
Abstract
Background:
Failure rates up to 14% have been reported after arthroscopic posterior capsulolabral repair. It is unknown if revision arthroscopic posterior capsulolabral stabilization has inferior restoration of stability and return to sport when compared with primary repair. Optimal management of failed posterior capsulolabral stabilization is unknown.
Purpose:
To report outcomes of revision posterior capsulolabral repair and factors that contribute to failure and to determine optimal management of failed posterior stabilization procedures.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A computerized search of the PubMed, EMBASE, and Web of Science databases and manual screening of selected article reference lists were performed in January 2022. Randomized controlled trial, cohort, case-control, and case series studies reporting clinical outcomes of revision arthroscopic posterior capsulolabral repair were eligible. Patient characteristics, indications for revision, intraoperative findings, surgical techniques, and patient-reported outcomes were recorded. Owing to heterogeneity of reported outcomes, data were summarized and presented without pooled statistics.
Results:
Only 3 of the 990 identified studies met inclusion criteria. The included studies encompassed 26 revision arthroscopic posterior capsulolabral repairs, with follow-up ranging from 2.3 to 5.3 years. The failed index procedure was arthroscopic capsulolabral repair with suture anchors (n = 22) or posterior thermal capsulorrhaphy (n = 4). The primary indications for revision were recurrent instability and pain. Six patients experienced recurrent instability after revision. Patient satisfaction ranged from 15% to 25%.
Conclusion:
This systematic review of 3 studies demonstrated that the incidence of persistent pain and recurrent instability after revision arthroscopic posterior shoulder stabilization is common, and despite slight improvement in patient-reported outcomes, many patients are dissatisfied with their clinical outcomes. Revision arthroscopic posterior shoulder stabilization appears to have a significant failure rate, and there is need for additional prospective studies to help determine the best intervention for these patients.
Historically, posterior shoulder instability was thought to be a relatively uncommon condition, occurring in about 10% of patients with shoulder instability. 27 However, posterior shoulder instability is an increasingly recognized and surgically treated pattern of instability in young active patients. Recent series have shown that isolated posterior labral tears make up 20% to 24% of all operative shoulder stabilization procedures. 33,34,39 While nonoperative treatment traditionally has been preferred, numerous studies over the past 25 years have demonstrated good to excellent outcomes for most patients with operatively treated posterior shoulder instability. 10,30
Despite mostly favorable results, previous studies of arthroscopic repair demonstrated failure rates of 0% to 14% for posterior stabilization procedures. 14 Optimal management of failed posterior labral repair and capsulorrhaphy is currently unknown. Few authors have reported outcomes of revision surgery to address failed primary repair, with mostly acceptable outcomes but with inferior restoration of stability and return to sport as compared with outcomes of primary repair. 8,35 However, these studies consist of mostly small patient cohorts and lack sufficient size for impactful clinical analysis.
Additionally, defining failure in primary and revision posterior shoulder stabilization surgery remains a challenge. Most studies define failure as poor patient-reported outcome scores or inability to return to play. 14 Unfortunately, outcome scores may not directly correlate with clinical failure. In a recent study by Bradley et al, 8 only 4 of 10 athletes who required revision arthroscopic surgery had pre-revision American Shoulder and Elbow Surgeons (ASES) or stability scores that were consistent with clinical failure. Additionally, 1 meta-analysis found that 12% of patients with operative posterior shoulder instability experienced persistent pain postoperatively. 14 Several authors have examined potential contributing factors for failure of primary posterior labral repair and capsulorrhaphy. Previous literature has demonstrated that female sex, dominant shoulder, and associated injuries were all risk factors for failed posterior capsulolabral repair. 8,35 Anatomic factors considered in recurrent instability include bony glenoid defects, glenoid retroversion, and inferior shoulder hyperlaxity. 5,37 Additionally, utilization of <3 suture anchors has been shown to be associated with recurrent instability. 5,8
To date, several studies have reported on failure of primary posterior labral repair and capsulorrhaphy and outcomes of revision posterior instability procedures. However, given the relatively small cohort sizes, there remains a lack of clarity in 3 areas: (1) clinical outcomes of revision arthroscopic posterior labral repair and capsulorrhaphy, (2) optimal definition of clinical failure, and (3) possible contributing factors to failure of primary surgery. Therefore, the primary purpose of this systematic review is to report outcomes of revision arthroscopic posterior labral repair and capsulorrhaphy. The secondary goals of this systematic review are to assess how the literature defines the failure of arthroscopic posterior stabilization procedures, particularly evaluating reasons for revision, including recurrent instability and/or persistent instability.
