
Abstract
Background:
The Quality of Patient-Surgeon Relationship (QPASREL) is an 11-item questionnaire developed and validated to assess the relationship between practitioners and patients on recovery and return to work after surgery.
Purpose:
To evaluate the association of patient-surgeon relationship (PSR) and patient-physical therapist relationship (PPR), as measured by QPASREL, with a patient's return to sports (RTS) after anterior cruciate ligament reconstruction (ACLR).
Study Design:
Case-control study; Level of evidence, 3.
Methods:
This study targeted patients who underwent primary ACLR at a specialized sports surgery referral center between January and May 2021. Patients who had revision surgery, multiligamentous knee injury, and sedentary status were excluded from the study. Patients were grouped based on ability to RTS at the preinjury level 1 year postoperatively (RTS group and no-RTS group). The primary outcome was rate of RTS at 1 year postoperatively, and the primary dependent variables were the quality of PSR and PPR as measured by QPASREL scores at 6-month intervals. Secondary outcomes were the correlation and discriminative capacity of the QPASREL compared with the Anterior Cruciate Ligament–Return to Sport After Injury (ACL-RSI) scores (collected at 6-month intervals).
Results:
The study included 243 patients. Patients in the RTS group exhibited a higher mean PPR QPASREL score (36.6 ± 5.1) compared with no-RTS patients (34.8 ± 5.2; P = .01) as well as a higher mean PSR score (35.7 ± 5.1) compared with no-RTS patients (33.8 ± 5.9; P = .01). Multivariate analysis showed that every 5-point increase in the QPASREL scores for PPR and PSR resulted in a 39% (odds ratio [OR] = 1.39; P = 0.014) and 35% (OR = 1.35, P = 0.021) increased odds of RTS, respectively. A weak yet positive correlation was found between QPASREL and ACL-RSI. The predictive capacity of the QPASREL (area under the curve [AUC] = 0.60 for PPR and 0.61 for PSR), although significant, was less powerful compared with that of the ACL-RSI (AUC = 0.73).
Conclusion:
The quality of the PPR and PSR, as measured by QPASREL scores, demonstrated a significant association with RTS rates at 1 year after ACLR. A weak yet positive correlation was found between QPASREL and ACL-RSI.
Keywords
The assessment of return to sports (RTS) after anterior cruciate ligament reconstruction (ACLR) involves multiple aspects, including knee laxity, functional knee status, and psychological readiness of the patient.8,14,18,22 Laxity can be evaluated through physical examination, various arthrometer devices, and radiological stress tests. 13 Functional status of the knee can be assessed using functional scores, isokinetic testing, and neuromuscular coordination testing.1,9,11,18,19 Psychological factors have been acknowledged as having significant impact on RTS, and this dimension has been assessed by the Anterior Cruciate Ligament–Return to Sport After Injury (ACL-RSI) instrument, a validated subjective measure.2,21,27 Despite the numerous tests and subjective outcome measures used to evaluate RTS after ACLR, none of them consider the influence of the patient-surgeon relationship (PSR) or the patient-physical therapist relationship (PPR).
Recent studies have established the potential impact of the PSR and PPR on functional outcomes, particularly regarding musculoskeletal disorders. 10 The Quality of Patient-Surgeon Relationship (QPASREL) instrument is a questionnaire developed in 2017 by Dubert et al 6 to assess the impact of the PSR on recovery and return to work after surgery. The QPASREL comprises 11 items, each rated from 1 to 4, resulting in a global score that can range from 11 to 44, and it covers aspects including a surgeon's communication, availability, understanding, empathy, and encouragement to discuss concerns. This questionnaire has been shown to have good psychometric properties, including reliability and validity. 6 In 2019, Dubert et al 7 demonstrated that a positive PSR as measured by the QPASREL was associated with shortened sick leave after surgery for upper limb injuries or musculoskeletal disorders. This can result in reduced time off from work and reduced lost productivity for both patients and payers. The authors concluded that the positive impact of a good PSR on surgical outcomes may not be limited to upper limb surgery but can extend to other types of surgeries. 7 Studying the influence of PSR and PPR on RTS after ACLR is a dimension of the cluster that has not been tested before. These relationships have been found to intervene with factors affecting psychological readiness to RTS, such as kinesiophobia and ACL-RSI. 17
The aims of the current study were to (1) evaluate the association between the patient-practitioner relationship (PSR and PPR), as measured by the QPASREL, and the rate of RTS at the same preinjury level at 12 months after ACLR and (2) compare these findings with the ACL-RSI through correlation and discriminative capacity analysis. The hypotheses being tested were that (1) a positive PSR and PPR as evaluated through the QPASREL would be associated with a higher rate of RTS at the same preinjury level after ACLR and (2) a positive PPR as measured by the QPASREL would be more highly correlated with the ACL-RSI score than would PSR.
