,31 and MRA was more accurate than plain magnetic resonance imaging (1.5 T) for ALPSA detection. 17 Magnetic resonance imaging scans of lesions are shown in Figure 3.

Magnetic resonance imaging scans showing a (A) Bankart lesion (axial cut), (B) bony Bankart lesion (sagittal cut), (C) Perthes lesion (axial cut), (D) glenoid labrum articular rim disruption lesion (axial cut), (E) anterior labrum periosteal sleeve avulsion lesion (axial cut), and (F) humeral avulsion of the glenohumeral ligament lesion (sagittal cut). Arrows indicate the respective lesion in the images. Reprinted with permission McAdams T, Fredericson M, Vogelsong M, Gold G. New developments in magnetic resonance imaging techniques for shoulder instability in athletes. Open Access J Sports Med. 2010;1:137-142. © 2010 McAdams et al, publisher and licensee Dove Medical Press Ltd. 23
Different shoulder positions in MRA improve lesion detection; adduction and internal rotation are effective for ALPSA lesions, and abduction and external rotation are effective for Perthes lesions.35,38 Conventional MRA is generally effective for detecting ALPSA lesions, 38 and 1 study 34 found that a single series of MRA in the abduction and external rotation positions was adequate for the diagnosis of anteroinferior labroligamentous lesions. The disadvantages of MRA include its time-consuming coil positioning, patient discomfort, and dislocation risk. 34
Classification
ALPSA lesions were classified into 2 subtypes by Antonio et al 2 based on labral detachment or attachment to the glenoid neck: (1) free and (2) adherent. Both subtypes were displaced medially. The adherent type was associated with recurrent dislocations and poor outcomes, as the medialized labrum was fixed by granulation tissue and coagulated blood in a nonanatomic position. 19
Gartsman 13 divided anterior labrum tears into 3 types: in type A, the labrum is separated from the glenoid bone but remains at the level of the glenoid joint; in type B, the labrum is separated from the glenoid bone and retracted medially; and in type C, the labrum is separated from the glenoid bone, retracted, and has healed medially on the glenoid, equivalent to an ALPSA lesion (Figure 4). Gartsman also reported that surgical dissection should be performed before a repair and the labrum should be mobilized to the superolateral region in type B and C lesions. 13

Gartsman classification of types A, B, and C for anterior labral tears. Type A: the labrum is separated from the glenoid bone but remains at the level of the glenoid joint. Type B: The labrum is separated from the glenoid bone and retracted medially. Type C: The labrum is separated from the glenoid bone, retracted, and has healed medially on the glenoid, equivalent to an anterior labrum periosteal sleeve avulsion lesion.
ALPSA lesions are also classified as acute and chronic types. 25 The acute form is easy to identify with magnetic resonance imaging by the presence of a medialized labrum, but identification of the chronic form is difficult. This is because of scarring and synovial reformation of the medial labrum. Acute forms can be treated easily by suturing the labrum to its anatomic and functional position; however, chronic forms need correct identification, thorough debridement of the scarred tissue, and repair of the labrum.22,26
Surgical Management of ALPSA Lesions
Before draping, shoulder motion and glenohumeral instability are assessed. Examination under anesthesia can flag potential ALPSA lesions if there is a >5° loss of external rotation on one side. 9 A thorough visual inspection of the joint is done via a posterior portal. Poor capsular tissue quality indicates recurrent dislocations, and ALPSA lesions are identified by examining the anteroinferior labrum. Instruments are introduced through 2 anterior rotator interval portals. The clinical and arthroscopic findings are summarized in Table 1.
ALPSA Lesion Findings a
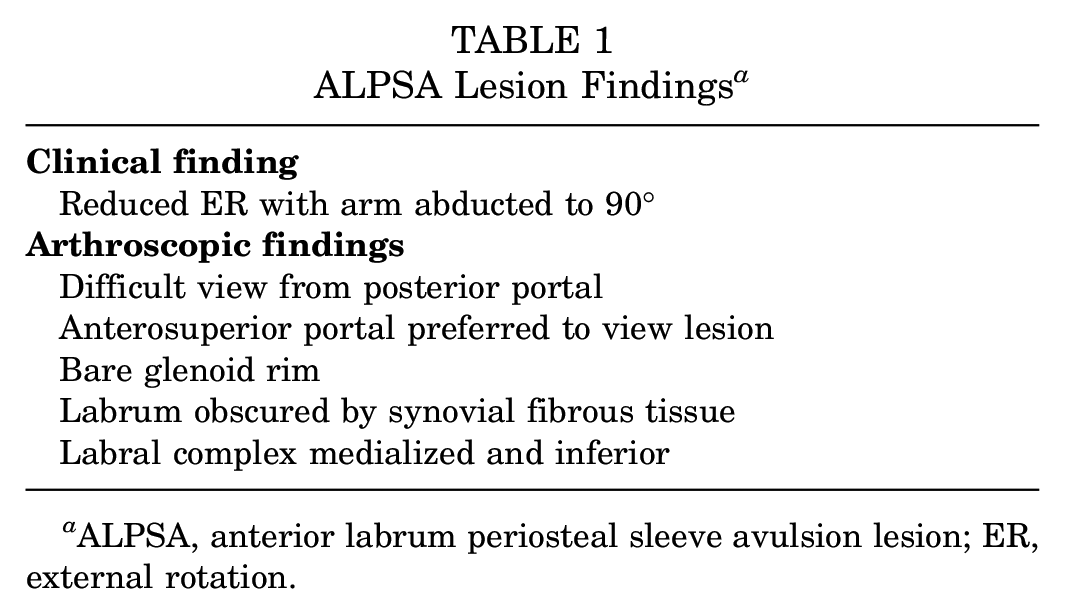
ALPSA, anterior labrum periosteal sleeve avulsion lesion; ER, external rotation.
ALPSA lesions can be more difficult to identify via arthroscopy from the normal posterior portal, but a 70° arthroscope can be useful. 28 Since the labroligamentous complex has healed medially, it cannot be viewed where the labral tissue is divided with a standard 30° scope. For a more accurate diagnosis, these lesions should be viewed from the anterosuperior portal. With use of this view, ALPSA lesions can be repaired by lifting the labroligamentous complex off the scapular neck using a curved radiofrequency wand or tissue liberator. Release is continued until the subscapularis muscle is visualized. This allows for adequate release and anatomically restoring the labral complex back onto the glenoid edge.10,12,14,33 Care must be exercised while releasing in the 4:30 to 5:30 positions as the axillary nerve is at its closest proximity and is at the greatest risk in this position.
Arthroscopic treatment of ALPSA lesions can be challenging. When the glenohumeral joint is viewed through the posterior portal, the glenoid rim may appear bare, with the labral complex out of sight behind the scapular neck. It could also be obscured by synovial fibrous tissue. Ozbaydar et al 29 found that the recurrence of instability after arthroscopic capsulolabral repair for an ALPSA lesion is twice as high as the recurrence after repair of a classic Bankart lesion.
The best results were seen in the repair that used a pleated shift of capsule by suture anchors. This procedure is successful because it bypasses degenerated labral tissue and restores the anatomic position (Figure 5).4,19,22,29 On the other hand, chronic ALPSA lesions with a decreased or collapsed periosteal hinge along the glenoid neck need to be repaired and reinforced by bony procedures, that is, Latarjet 12 or double-row anchor suture repair 1 or double-mattress suture bridge repair. A recent technique described the use of the long head of the biceps tendon to create a labral augmentation. 42 This technique is useful for patients with intact or minimally disrupted bone stock, but with poor capsulolabral tissues.

