
Abstract
Background:
The success of glenoid augmentation procedures depends on accurate placement and healing of the graft to the glenoid. Different glenoid augmentation techniques have been described, but no comparative studies between them exist.
Purpose:
To assess the bone graft position, healing, and resorption in a group of patients treated with 1 of 4 procedures: arthroscopic anterior bone-block procedure using either (1) fresh-frozen iliac crest allograft or (2) iliac crest autograft, (3) open Latarjet, or (4) arthroscopic Latarjet.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 40 patients (87.5% men; mean age, 29.5 ± 7.9 years) were included, with 10 patients in each of the procedure groups. The graft position in the axial and sagittal planes was assessed on postoperative computed tomography (CT). Graft healing and resorption were assessed in a second CT scan performed 1 year postoperatively. Qualitative variables were compared between the 4 procedures using the chi-square test, and quantitative variables were compared with the Student t test or Mann-Whitney U test.
Results:
No differences were found between the procedures in the axial or sagittal position. The healing rate was significantly lower in the allograft bone-block group (20%) compared with the autograft bone-block (80%), open Latarjet (90%), and arthroscopic Latarjet (90%) groups (P < .001). Graft resorption developed in 17 of 40 (42.5%) cases overall. Osteolysis occurred in 100% of cases in the allograft bone-block group compared with 50% in the autograft group, 20% in the open Latarjet group, and 0% in the arthroscopic Latarjet group (P < .001). The glenoid surface area on 1-year CT scan was significantly lower in the allograft bone-block group compared with the autograft bone-block, open Latarjet, and arthroscopic Latarjet groups (P < .001).
Conclusion:
Arthroscopic bone-block, open Latarjet, and arthroscopic Latarjet procedures provided accurate bone graft positioning. However, very high rates of osteolysis and nonunion were observed in the iliac crest fresh-frozen allograft bone-block procedure when compared with the other procedures.
Glenohumeral instability is a common condition frequently affecting the young, active population. Anteroinferior glenoid bone loss has been reported in up to 90% of patients with glenohumeral instability. 49 In these cases, isolated soft tissue repair procedures have a higher risk of failure, and anterior glenoid bone augmentation may be required.11,49 Different procedures have been described to address bone loss by glenoid bone grafting, using either a coracoid graft (Latarjet procedure) or free bone grafts, most frequently iliac crest allograft or autografts. 10
The success of glenoid augmentation procedures depends on accurate placement and healing of the graft to the glenoid.7,27,38 A position that is too medial is associated with an increased rate of recurrence, 1 while placing the graft laterally may result in early glenohumeral osteoarthritis. 27 Optimal sagittal bone-block positioning may reduce complications such as recurrent instability or neurologic injury when placing the graft too high or a higher risk of mechanical failure and nonunion if placing the graft too low.44,45 Nonunion and resorption could also result in a higher rate of recurrent shoulder instability, residual pain, or worse functional outcomes.7,29,38
Overall, good results have been reported in terms of positioning in both the open and arthroscopic Latarjet procedures.8,24 Positioning of the graft has also been noted to be accurate when performing an arthroscopic bone-block procedure.6,42 However, concern exists regarding graft osteolysis, which has been found to occur in up to 100% of the patients who underwent a Latarjet procedure8,41 and 100% of those operated on with iliac crest grafts. 5 In addition, whether these results may depend on the technique or graft chosen is unknown.
The purpose of this study was to assess and compare bone graft position, integration, and resorption, in a group of patients with anterior glenohumeral instability and glenoid bone loss treated using 1 of 4 procedures: arthroscopic bone block with an iliac crest allograft, arthroscopic bone block with an iliac crest autograft, open Latarjet, or arthroscopic Latarjet.