Methods
Study Design
This prospective study formed part of the French prospective ACLR cohort study (FAST; ClinicalTrials.gov identifier NCT02511158) and was conducted at a specialized sports surgery referral center. The study protocol was approved by the research ethics committee of the center, and all included patients provided consent to participate. The study targeted patients who underwent primary ACLR between January and May 2021 at a single institution. Exclusion criteria were revision surgery, multiligamentous knee injury, patients who did not participate in any sports, and those who refused to participate in the study.
Study Population
During the study time frame, 360 patients underwent ACLR. Of these patients, 77 patients did not meet the eligibility criteria (28 patients who had revision surgery, 12 patients who had multiligamentous injury, 14 sedentary patients, and 23 patients who refused to participate). Of the remaining 283 patients, 40 were lost to follow-up. Consequently, the final study sample comprised 243 patients.
Surgical Intervention and Postoperative Rehabilitation
Six senior orthopaedic surgeons specializing in sports surgery operated on patients in this study, with different ACLR techniques, mainly hamstring grafts (quadrupled semitendinosus, doubled gracilis and doubled semitendinosus, Biofast technique 12 ) and the modified Macintosh procedure. 5
For all patients, the surgeon follow-up was scheduled 4 times: at 45 days, 3 months, 6 months, and 9 months postoperatively. Standard physical therapy was conducted 3 times a week. For competitive or professional athletes, the frequency of physical therapy was increased to 5 times a week.
All patients followed a uniform postoperative rehabilitation protocol, which involved wearing a hinged brace in full passive extension for several days. Total weightbearing was allowed. The rehabilitation program started a few days after surgery, and physical therapists were given a certain margin of autonomy. The program involved progressive range of motion exercises with a focus on hamstring strengthening and quadriceps activation. Patients with repaired meniscal injury had motion restricted between 0° and 90° for the initial 6 weeks, accommodating the meniscal repair. Adherence to the physical therapy protocol was confirmed on a binary basis (“yes” for adherence, “no” for nonadherence) when the information was gathered during patient follow-up.
Collected Data and Timeline
A timeline of data collection procedures is shown in Figure 1. We prospectively collected demographic data, type of sport, and preoperative information such as the Tegner activity level 23 using the internet-based software WebSurvey. At 6 months postoperatively, each included patient was asked to complete the validated French version of the ACL-RSI2,21 as well as an online version of the QPASREL with its original form for PSR and a modified form for PPR. In the modified form, the word surgeon was replaced with physical therapist in the 11-item questionnaire. Patients who expressed uncertainty about any item received a clarifying explanation from a researcher via telephone.

Timeline of patient recruitment and data collection for the study. ACL-RSI, Anterior Cruciate Ligament–Return to Sport After Injury; QPASREL, Quality of Patient-Surgeon Relationship; RTS, return to sports.
Time to RTS was stratified based on the activity type: 4 months for nonpivoting sports, 6 months for pivoting noncontact sports, and 8 to 9 months for pivoting contact sports. Athletes were cleared for RTS upon achieving <10% deficit in quadriceps and hamstring strength; dynamic valgus control; and deficits <10% in single-hop, triple-hop, and triple crossover tests, with values normalized to the limb symmetry index. Normalization of the quadriceps to hamstring ratio was also required.