Methods
Study Eligibility
The design and reporting of this systematic review are in accordance with the PRISMA guidelines (Preferred Reporting Items for Systematic Reviews and Meta-analyses). 28 To ensure a comprehensive analysis, all randomized controlled trial, cohort, case-control, and case series studies examining clinical outcomes after arthroscopic revision posterior capsulolabral repair were considered for eligibility. Those investigating skeletally mature patients undergoing revision arthroscopic posterior capsulolabral repair with a minimum follow-up of 12 months were included in this review. Exclusion criteria consisted of (1) studies not available in English; (2) studies investigating anterior shoulder instability; and (3) studies examining posterior shoulder instability procedures based on open revision posterior capsulolabral repair, open and/or arthroscopic-assisted bone block, or bone augmentation. Studies were also excluded when patients undergoing revision arthroscopic posterior capsulolabral repair were included in the overall cohort but their data were not separately reported.
Literature Search
A comprehensive literature search was performed by an institution librarian in January 2022 via a computer-based search within the Medline/PubMed, EMBASE, and Web of Science databases. The following terms were used as keywords and Medical Subject Headings and appeared in the title, abstract, or keyword fields: (posterior) AND (shoulder OR glenoid OR glenohumeral OR labrum) AND (instability OR laxity OR joint subluxation OR joint dislocation) AND (reoperation OR surgical revision OR revision surgery OR repeat surgery). Further manual screening of selected articles’ reference lists was performed by 2 authors (C.A.J. & P.R.) to ascertain any relevant articles not found by the computerized search.
Study Selection and Data Extraction
After excluding duplicate articles, 2 reviewers (C.A.J., P.R.) independently screened articles identified in the literature search on the basis of title and abstract using a web app for systematic reviews (Rayyan). 25 Any disagreements between the reviewers were resolved by the senior author (L.L.). Potentially eligible articles underwent full-text review before final determination of study inclusion. Data were collected according to recommendations from the Cochrane Handbook for Systematic Reviews for data extraction, using a custom form including information on study design, patient demographics, prior surgical procedure, revision surgical procedure, and outcomes. 21
Risk-of-Bias and Quality Assessment
In the absence of randomized trials identified by the literature search and a high proportion of case series, all studies were critically appraised for risk of bias and quality of evidence. The case-control study was assessed for risk of bias using the Newcastle-Ottawa Scale: an assessment tool that assigns a maximum of 9 points for the least risk of bias in 3 domains—selection of study groups, comparability of groups, and ascertainment of exposure. 36 The case series were assessed using a tool proposed by Murad et al 24 that modifies the Newcastle-Ottawa Scale and causality criteria for case series. Quality of evidence was assessed using the MINORS tool (Methodologic Index for Non-randomized Studies) 32 : a 12-item assessment of methodologic value, with 8 criteria indicated for noncomparative and comparative studies and 4 criteria specific for comparative studies. The ideal score is 24 for comparative studies and 16 for noncomparative studies. 32
Data Analysis
Primary outcomes of interest were (1) recurrent instability defined as recurrent dislocation, subluxation, or subjective instability at final follow-up; (2) persistent pain; and/or (3) need for additional revision surgery. Other outcome measures of interest were recorded: subjective satisfaction, postoperative range of motion, postoperative ASES scores, and return to sport. Unfortunately, there was heterogeneity among the studies regarding outcome measures; as such, a meta-analysis was not conducted, and data are presented without pooled statistics, such as weighted mean or weighted effect.
Results
The literature query yielded 990 articles. After removal of duplicates, 636 articles were screened for eligibility based on title and abstract. Twelve were extracted for full-text review. Sixteen additional articles were identified by cross-referencing the selected articles’ reference list. The full text of 28 publications was reviewed for possible inclusion. After full-text review, 3 articles were included for narrative analysis (Figure 1): 1 case-control study (level of evidence 3) and 2 case series (level of evidence 4). There were no level 1 or 2 studies. When critically appraised, the MINORS score ranged from 6 to 21.