Pleated capsular shift by suture anchors.
The most applicable situation for double-row labral repair is cases of severe capsulolabral injury or ones that require full release and mobilization of the capsulolabral complex, such as in ALPSA lesions (Figure 6). Ozbaydar et al 29 recently reported a significantly higher failure rate for arthroscopic repair of ALPSA lesions compared with Bankart lesions. The ability of the double-row repair to better oppose a large amount of capsulolabral tissue could be helpful in anatomically reconstructing these ALPSA lesions, improving healing.

Double-row labral repair of capsulolabral injury.
As recurrent dislocation rates are high in ALPSA lesions despite strict adherence to postoperative physical therapy, all acute ALPSA lesions should be surgically repaired to avoid (1) scarring of tissue in the glenoid neck, (2) poor tissue quality, (3) complex surgery, and (4) poor outcomes in preference to nonoperative treatment. 28
Postoperative Rehabilitation
Postoperatively, the physical therapy protocol in many studies is to immobilize the shoulder in an abduction brace for 3 to 4 weeks.4,8,10,27 However, Dumont et al 12 advised anterior repairs to be immobilized in an abduction sling and posterior repairs in an external rotation sling, with and active- and passive-assisted motions 7 to 10 days after surgery. This was to avoid stress on posterior capsular tissues after repair.
After surgery, Gartsman 13 recommends 15° of arm abduction in a sling and initiation of light exercises for 2 weeks. Patients advance to full-range movements by 4 weeks. Other protocols, such as those of Kim et al 19 and Dumont et al, 12 introduce muscle strengthening between 6 and 12 weeks. De Campos Azevedo and Ângelo 8 start resistance exercises 3 to 6 weeks after surgery, and sports are generally permitted at 6 months, except for contact sports, which are allowed after 1 year. Our protocol is to use an arm sling for 6 weeks and gradually increase exercises, allowing a return to overhead sports between 9 and 12 months.
Failure Rates in ALPSA Management
ALPSA lesions are linked to more preoperative dislocations, larger Hill-Sachs defects, and more glenoid bone loss compared with isolated Bankart lesions.6,29 They also have a higher failure rate, with nearly twice the rate of recurrent instability after arthroscopic repair.
ALPSA lesions have a much higher rate of preoperative dislocation, synovitis, engaging Hill-Sachs lesions, and postoperative redislocations. 14 On the other hand, ALPSA lesions were present in 18% of first-time glenohumeral dislocations that were arthroscopically evaluated. 36 Antonio et al 2 concluded that MRA and arthroscopic evaluations revealed ALPSA lesions in 39% of their first-time shoulder dislocations. The ALPSA lesion occurred in 12.5% of patients, and 9 of 72 of their patients experienced 1 episode of dislocation, which implies that this lesion is also present in those with first-time dislocations and not just after repeated dislocations. According to Park et al, 30 the ALPSA group showed a greater frequency of dislocations (9.3 ± 13.5) compared with the Bankart group (3.2 ± 5.1) (P = .0091).
Recurrence rates after arthroscopic repair of ALPSA lesions ranged between 8.3% and 19.2%, 11 which corresponded with approximately double the rate of recurrences of the Bankart lesions that were operated on in the same studies. In a meta-analysis without individual patient data, only a separate analysis of risk factors such as age ≤20 years and ≤30 years was possible; a multivariate analysis was not feasible because of the lack of patient information 40 (Table 2). The articles reviewed with their characteristics and key findings are given in Supplementary Table 3 for reference.