At 12 months postoperatively, patients were asked to fill out an online questionnaire, which included questions about their ability to return to their preinjury level. The RTS questionnaire contained the following items and response options:
Have you resumed running? yes/no (if yes, resumption date).
Have you resumed pivot sports training? yes/no (if yes, resumption date).
Have you resumed pivot sports competition? yes/no (if yes, resumption date).
Have you resumed the sport you used to practice regularly before your injury? yes/no (if yes, resumption date).
Your current sports level is superior/identical/inferior/changed sports/stopped sports.
If you have changed sports, is it due to your knee (pain, apprehension, instability)/personal reasons/professional reasons?
If you have stopped sports, is it due to your knee (pain, apprehension, instability)/personal reasons/professional reasons?
Outcome Measures
The primary outcome measure was the rate of RTS at the preinjury level at 12 months postoperatively. The primary dependent variables were the quality of PSR and PPR as measured by QPASREL scores. The secondary outcome measure was the correlation between the QPASREL and ACL-RSI.
Patients were divided into 2 groups: those who returned to the same preinjury level (RTS group) and those who did not (no-RTS group). The RTS group included respondents who both returned to the same preinjury sport or activity level and perceived their postinjury performance as equivalent to their preinjury level. Conversely, the no-RTS group included respondents who did not return to the same preinjury sport or activity level did not perceive a decline in their postinjury performance and did not transition to a different sport due to the injury.
For each group, we assessed the QPASREL scores for surgeon (for PSR) and physical therapist (for PPR).
Statistical Analysis
Categorical variables were described using percentages, whereas continuous variables were described by means and standard deviations. Comparisons between the RTS and no-RTS groups were performed with the Fisher exact test or chi-square test for categorical data and the t test or Mann-Whitney test for continuous variables, as appropriate.
Multivariate regression analyses were performed to determine whether physical therapist and surgeon QPASREL scores were predictors of RTS at 1 year postoperatively. PPR QPASREL score and PSR QPASREL score were evaluated as continuous variables (with an increase every 5 points) and as categorical variables. For categorical variables, the QPASREL scores were divided into quartile categories using 2 methods: (1) as defined by Dubert et al 7 : low (11-28), medium-low (29-32), medium-high (33-38), and high (39-44), and (2) as defined by our own data quartiles. This dual-category analysis was undertaken to mitigate potential quartile limitations like outlier sensitivity and information loss while harmonizing our results with established norms of the QPASREL score. 7 Our analysis focused on examining the relationships between PSR/PPR and RTS, separately in different regression models, and all regression models were adjusted for sex, age, body mass index (BMI), and the level of sport.
Due to the multiple comparisons, the Benjamini-Hochberg statistical correction was applied to the P values (Padj), ensuring a controlled threshold of statistical significance.
The Spearman correlation coefficient was used to assess the association between the QPASREL and the ACL-RSI scores. To compare the capacity of the QPASREL and the ACL-RSI in determining readiness to RTS at 1 year, receiver operating characteristic curves were plotted.
For all analyses, P < .05 was considered statistically significant. All statistical analyses were carried out using the R statistical software (Version 4.2, Vienna, Austria).
Results
Patient Characteristics
Patients had a mean age of 31.4 ± 10.8 years, the sample included 46.5% women and 53.5% men, and no significant age- or sex-based differences were found between the RTS group (n = 130) and the no-RTS group (n = 113) (Table 1). Mean BMI was 23.7, and knee injuries were slightly more frequent on the right side (56.8%). A significant difference was observed in the level of sport engagement, with the RTS group containing more competitive or professional athletes (P < .01). Participants predominantly played pivot contact sports (56.0%), but the type of sport did not significantly affect RTS rates. The mean preoperative Tegner activity score was 6.9, with no significant difference between RTS groups. The rate of RTS to the same preinjury level was 53.4% (130 patients).
Descriptive Data of the Study Population a

Data are reported as mean ± SD or n (%) unless otherwise indicated. BPTB, bone–patellar tendon–bone; IQR, interquartile range; LET, lateral extra-articular tenodesis; RTS, return to sports.