PRISMA flowchart of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
A total of 26 patients were included in this systematic review, with follow-up ranging from 2.3 to 5.3 years. The majority of patients were male (n = 17) and had a traumatic cause for their recurrent posterior shoulder instability (n = 20). The failed index procedure was arthroscopic capsulolabral repair with suture anchors (n = 22) or posterior thermal capsulorrhaphy (n = 4). Individual study and patient characteristics are summarized in Table 1.
Study Design and Patient Characteristics a

a MINORS, Methodological Index for Non-randomized Studies; NR, not reported.
The mean time from initial stabilization procedure to revision ranged from 1 to 3.2 years. The indication for revision posterior capsulolabral repair in the majority of patients was recurrent instability; however, 1 patient’s primary indication was persistent pain during sport. All patients underwent arthroscopic revision surgery. Twenty-five patients underwent a combined capsulolabral repair. A range of 3 to 6 suture anchors was used for the repairs. One patient underwent a capsular plication with suture alone (Table 2). Intraoperative findings were reported for 5 patients: 2 with posterior bone loss, 1 with failure of labral healing and posterior capsular thinning, 1 with healed posterior labrum but patulous posterior capsule, and 1 with persistent capsulolabral separation.
Indications for and Types of Revision Surgery Performed a
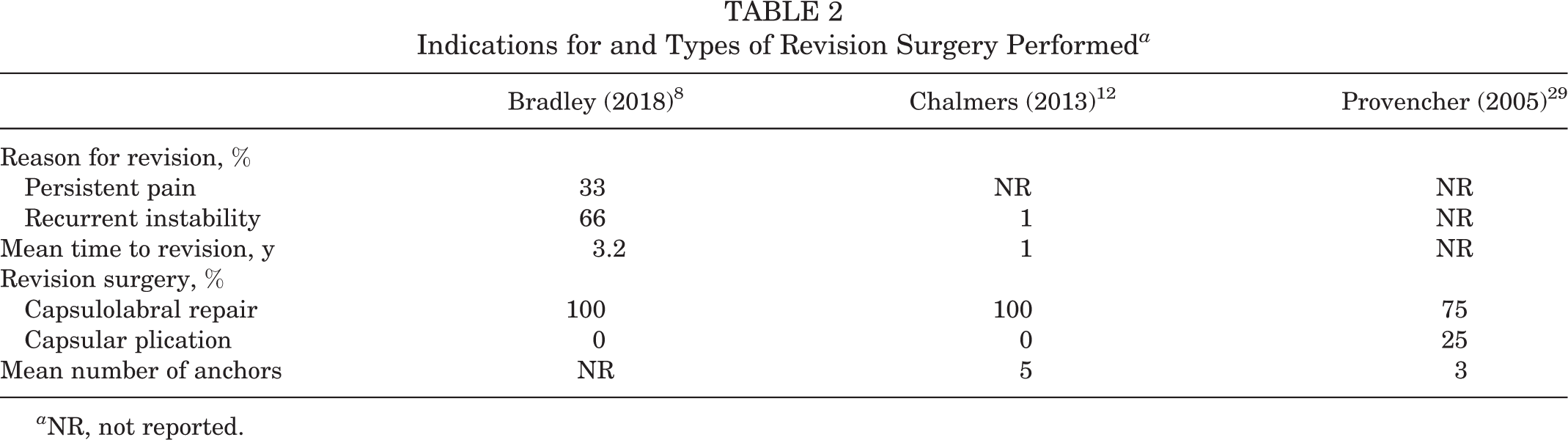
a NR, not reported.
In the majority of patients, revision surgery failed because of pain and/or instability. In the Bradley et al 8 cohort, 21% (4/19) of the revision procedures failed on the basis of the authors’ criteria (3 patients with persistent instability, 1 patient according to ASES scoring). Yet, in the Provencher et al 29 case series, revision surgery failed for 75% (3/4) of patients according to the authors’ criteria (1 patient with persistent instability, 2 patients with persistent pain). The Chalmers et al 12 case series did not define failure or failure rate.