ALPSA, anterior labrum periosteal sleeve avulsion lesion.
The high failure rate of ALPSA lesions is likely related to the difficulty in restoring the anatomic footprint of the labrum in these medialized and scarred lesions. 40 The 2 possible explanations are (1) technique-based difficulties resulting in inadequate tissue mobilization before repair and (2) poor quality and/or insufficient tissues that are inadequate for the mechanical loading encountered during rehabilitation and normal motions with use.
Park et al 30 reported in their study that ALPSA lesions, Hill-Sachs lesions, a poor labrum, and poor capsular tissue quality appeared to be closely related to labral height loss between 3 months and 1 year postoperatively.
In the ALPSA group, the mean postoperative labral heights at 3 months and 1 year were 5.4 ± 2.0 mm (range, 2.9-8.8 mm) and 4.6 ± 2.2 mm (range, 1.6-8.5 mm), respectively. There was a significant decrease in the mean labral height at 1 year postoperatively (P < .01) compared with that observed at 3 months.
In a recent study, Arner et al 3 compared the results of matched patients with 19 ALPSA lesions and 62 Bankart repairs with a minimum 2-year follow-up and found a significantly greater rate of recurrent dislocation in the ALPSA group (32%) compared with the Bankart group (10.7%). Also, although not statistically significant, 20% of patients from the ALPSA group had revision surgery compared with only 10.7% from the Bankart group. However, no difference was found in the postoperative outcome scores between the groups. The number of preoperative dislocations in this study was lower than those in an earlier study by Ozbaydar et al. 29
Some authors recommend opting for the Laterjet procedure when treating an ALPSA lesion, particularly if it is coupled with significant glenoid bone loss and poor tissue quality and in patients deemed at a higher risk of recurrence during physical activities such as sports and work. 3 Recently, there has been experimentation with labral reconstruction using the long head of the biceps tendon, and clinically favorable outcomes have been observed during the 1-year follow-up period. High-quality studies are required in the form of randomized controlled trials to establish the outcomes of ALPSA lesions compared with Bankart lesions. Currently, no high-quality studies have been published.
Limitations
Our study has some limitations. First, several studies may have included ALPSA lesions as part of their cases even though the title or abstract did not include terms picked up by our search, so these studies may have been left out. Second, the incidence of ALPSA lesions is rare compared with Bankart lesions; therefore, the number of high-quality studies is limited to just case series and cohort studies with limited numbers.
Conclusion
There is a paucity of exclusive literature on ALPSA lesions. It is important to distinguish these lesions from Bankart lesions as it is associated with worse outcomes. The greater failure rates of ALPSA lesions indicate that the current repair techniques require further refinement to improve the outcomes to the standard of Bankart lesions.
ALPSA lesions of the shoulder should be diagnosed and repaired early, before scarring and healing onto a medialized, nonfunctional glenoid neck position, to prevent recurrent dislocations and reduce repair failures. These lesions also need to be clinically followed for a longer duration to ensure good functional outcomes. Further high-quality studies are required on this topic to both understand the relationship between ALPSA lesions and associated subcritical bone loss as well as off-track lesions and improve repair techniques and outcomes.
Supplemental Material
sj-docx-1-ojs-10.1177_23259671241258198 – Supplemental material for Anterior Labrum Periosteal Sleeve Avulsion Lesions of the Shoulder: A Scoping Review
Supplemental material, sj-docx-1-ojs-10.1177_23259671241258198 for Anterior Labrum Periosteal Sleeve Avulsion Lesions of the Shoulder: A Scoping Review by Senthilvelan Rajagopalan, Mounika N.S. Chodavarapu, Srinivas B.S. Kambhampati, Shyam Kumar Chinta and Srinath Kamineni in The Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted October 5, 2023; accepted January 1, 2024.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.