Examples include soccer, handball, rugby, basketball, and judo.
Examples include tennis, skiing, badminton, and volleyball.
Examples include jogging, bicycling, and swimming.
Comparison of QPASREL Scores and Categories Between Groups
Patient-Surgeon Relationship
The RTS group had a higher mean PSR QPASREL score (35.7 ± 5.1) than the no-RTS group (33.8 ± 5.9; P = .01, Padj = .027). When scores were categorized according to the Dubert et al 7 categories, no significant difference was observed (P = .11, Padj = .113). However, significance emerged when the scores were segmented using our data quartile categories (P = .03, Padj = .039) with the RTS group being more likely to have high quality of PSR (>38; 32.3% vs 21.2%, respectively). Conversely, 55.8% of patients in the no-RTS group fell into the lower 2 quartiles, specifically those classified as low (<31) and medium-low (31-34), compared with only 39.3% in the RTS group (Table 2 and Figure 2).
Comparison of Physical Therapist and Surgeon QPASREL Scores Between Groups a

Data are reported as mean ± SD or n (%). Boldface Padj values indicate statistically significant difference between groups (P < .05). PPR, patient-physical therapist relationship; PSR, patient-surgeon relationship; QPASREL, Quality of Patient-Surgeon Relationship; RTS, return to sports.
Adjusted P value with Benjamini-Hochberg correction.

Comparison of RTS rate according to differing categories of the QPASREL score for the (A) patient-surgeon relationship and (B) patient–physical therapist relationship. Top row: Dubert et al 7 categories; bottom row: categories according to data quartiles. QPASREL, Quality of Patient-Surgeon Relationship; RTS, return-to-sports.
Notably, higher scores for item 1 (ease of obtaining sick leave certificates from the surgeon), item 2 (easy and clear language), item 5 (guidance on returning to work from the surgeon), item 8 (discussion of return-to-work conditions), and item 9 (empathy and understanding by the surgeon of the impact of pain and disability on mood) were particularly associated with a successful RTS (Appendix Tables A1 and A2).
Patients in the RTS group exhibited a higher mean PPR QPASREL score (36.6 ± 5.1) compared with patients in the no-RTS group (34.8 ± 5.2; P = .01, Padj = .025). Patients who had high-quality PPR had increased odds to be in the RTS group (43.1% for Dubert et al 7 categories; 34.6% for data quartile categories) than those in in the no-RTS group (28.3% and 22.1%, respectively) (Table 2). An increasing trend of RTS rates was observed when scores passed from low to high PPR quality (Figure 2).
Notably, higher scores on the PPR QPASREL for item 1 (ease of obtaining recommendations for sick leave certificates from the physical therapist), item 4 (satisfaction with the availability of the physical therapist), item 8 (physical therapist discussing return-to-work conditions), and item 11 (physical therapist encouraging discussions about concerns and listening carefully) were closely linked to a successful RTS. Scores for all items on the PSR and PPR QPASREL are provided in Appendix Tables A1 and A2.
Results of Multivariate Analysis
Table 3 shows the results of the multivariate analysis after we controlled for factors such as sex, age, BMI, and the level of sport and accounted for PSR and PPR (and vice versa). For the continuous scores, every 5-point increase in the PSR QPASREL score corresponded to a 35% increased odds of RTS at 1 year (OR = 1.35; 95% CI, 1.05-1.76; P = .021, Padj = .045). Similarly, for every 5-point increase in the PPR QPASREL score, there was a 39% increased odds of RTS at 1 year (OR = 1.39; 95% CI, 1.07-1.83; P = .014, Padj = .037).
Multivariate Analyses of Return-to-Sports Rates Based on QPASREL Scores a

Boldface Padj values indicate statistical significance (P < .05). PPR, patient-physical therapist relationship; PSR, patient-surgeon relationship; QPASREL, Quality of Patient-Surgeon Relationship.
Adjusted P value with Benjamini-Hochberg correction.