Methods
After receiving ethics committee approval, we conducted a prospective, multicentric, 4-cohort study of patients with anterior glenohumeral instability and glenoid bone loss who were managed surgically with a glenoid augmentation technique between 2017 and 2020 at 3 high-volume university hospitals. The inclusion criteria for the participants were (1) ≥18 years old; (2) having a glenoid bone loss >5% on preoperative CT scan; (3) having undergone an open or arthroscopic Latarjet procedure or an arthroscopic bone-block procedure using iliac crest graft, allograft, or autograft; and (4) availability of preoperative and postoperative CT scans performed 3 and 12 months after the surgical procedure. Excluded were patients with (1) posterior, multidirectional, or atraumatic instability; (2) previous glenohumeral osteoarthritis; and (3) a previous glenoid bone augmentation procedure.
Surgical Technique
The type of surgery and kind of graft used were based on surgeon preference. Surgeries were performed by 3 senior shoulder surgeons (E.C., P.C., M.A.R.I.).
The bone-block procedure was performed as described by Taverna et al 42 using iliac crest graft, either fresh-frozen allograft or autograft, prepared to obtain a 20 × 10 × 10-mm block and fixed with a double suture button (Smith&Nephew). If a large or deep engaging Hill-Sachs lesion was observed, a remplissage procedure was performed. The arthroscopic Latarjet procedure was carried out as described by Calvo et al 13 using the arthroscopic screws Latarjey system (DePuy Mitek). The open Latarjet procedure was performed using screws as described by Patte et al, 34 with the addition of a plate when needed. 15
CT Evaluation
All CT measurements were performed by a fellowship-trained shoulder and elbow surgeon (C.D.) Preoperative glenoid bone loss was evaluated using the Pico method. 3 The Hill-Sachs lesion was measured with the method described by Saito et al. 37 The glenoid track was evaluated as defined by Yamamoto et al 49 and Di Giacomo et al. 17
The graft position in the axial and sagittal planes was assessed on postoperative CT scans obtained from all patients throughout the first 3 months after surgery. On the en face view of the glenoid, 2 circles (1 inferior and 1 superior) were drawn: a best-fit circle to the posteroinferior glenoid and a circle superior and tangent to the glenoid margins. The line connecting the center of both circles defined the vertical height of the glenoid. 2 The axial position of the bone block was evaluated as described by Kany et al 24 at the level of 25% and 50% of the glenoid height. At both 25% and 50% of the glenoid height, a circle was drawn along the curvature of the glenoid surface. The distance (in mm) between the tip of the graft and the circumference was measured (Figure 1).
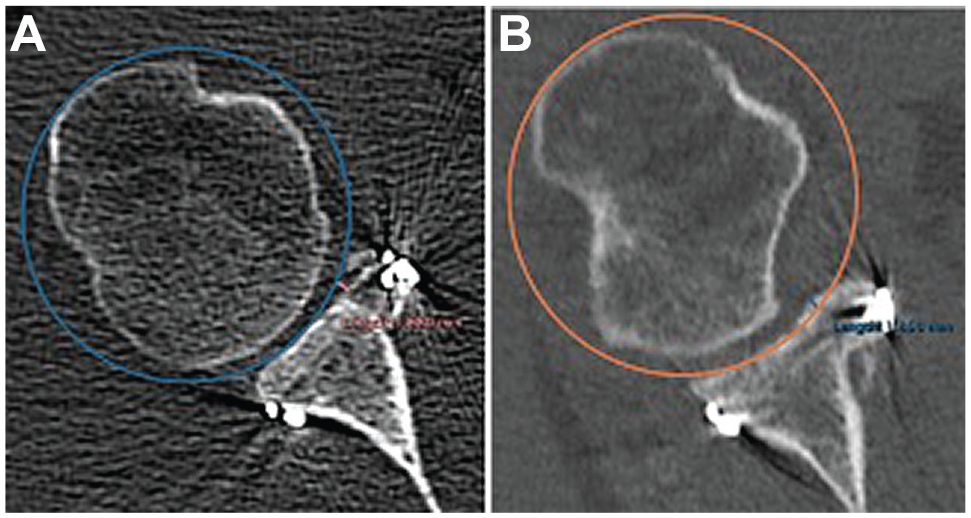
Axial position evaluation on computed tomography. A circle along the glenoid rim was drawn, and the distance between the tip of the graft and the circle was measured. (A) Mildly medialized graft. (B) Slightly lateralized graft.