Despite the heterogeneity among the outcome measures, all 3 studies reported postoperative ASES scores, which ranged from 67 to 84. Preoperative ASES scores were in 2 studies, ranging from 38 to 74; the improvement in ASES scores ranged from 9 to 29 points. Persistent pain after revision was not insignificant; mean postoperative pain (visual analog scale) in the Bradley et al 8 cohort was 4.2 on a scale of 10. In the Provencher et al 29 case series, 50% of patients had persistent pain after revision; conversely, no patients had persistent pain in the Chalmers et al case series. 12 Recurrent instability after revision was noted in 6 patients across all 3 series. Only 38% of patients in the Bradley et al cohort regained full range of motion after arthroscopic revision. Just 1 patient required an additional procedure after revision and underwent arthroscopic glenohumeral debridement, capsular release, and biceps tenodesis owing to loss of range of motion and biceps pain 4 years after revision posterior stabilization. Of note, despite a failure rate of 21%, only 15% of patients in the Bradley et al cohort thought that surgery was worthwhile. The outcome measures in each article are summarized in Table 3.
Outcomes of Revision Arthroscopic Posterior Capsulolabral Repair a

a ASES, American Shoulder and Elbow Surgeons; NR, not reported.
b Reported as mean visual analog scale score.
Discussion
The current study suggests that persistent pain and recurrent instability after revision arthroscopic posterior shoulder stabilization are common and many patients are dissatisfied with their clinical outcomes. Shoulder instability is a common cause of shoulder pain and dysfunction among young active individuals, particularly recurrent pain and instability after operative stabilization. Despite a recent significant increase in outcomes of arthroscopic posterior labral repairs, a known failure rate of 0% to 18%, and suboptimal outcomes of open revision posterior surgery, there is a paucity of literature objectively documenting outcomes of arthroscopically treated recurrent posterior instability even though numerous studies include patients undergoing revision in their arthroscopic cohort.
Historically, posterior shoulder instability was thought to be a relatively uncommon injury with an incidence of 2% to 10% of all operative shoulder instability cases. 6,27 However, several recent publications suggest that the incidence of operative posterior shoulder instability is higher (20%-24%) than previously published, particularly in contact and throwing athletes and the military population. 20,26,33,34,39 Song et al 33 showed that preoperative magnetic resonance imaging reports correlated with arthroscopic findings in 38 of the 55 patients (69.1%) with isolated posterior shoulder instability, as compared with correlation in 78.5% patients with anterior shoulder instability. As such, these injuries may be more difficult to detect with standard imaging studies.
Reported outcomes after arthroscopic posterior shoulder stabilization have not been consistent. In a systematic review, DeLong et al 14 cited an overall subjective patient satisfaction rate of 93.8% despite a reoperation rate of 7.6%. Unfortunately, the definition of failure is inconsistent among the posterior shoulder instability literature. In a 2006 prospective cohort study by Bradley et al 9 of patients undergoing primary posterior shoulder capsulolabral repair, 9% of cases failed on the basis of the ASES scoring system (<60) and 11% failed per a stability scale. Similarly, Provencher et al 29 found that 12% of procedures failed on the basis of recurrent instability and an additional 9% failed because of persistent pain. More recent long-term outcomes from the United States Naval Academy suggest that the failure rate of posterior repairs approaches 18% with mid- and long-term follow-up. 4
Despite evidence suggesting a nearly 1-in-5 failure rate of primary posterior shoulder stabilization, only a few series have focused on revision posterior shoulder stabilization. Some surgeons addressed these complex cases with open posterior capsular plications or bone block procedures. The outcomes of open posterior capsular plication have been modest, with instability recurring at a rate of 23%. 16 Similarly, posterior bone block procedures are technically challenging with poor long-term outcomes. Meuffels et al 23 demonstrated that over half of patients undergoing posterior bone block procedures were not satisfied and had experienced recurrent instability at 18-year follow-up.