Based on the data quartile categories, patients with a low (>38) PSR QPASREL score had 2.89 times more odds to RTS at 1 year than those with a high (<31) score (OR = 2.89; 95% CI, 1.32-6.49; P = .009, Padj = .043). When we classified the QPASREL scores by Dubert et al 7 categories, no significant difference was observed on either PSR or PPR QPASREL scores.
QPASREL Versus ACL-RSI Scores at 6-Month Follow-up
Receiver operating characteristic curve analyses revealed no significant difference between the area under the curve (AUC) values for PSR QPASREL and PPR QPASREL (0.61 [95% CI, 0.54-0.68] vs 0.60 [95% CI, 0.53-0.67], respectively; P = .60) (Figure 3). However, we found a significant difference when comparing the AUC of the PPR QPASREL with that of the ACL-RSI (0.73 [95% CI, 0.66-0.80]; P = .02). Similarly, a significant difference was observed between the AUC of the PSR QPASREL and the ACL-RSI (P = .01). The ACL-RSI exhibited superior discriminative capability in predicting 1-year RTS in patients compared with both the PSR QPASREL and the PPR QPASREL.
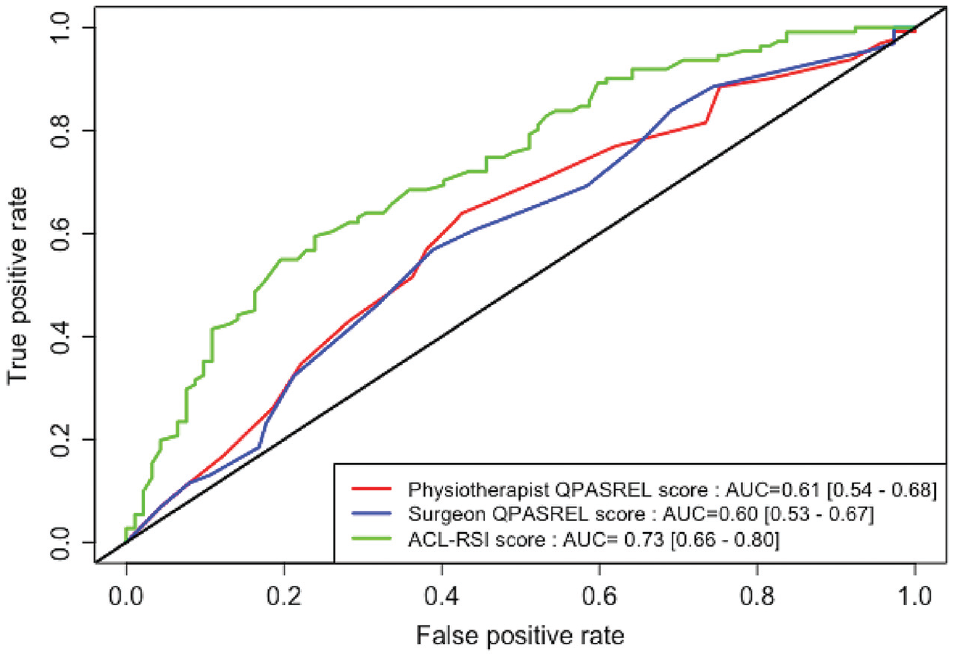
Comparative receiver operating characteristic curve analysis of the QPASREL score for PPR and PSR and the ACL-RSI score for predicting return to sport at 1 year after anterior cruciate ligament reconstruction. ACL-RSI, Anterior Cruciate Ligament–Return to Sport After Injury; AUC, area under the curve; PPR, patient-physical therapist relationship; PSR, patient-surgeon relationship; QPASREL, Quality of Patient-Surgeon Relationship.
In the correlation analysis, weak yet positive association was found between the QPASREL and the ACL-RSI for both PSR (rS = 0.19; 95% CI, 0.05-0.33; P = .008) and PPR (rS = 0.21; 95% CI, 0.08-0.34; P = .002).