The graft was considered accurate (flush) if positioned between 3 mm lateral and 5 mm medial relative to the circumference. Grafts were defined as lateral if placed >3 mm lateral. Bone blocks positioned >5 mm medially were considered medial. 24 Regarding the sagittal position of the graft, a different method was used for the evaluation of free bone blocks and the Latarjet procedure. In the patients undergoing a free iliac crest graft, the vertical bone-block location was evaluated using the “defect coverage index method,” as described by Delgado et al. 14 The length of the bone defect and amount of graft covering the defect were measured (Figure 2).

Sagittal position evaluation of the bone-block procedure on computed tomography. The percentage of coverage was obtained using the formula (A/B) × 100, where A is the amount of glenoid defect covered by the graft and B is the length of the bone defect. (A) Coverage >90%. (B) More than 10% of the bone defect is uncovered.
Positioning of the graft on the sagittal plane was classified as accurate if the graft covered at least 90% of the defect. In the Latarjet procedure, the amount of graft below the glenoid equator was measured and considered accurate when >75% of the graft was located below the glenoid equator 33 (Figure 3).

Sagittal position evaluation of the Latarjet procedure on computed tomography. The percentage of graft below the glenoid equator (dotted line) was obtained using the formula (A/B) × 100, where A is the length of the graft and B is the amount of graft above the equator.
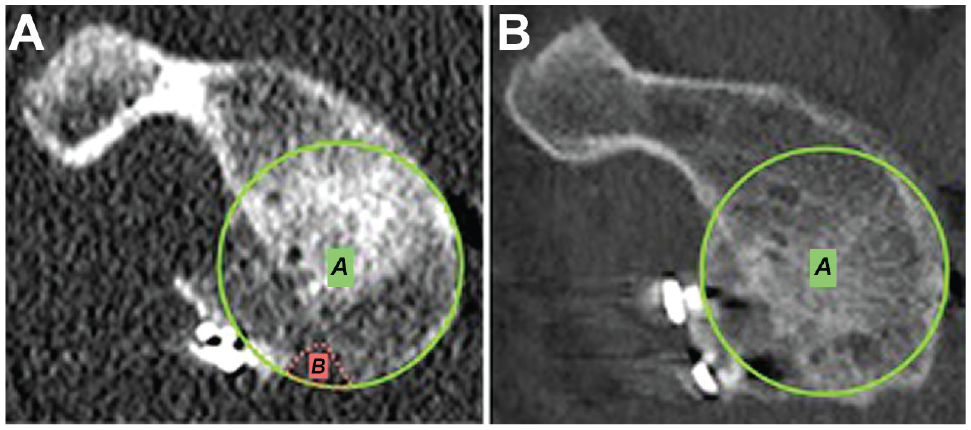
At the 1-year follow-up, the CT scans of all patients were evaluated for graft healing and resorption. Graft healing was defined as the inability to identify the contiguous cortical profiles between the graft and glenoid rim (Figure 4). Fusion was considered as established when >35% of the graft had bone unions to the glenoid surface. 36

Healing evaluation on axial computed tomography. (A) A healed graft. (B) No bony bridges are observed; thus, the graft was considered unhealed.