In recent years, there has been a shift to arthroscopic revision procedures, although few studies have specifically examined the outcomes of these procedures. While outcomes of revision arthroscopic labral repair and capsulorrhaphy have been the subject of much study, with numerous published results, 1,3,15,18,19,31,38 the outcomes of revision arthroscopic posterior instability surgery are largely unknown. In the current data set, the failure rate of arthroscopic revision posterior shoulder stabilization ranged from 21% to 75%, although only 1 of 26 patients underwent an additional surgical procedure. Similar to rates of recurrent instability after open plication, 16 6 (23%) of the 26 patients experienced recurrent instability. Persistent pain occurred at a rate of 0% to 50%. Additionally, subjective patient satisfaction, based on whether the surgery was worthwhile, was low, ranging from 15% to 25%. Failure is difficult to define; however, we suggest that clinical failure be considered when patients experience persistent functional pain and/or recurrent instability.
Given the poor outcomes of revision arthroscopic posterior capsulolabral repair and the recurrent posterior shoulder instability and pain after arthroscopic posterior capsulolabral repair, this clinical entity poses a difficult problem for surgeons. This may be a career-ending injury for throwing and contact athletes, with a 68% rate of return to sport at the preinjury level. 17 In counseling patients before the index procedure, it is important to identify risk factors for failure. Some series have identified female sex, glenoid bone width ≤26 mm, and <3 anchors as potential risk factors for the need for revision arthroscopic posterior labral stabilization. 7,8,35 Additionally, preoperative symptoms may provide insight into operative outcomes. In a cohort study of active duty military personnel with operative posterior instability, patients presenting with pain or combined pain and instability were more likely to experience clinical failure as compared with patients presenting with instability alone. 13 In the Chalmers et al 12 and Provencher et al 30 case series, a subset of patients had a patulous posterior capsule at the time of revision. This is consistent with previous reporting by Bradley et al, 9 which demonstrated capsular laxity in 8 patients who required a revision index procedure. This suggests that a combined capsulolabral repair as opposed to an isolated labral repair may be indicated in patients with risk factors for recurrence. However, we recognize that this is a very subjective finding and is difficult to quantify.
The current study identifies the need for additional prospective series on the outcomes of revision posterior shoulder stabilization. Several series on posterior instability have included previously operated shoulders within their cohorts. 2,9,11,22 These texts were reviewed, but few featured sufficient outcome data on the revision procedures to draw conclusions on outcomes (Table 4).
Publications With Revisions in Their Cohorts

Through a comprehensive literature review, the current study identified a small cohort of 26 patients with sufficient outcome data regarding arthroscopic revision. As mentioned, recent literature suggests that failure of primary posterior shoulder stabilization occurs more frequently than previously believed. Thus, there is likely a higher proportion of patients undergoing revision posterior shoulder stabilization than what is accurately represented in this cohort and the current literature. More knowledge about the outcomes of these revision procedures is important for physician decision making and counseling patients before the index and revision procedures.
Limitations
The current study has several important limitations. First, the current review included 3 articles accounting for a total of 26 patients, the majority of whom were from a single study. Moreover, the publications in the analysis were level 3 or 4 evidence. Two studies were case series and noncomparative by nature. Additionally, 4 of the 26 patients underwent thermal capsulorrhaphy as their index procedure, making it difficult to compare outcomes of arthroscopic revision after the index capsulolabral repair. Finally, there was heterogeneity among the outcomes, and we were unable to calculate pooled analysis. Thus, conclusions are drawn solely by narrative data.
Conclusion
This systematic review of 3 studies demonstrated that the incidence of persistent pain and recurrent instability after revision arthroscopic posterior shoulder stabilization is common, and despite slight improvement in patient-reported outcomes, many patients are dissatisfied with their clinical outcomes. Revision arthroscopic posterior shoulder stabilization appears to have a significant failure rate, and there is need for additional prospective studies to help determine the best intervention for these patients.
Footnotes
Acknowledgment
The authors acknowledge Rachel Walden, MLIS, Eskind Biomechanical Library, and Rogelio Coronado, PT, PhD, research assistant professor, Department of Orthopaedic Surgery, Vanderbilt University Medical Center.
Final revision submitted February 11, 2023; accepted February 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.B. has received grant support from DJO, education payments from Arthrex and Smith & Nephew, and hospitality payments from Stryker. R.W.W. has received royalties from Responsive Arthroscopy. J.D. has received education payments from Supreme Orthopedic Systems and nonconsulting fees from Arthrex. L.L. has received grant support from DJO and education payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.