Discussion
The main finding of this study was that higher QPASREL scores, indicating better PSR and PPR, were associated with an increased rate of RTS to the same preinjury level 12 months after ACLR.
Patient-Surgeon Relationship
Although the QPASREL was initially developed to evaluate the association between a better PSR and the return to work,6,7 the comprehensive question set of the QPASREL was found to be also effective for assessing PSR and PPR in the context of RTS. This score measures critical aspects of the patient-practitioner relationship such as communication (items 1, 2, 3, 7), availability/time management (items 4, 10), interprofessional collaboration (items 3, 6), and empathy (items 9, 11). Our results are in line with those of Kelley et al, 10 who demonstrated in their systematic review that a high-quality patient-practitioner relationship is associated with better outcomes, especially in patients with osteoarthritis and diabetes. Our data extend these findings by providing evidence within the context of ACLR. Specifically, higher scores of empathy (item 9), communication (items 1, 2), guidance (item 5), and discussion of return-to-work conditions (item 8) were particularly associated with a successful RTS. Our findings underscore the significance of these aspects of the PSR and encourage practitioners to develop this area of their skills to enhance RTS outcomes after ACLR.
Van Eck et al 24 performed a randomized controlled trial on 177 patients to investigate the impact of improving PSR, through a web-enhanced education, on patient satisfaction after knee and shoulder surgery (including ACLR). Patient satisfaction was assessed through the Outpatient and Ambulatory Surgery Survey Consumer Assessment of Healthcare Providers and Systems. The results showed statistically higher satisfaction scores in the study group for the “recovery” core measure, which includes questions about the ability to manage pain, instructions for postoperative care, communication with health care providers, and overall satisfaction with the recovery process. Building on the study by van Eck et al, we observed that when patients had a high-quality PSR and PPR when categorized by QPASREL data quartiles, there was a significantly higher rate of RTS, with ORs ranging from 2.17 (PPR QPASREL score >39; P = .0497) to 2.89 (PSR QPASREL score >38; P = .009). Furthermore, the highest category (scores >38 for PSR and >39 for PPR) showed a stronger statistical significance for RTS in favor of PSR (Padj = .043) compared with PPR (Padj = .12).
In a 2022 study, Chapon et al 3 aimed to understand how patients choose their surgeon for ACLR. Results on 105 patients showed that the primary criterion was the clarity of information provided (items 2, 7, and 8 of the QPASREL), followed by wait times for consultation and surgery and then the surgeon's reputation. 3 Chapon et al concluded that trust and recommendations are essential in PSR and that quality of information is crucial in the decision-making process. Our study showed that patients who completely agreed with items 2, 7, and 8 had increased odds of being in the RTS group.
Patient–Physical Therapist Relationship
Our data demonstrated that the OR of 5-point increases in PPR QPASREL score was associated with 39% odds of RTS. In their systematic review, Walker et al 25 found that patients perceived the therapeutic relationship, interaction with family and friends, self-motivation, fear of reinjury, organization/lack of time, and interpersonal comparison as the most common barriers to and facilitators of rehabilitation. In another study, Walker et al 26 demonstrated that a good relationship with the rehabilitation provider was regarded as the most important factor in facilitating rehabilitation.
One explanation of our results is that a low-quality PPR may contribute to kinesiophobia, potentially affecting the likelihood of a successful RTS. 16 This assertion is supported by the findings of Rodríguez-Nogueira et al, 20 who demonstrated that the empathy and high-quality communication of a physical therapist significantly affected the success of a therapeutic alliance. These aspects are tested by QPASREL items 1, 2, 3, 7, 9, and 11. In their systematic review, Mir et al 17 investigated the fear of reinjury as measured by the Tampa Scale of Kinesiophobia. Those investigators concluded that kinesiophobia negatively correlated with postoperative International Knee Documentation Committee scores and Knee injury and Osteoarthritis Outcome Score subscale values and positively correlated with inability to RTS at preinjury level.