For the evaluation of resorption, the outline of the coracoid graft was manually traced on serial axial images using 3-dimensional reconstruction software (Horos Version 3.3.6; Pixmeo). Then, we used the ROI (region of interest) segmentation tool to create a volume rendering of the graft (Figure 5). The volumes obtained at the first postoperative CT scans were compared with the 12-month postoperative volumes. Osteolysis was considered when a >20% decrease of the volume occurred, as suggested by Haeni et al. 23

For osteolysis evaluation, graft volume was obtained on computed tomography. (A and B) The contour of the bone graft was manually defined in the axial plane using the close polygon tool in different heights. (C) The entire volume (in cm3) was automatically generated using 3-dimensional reconstruction software.
The glenoid surface area 31 (as a percentage) was analyzed on the postoperative and 12-month CT scans with the Pico method, and residual bone defects were noted (Figure 6).
The glenoid surface area, A, and residual glenoid bone loss, B, were measured on computed tomography according to the Pico method. (A) Residual bone loss is observed. (B) The glenoid surface area is fully restored.
Clinical Assessment
Recurrence after surgery and intraoperative and postoperative (immediate and late) complications, including neurovascular injuries, infection, or loss of range of movement, were recorded. Also, return to previous sports was evaluated and graded into 4 categories: 0, no return to sports activity; 1, partial recovery; 2, subtotal recovery; or 3, complete recovery.
Statistical Analysis
Statistical analysis was performed using SPSS Version 26 (IBM). The normality of data was assessed using the Kolmogorov-Smirnov test. Qualitative variables were analyzed using frequencies and percentages and compared using the chi-square test. Quantitative variables were presented as the mean and standard deviation or median and interquartile range. The Student t test was used to compare parametric quantitative variables, and the Mann-Whitney U test was used for nonparametric data. Correlations between potential preoperative risk factors and evaluated outcomes were assessed using the logistic regression test. The statistical threshold for significance was established at P < .05.
Results
A total of 40 patients (87.5% men, mean age 29.5 ± 7.9 years) complied with the inclusion criteria and had full CT assessment at the 3 established time points. The characteristics of all participants are summarized in Table 1. The groups (10 patients in each group) were homogeneous in terms of preoperative features, but bone loss was significantly higher in the open Latarjet group compared with other procedures (P = .015). The mean preoperative glenoid bone loss was 15.2% ± 3.9%. Remplissage was added in 90% of the patients in the allograft bone-block group and 60% of the cases in the autograft bone-block group. In the arthroscopic Latarjet group, an anterior capsulolabral reattachment was performed in 60% of the patients. Finally, the capsule was reattached to the coracoacromial ligament remanent in 100% of the patients who underwent an open Latarjet procedure. No intraoperative or immediate postoperative complications occurred.
Patient Characteristics and Preoperative Clinical and Imaging Features of the 4 Study Groups a

Data are reported as n (%) unless otherwise indicated. Boldface P value indicates a statistically significant difference between groups (P < .05). ABER, abduction and external rotation.
The mean time to initial postoperative CT scan was 3.71 ± 1.1 months. In the axial view, the bone graft was placed flush with the glenoid rim in 38 of the 40 (95%) cases. In the sagittal plane, accurate graft positioning was obtained in 90% (36/40) of patients. No differences were found in the axial (P = .32) or sagittal (P = .528) position between the procedures. The bone graft was optimally positioned in the vertical and horizontal planes in 90% (36/40) of all patients. No significant differences were found between the 4 groups (Table 2).