Patient-Clinician Relationship and Psychological Readiness to RTS at 6-Month Follow-up
Although our study established the relevance of the QPASREL score in predicting RTS to preinjury levels, the predictive capacity of the QPASREL score was less potent than that of the ACL-RSI score. The AUC for QPASREL fell within a weak range, indicating that it alone may not be a reliable predictor of RTS. In fact, we did not aim to replace the ACL-RSI with QPASREL but rather to highlight the association of PSR and PPR with RTS outcomes. Clinicians are encouraged to enhance these relationships by improving communication, empathy, and clarity of the information transmission. The weak yet positive correlation between the QPASREL and ACL-RSI suggests that an improved PSR and PPR may help boost the psychological readiness to RTS by instilling confidence and decreasing fear of reinjury. This hypothesis is supported by results from Marok and Soundy, 15 who emphasized the importance of PPR and urged that physical therapists use a range of techniques to help individuals overcome kinesiophobia and improve their functional outcomes.
Our findings are in line with previous studies showing the high impact of psychological readiness on RTS.4,27,28 In their review of the functional outcomes of ACLR, Marok and Soundy 15 concluded that physical therapists need to use a range of physical therapy techniques, such as motor imagery and rehabilitation, to assist individuals to overcome their kinesiophobia and improve their functional outcomes. Wu et al 28 emphasized the potential negative impact of psychiatric comorbidities, such as depression, on postoperative recovery. Finally, Christino et al 4 found that high levels of self-esteem significantly influenced RTS outcomes after ACLR.
An important consideration in interpreting our results is the potential cause-and-effect aspect of this association. Indeed, a better relationship with the surgeon or therapist may encourage better postoperative compliance and motivation, contributing to a successful outcome. Similarly, excellent postoperative progress could lead patients to think more highly of their surgeon or therapist. Both possibilities reinforce the hypothesis of the significant impact of psychological factors as a primary player in the RTS outcome.
Limitations
The limitations of the study include its monocentric nature and lack of matching technique. Being observational, this study cannot establish causality but only associations. Additionally, the QPASREL questionnaire was completed 6 months postoperatively, which might be susceptible to recall bias. However, it was important to select a timeline long enough to allow the patient to make clear and well-considered responses. Furthermore, although the QPASREL was assessed at 6 months, RTS may typically occur later after ACLR, between 9 and 12 months, especially for pivoting sports. This time gap may introduce discrepancies because the quality of the patient-practitioner relationship might change by this time. However, we believe that this is also one of the strengths of the study; by selecting this specific timeline, we aimed to minimize the influence of RTS on the PSR and PPR quality, thus potentially reducing confounding factors when drawing association conclusions. Another limitation is that we modified the original QPASREL when we used it regarding physical therapists, and this modification was not validated. Furthermore, item 1 in the QPASREL, addressing the provision of sick leave, is not applicable to physical therapists in all countries. This could introduce bias in our results. Future studies should consider modifying or omitting this item for clarity. Finally, a minimal clinically important difference for the QPASREL score has not been established, making it challenging to definitively assess the clinical relevance of these differences.
Conclusion
Both PPR and PSR as measured by QPASREL were found to be significantly associated with patient RTS after ACLR. There was a weak yet positive correlation between QPASREL and ACL-RSI. The predictive capacity of the QPASREL score was less potent when compared with the ACL-RSI score.