Postoperative Imaging Outcomes a
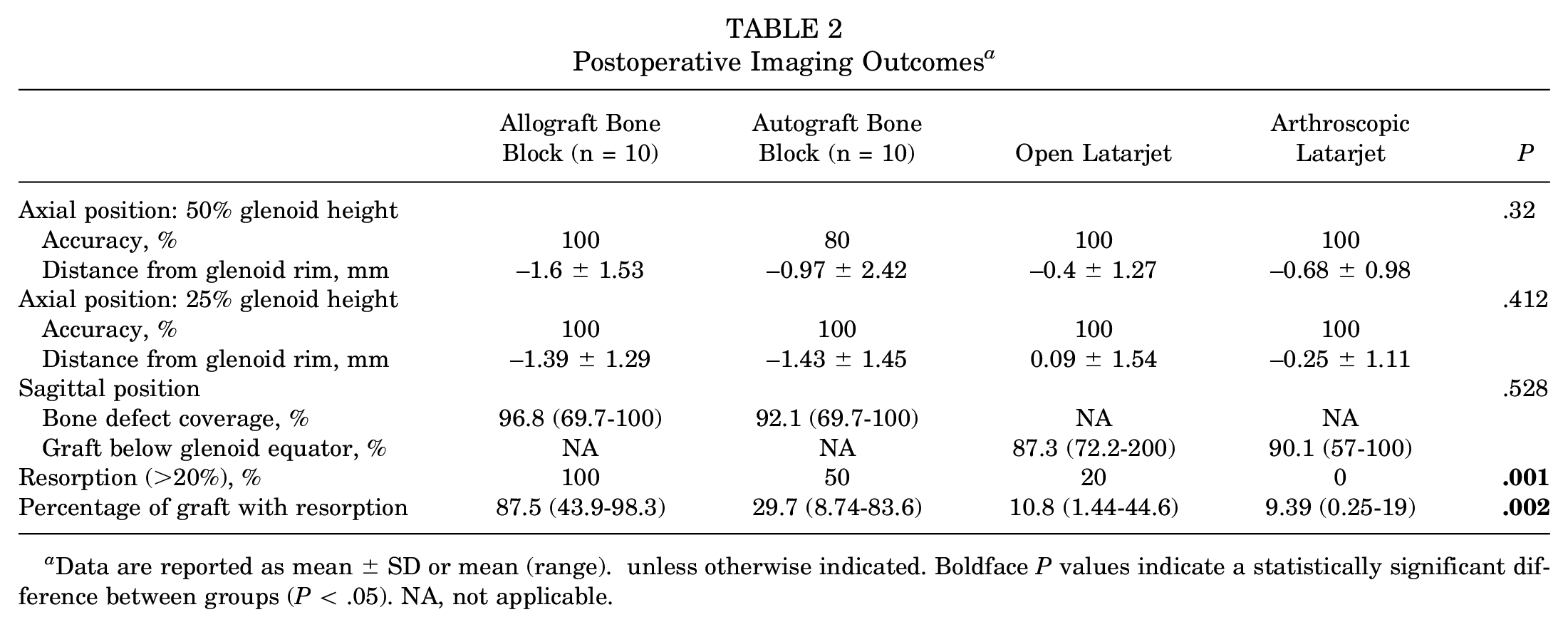
Data are reported as mean ± SD or mean (range). unless otherwise indicated. Boldface P values indicate a statistically significant difference between groups (P < .05). NA, not applicable.
Graft integration and resorption were evaluated by CT scan at a mean of 17.4 ± 8.27 months of follow-up. The healing rate was significantly lower in the allograft bone-block group (20%) compared with the autograft bone-block (80%), open Latarjet (90%), and arthroscopic Latarjet (90%) groups (P < .001) (Table 2). The overall incidence of bone-block resorption was 42.5% (17/40). In the allograft bone-block group, osteolysis occurred in 100% of cases versus 50% in the autograft bone-block and 20% in the open Latarjet groups (P < .001). No resorption occurred in the arthroscopic Latarjet group.
On 1-year CT, the glenoid surface area was significantly lower in the allograft bone-block group compared with the autograft bone-block, open Latarjet, and arthroscopic Latarjet groups (P < .001) (Figure 7). In addition, on the 1-year CT scan, a significant reduction of the glenoid surface area was observed compared with the initial (3-month postoperative) CT scan in the allograft bone-block group (from 98.5% [range, 96.6%-100%] to 93.3% [range, 88.3%-96%]; P = .005), in the autograft bone-block group (from 99.2% [range, 96.3%-100%] to 96.8% [range, 94.5%-98,8%]; P = .005), and in the open Latarjet group (from 98.5% [range, 91.4%-100%] to 95.8% [range, 91.3%-98.6%]; P = .005). No significant reduction occurred in the arthroscopic Latarjet procedure. At 16.3 ± 4.7 months of follow-up, the glenoid surface area was restored in only 10% (1/10) of patients in the allograft bone-block group compared with 80% in the autograft bone-block group, 80% in the open Latarjet group, and 90% in the arthroscopic Latarjet (P = .004). The multivariate regression analysis showed no association between preoperative features and position, healing, and resorption rates.

Mean glenoid surface area preoperatively, postoperatively, and at the final follow-up.
At the final follow-up (33.3 ± 10.1 months), all patients remained stable except for 1 patient in the allograft bone-block group. No intraoperative complications occurred. At the 3-month follow-up, 2 patients, 1 in the arthroscopic Latarjet group and 1 in the autograft bone-block group, showed loss of external rotation, and 1 patient in the allograft bone-block group showed scapular dyskinesis. All 3 patients underwent a specific physical therapist program recovering shoulder range of movement and function. Regarding athletic activity, 83.3% of patients returned to their previous activity level, with no significant differences between groups (P = .183).
Discussion
The main finding of this study was that the arthroscopic bone-block procedures as well as the open and arthroscopic Latarjet procedures can provide accurate bone graft positioning with glenoid bone stock restoration. However, patients treated with the iliac crest allograft bone-block procedure were found to have significantly higher nonhealing and resorption rates when compared with those who had undergone iliac crest autograft bone-block and Latarjet procedures.
When significant glenoid bone loss is present in anterior shoulder instability, glenoid bone augmentation should always be considered. 12 The bone defect can be solved by transferring the coracoid (Latarjet) or through the use of free bone grafts, such as an iliac crest, distal tibia allograft, distal clavicle, or scapular spine autograft. The Latarjet procedure has shown to be an effective technique in the management of patients with anterior glenohumeral instability and bone loss.4,8,21 However, it is not devoid of complications such as glenohumeral osteoarthritis, restricted shoulder range of movement, and neurological or vascular lesions.20,21 In addition, it is a nonanatomic technique, and a split of the subscapularis muscle is required, which may lead to damage of the muscle. 43 The bone-block procedure has recently emerged as an alternative for the management of patients with subcritical bone loss and reparable soft tissue injuries. 42 It allows an anatomic reconstruction while preserving the subscapularis tendon and avoiding neurovascular damage.20,40 Studies comparing Latarjet and bone-block procedures are limited. Moroder et al 32 performed a randomized controlled prospective study comparing clinical results at 24 months between an open Latarjet procedure and an arthroscopic bone-block technique in patients with recurrent anterior shoulder instability and glenoid bone loss and found no differences in recurrence rate and clinical outcomes. However, the authors did not analyze radiological outcomes. Similarly, Gilat et al 19 published a systematic review comparing the outcomes between the Latarjet and bone-block procedures, showing no differences in terms of recurrence, complication rate, progression of osteoarthrosis, and return to sports, but again, no radiological data comparison was provided.
The success of bone-block procedures depends on both accurate placement of the graft and its proper integration to the anterior glenoid bone. 30 According to our results, all surgical procedures presented (bone block, arthroscopic, and open Latarjet) allow for accurate positioning of the graft in both the axial and the sagittal plane. Previous studies analyzing glenoid bone augmentation procedures have shown accurate positioning of the graft: Taverna et al 42 and Boileau et al, 6 using the same technique as we did, both reported that 100% of bone blocks were optimally positioned in the axial plane. The sagittal position of the graft was accurate in 92.3% of bone blocks according to the first authors 42 and in 100% according to the second authors. 6 Similar results were reported by Russo et al 36 and Zhu et al, 51 who found an accurate position of the graft in 100% of the patients who underwent an open Latarjet procedure and in 96% and 91.3%, respectively, of those who underwent an arthroscopic Latarjet technique. Moreover, when the open and arthroscopic Latarjet procedures are compared, good positioning results with no differences between groups are found,25,36,51 as observed in our series.