Footnotes
Appendix
Comparative Analysis of PPR QPASREL Item Responses According to the RTS Group a

| PPR QPASREL Item | No RTS |
RTS |
P |
|---|---|---|---|
| 1. I can easily obtain recommendations for sick leave certificates from my physical therapist. |
|
||
| Strongly disagree | 6 (5.3) | 9 (6.9) | |
| Tend to disagree | 21 (18.6) | 6 (4.6) | |
| Agree | 47 (41.6) | 52 (40.0) | |
| Strongly agree | 39 (34.5) | 63 (48.5) | |
| 2. My physical therapist avoids using medical vocabulary so I can understand him/her. | .496 | ||
| Strongly disagree | 1 (0.9) | 0 (0.0) | |
| Tend to disagree | 8 (7.1) | 5 (3.8) | |
| Agree | 53 (46.9) | 65 (50.0) | |
| Strongly agree | 51 (45.1) | 60 (46.2) | |
| 3. I find that information is communicated properly and consistently between the different professionals (general practitioner, surgeon, rheumatologist, psychologist, etc) who take care of my condition, including my physical therapist. | .398 | ||
| Strongly disagree | 13 (11.5) | 8 (6.2) | |
| Tend to disagree | 28 (24.8) | 32 (24.6) | |
| Agree | 41 (36.3) | 50 (38.5) | |
| Strongly agree | 31 (27.4) | 40 (30.8) | |
| 4. I am satisfied with the availability of my physical therapist (in person or by phone) when I need him/her. |
|
||
| Strongly disagree | 0 (0.0) | 1 (0.8) | |
| Tend to disagree | 17 (15.0) | 4 (3.1) | |
| Agree | 38 (33.6) | 43 (33.1) | |
| Strongly agree | 58 (51.3) | 82 (63.1) | |
| 5. My physical therapist tells me when I can go back to work or that I cannot go back to work. | .067 | ||
| Strongly disagree | 3 (2.7) | 4 (3.1) | |
| Tend to disagree | 13 (11.5) | 6 (4.6) | |
| Agree | 47 (41.6) | 44 (33.8) | |
| Strongly agree | 50 (44.2) | 76 (58.5) | |
| 6. My physical therapist regularly informs my doctor about my care management and about the progress of my health problem. | .823 | ||
| Strongly disagree | 25 (22.1) | 29 (22.3) | |
| Tend to disagree | 48 (42.5) | 50 (38.5) | |
| Agree | 26 (23.0) | 30 (23.1) | |
| Strongly agree | 14 (12.4) | 21 (16.2) | |
| 7. My physical therapist is patient when I do not understand what he/she says. | .071 | ||
| Strongly disagree | 2 (1.8) | 0 (0.0) | |
| Tend to disagree | 3 (2.7) | 5 (3.8) | |
| Agree | 54 (47.8) | 46 (35.4) | |
| Strongly agree | 54 (47.8) | 79 (60.8) | |
| 8. My physical therapist discussed the conditions of my return to work with me. |
|
||
| Strongly disagree | 2 (1.8) | 3 (2.3) | |
| Tend to disagree | 13 (11.5) | 8 (6.2) | |
| Agree | 54 (47.8) | 40 (30.8) | |
| Strongly agree | 44 (38.9) | 79 (60.8) | |
| 9. My physical therapist understands the impact of pain and disability on my mood. | .050 | ||
| Strongly disagree | 1 (0.9) | 0 (0.0) | |
| Tend to disagree | 10 (8.8) | 4 (3.1) | |
| Agree | 53 (46.9) | 53 (40.8) | |
| Strongly agree | 49 (43.4) | 73 (56.2) | |
| 10. I'm satisfied with the time allotted to me by my physical therapist during consultation. | .067 | ||
| Strongly disagree | 0 (0.0) | 1 (0.8) | |
| Tend to disagree | 12 (10.6) | 5 (3.8) | |
| Agree | 46 (40.7) | 47 (36.2) | |
| Strongly agree | 55 (48.7) | 77 (59.2) | |
| 11. My physical therapist encourages me to talk about my concerns and listens to me carefully. |
|
||
| Strongly disagree | 0 (0.0) | 1 (0.8) | |
| Tend to disagree | 14 (12.4) | 3 (2.3) | |
| Agree | 52 (46.0) | 61 (46.9) | |
| Strongly agree | 47 (41.6) | 65 (50.0) | |
Data are reported as n (%). Boldface P values indicate statistically significant difference between RTS groups (P < .05). PPR, patient-physical therapist relationship; QPASREL, Quality of Patient-Surgeon Relationship; RTS, return to sports.
Final revision submitted November 20, 2023; accepted December 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: N.L. has received consulting fees from WebSurvey Society. F.K. has received consulting fees from Newclip. A.H. has received consulting fees from Arthrex and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Groupe Hospitalier Pitié Salpêtrière.