In our study, graft healing was observed in 28 (70%) of patients. Healing was achieved in only 2 (20%) patients in the allograft bone-block group versus 80% of the cases in the autograft bone-block group and 90% in the arthroscopic and open Latarjet groups (P < .001). Healing rates reported in the literature vary widely. In a systematic review analyzing the results of both allograft and autograft iliac crest bone-block procedures, Gilat et al 19 did not find differences between the 2 groups, with a mean healing rate of 78%. Zhao et al 50 and Sayegh et al 39 both found that graft was integrated in 100% of the allografts, a finding that is in strong contrast with the rates found in our study. When analyzing autograft, we found that integration was obtained in 80% of the patients in our series, similar to the 58% healing rate reported by Giannakos et al. 18 Better healing rates were achieved by Boileau et al, 6 who found, after a mean follow-up of 21 months, a 100% healing rate. Regarding the Latarjet procedure, a 90% rate of healing was found in both the arthroscopic and open procedures in our series, similar to the 95% and 95.3% healing rates reported in literature.8,26 Discrepancy between different studies may be a consequence of the lack of agreement in the healing evaluation method and the threshold to consider significant findings.
Significant osteolysis was observed in all patients who underwent an arthroscopic bone-block procedure with iliac crest allograft. Massive resorption of iliac crest allografts was also observed by Boehm et al, 5 who found a significant resorption of the graft in 10 patients assessed at 1-year follow-up. A higher resorption rate was also found by Wong et al 47 with glenoid reconstruction using distal tibia allograft compared with coracoid autograft (73% vs 42%). Two years later, when analyzing their series of 72 patients undergoing an arthroscopic bone-block procedure using distal tibia allograft, Wong et al found a 100% union rate and graft resorption <50% in 86% of patients, much lower than the resorption rate found in our study. On the other hand, when using the autograft bone-block procedure, just 50% of patients experienced osteolysis in our study, a similar rate to the one reported by Hachem et al, 22 who found resorption in 32.5% of patients, with a higher resorption rate at the peripherical area when compared with the areas with glenoid contact.
Conversely, osteolysis occurred in only 20% of the patients who underwent an open Latarjet procedure and in none of the patients in the arthroscopic Latarjet group. These rates are lower than the ones reported in literature. Di Giacomo et al 16 noted a 60% rate of complete coracoid osteolysis in 26 patients who underwent an open Latarjet procedure. Zhu et al 52 also reported high rates of osteolysis with major resorption found in 50% of cases, as well as higher rates in patients who underwent an open Latarjet procedure compared with the arthroscopic Latarjet technique. Finally, with regard to the arthroscopic Latarjet procedure, Kordasiewicz et al 26 found osteolysis in 70% of patients, but resorption affected the whole coracoid in only 1 patient. In our study, significantly higher rates of osteolysis were observed in patients with the iliac crest allograft bone-block procedure compared with the other groups. One explanation for this finding could be that allografts are devascularized, 39 whereas the coracoid in the Latarjet group maintains blood supply through the conjoined tendon. Moreover, because of its allogenic origin, immunological factors such as production of bone protein antibodies and osteoclast activity may be increased, thus leading to a higher level of resorption.5,47
Interestingly, despite this high resorption rate, a redislocation event was reported in only 1 patient of the bone-block group. Similar findings were found in the study by Boehm et al, 5 who reported on 10 patients who underwent the allograft bone-block procedure. Despite observing total resorption of the allografts, no postoperative recurrence was noted. However, in both the studies by Boehm et al and our series, the minimum follow-up was set as 12 months. Because many recurrences occur after 1 year postoperatively, ours could be considered insufficient follow-up to detect postoperative recurrence. In addition, different preoperative and intraoperative features (ie, smoking, age, amount of bone defect, type of allograft including both its preservation [fresh, cryopreserved] and source [distal tibia, 35 spine of the scapula 48 ], or fixation device) could affect osteolysis but could not have been assessed in our series given the small sample size. Therefore, further long-term follow-up studies with larger samples are needed to identify the clinical repercussions of our findings and potential risk factors for osteolysis development. It is also noteworthy that similar to the disparity mentioned with healing evaluation, disparity of results in literature may be due to the lack of an established method and threshold in the evaluation of resorption.
It is important to note that in the 4 procedures a minimum rate of osteolysis occurred. This resorption phenomenon has been suggested to be physiological secondary to the remodeling process. According to Wolff's law, 46 the bone under no stress would undergone osteolysis. Commonly, in the glenoid augmentation procedures the harvested grafts are bigger than the glenoid defect. As a result, part of the graft would be superfluous and therefore may not be under stress, thus experiencing osteolysis. This is the reason that we have considered it important to analyze glenoid surface area restoration: a progressive reduction of the previously restored glenoid surface area occurred in the 4 procedures after 1 year. However, at the final evaluation, the glenoid surface area in the allograft bone-block group was significantly smaller compared with the other groups. Moreover, the glenoid surface area was only restored in 1 (10%) patient. Because the purpose of bone-block procedures is basically to restore the glenoid surface area, the allograft bone-block procedure can be considered a failure in 90% of patients. Regarding the autograft bone-block, open Latarjet, and arthroscopic Latarjet procedures, as previously stated, we also observed a reduction in the glenoid surface area from immediate postoperatively to 1 year postoperatively. However, besides partial graft resorption, restoration of the glenoid surface area was obtained in 80%, 80%, and 90% of patients, respectively.
Our findings may be relevant because the arthroscopic bone-block procedure using iliac crest allograft, despite its accuracy in positioning of the graft, has shown to have unsatisfactory resorption rates. Therefore, other options should be explored to find a graft with lower resorption rates. Scapula spine has recently emerged as a possible alternative to iliac crest autograft. 48 Authors attribute to this graft the advantage of being an autologous graft; thus, it would have foreseeably better healing and osteolysis rates. In addition, harvesting of the scapular spine graft is safe, with fewer complications compared with iliac crest harvesting. 48
Limitations
This study has some limitations. First, the sample is clearly small, and no formal determination of the sample size was made; thus, the risk of type 2 error should be acknowledged. However, we wanted to compare 4 relatively homogeneous populations of patients. Moreover, only patients with 3- and 12-month postoperative CT scans available were included in the study, thus making the recruitment more difficult. In addition, the use of iliac crest allografts was ended in our institution because of the observed high rates of resorption, and consequently, no further patients were enrolled in this study. Second, it was a multicenter study, thus a potential heterogeneity bias exists. However, surgeries were always performed by senior surgeons, thus reducing bias related to experience or learning curve and variability between surgeons. In addition, all radiological measurements were performed by the same fellowship-trained shoulder surgeon. Third, measurements were manually drawn. However, the assessment methods used have previously been demonstrated to be reliable.9,28 Fourth, the true clinical relevance of these findings is still unknown. Therefore, studies specifically designed to determine the repercussions of these results on clinical performance are needed.
Conclusion
The arthroscopic bone-block, open Latarjet, and arthroscopic Latarjet procedures were all found to provide accurate bone graft positioning. However, very high rates of osteolysis and nonhealing were observed in the iliac crest fresh-frozen allograft bone-block procedure when compared with the other procedures.
Footnotes
Final revision submitted October 24, 2023; accepted November 16, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital Universitario Ramón y Cajal (protocol No. 0.92, approved under Act 400).