
Abstract
Background:
Research at the intersection between social determinants of health (SDOH) and orthopaedics remains an area of active exploration, with recent literature demonstrating significant disparities in a wide array of orthopaedic outcomes in patients with different SDOH.
Purpose/Hypothesis:
The purpose of this study was to use a validated composite measure of SDOH mapped to census tracts (Child Opportunity Index [COI]) to explore disparities in functional outcomes after anterior cruciate ligament (ACL) reconstruction. It was hypothesized that patients with a lower COI score would have delayed surgical care and worse functional outcomes after ACL reconstruction.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Demographic, surgical, and functional outcomes data were extracted for all patients aged ≤18 years who underwent primary ACL reconstruction at our institution between 2009 and 2019. Strength deficits were calculated, and COI quintile scores were obtained. One-way analysis of variance, the chi-square test, and the Fisher exact test were used to compare variables of interest between the lower 2 quintiles (low group) and the upper 2 quintiles (high group).
Results:
Of the 1027 patients, 226 (22.0%) were in the low group, while 801 (78.0%) were in the high group. There was a significantly greater time from injury to surgery in the low group than in the high group (98.15 ± 102.65 vs 71.79 ± 101.88 days, respectively; P < .001). The low group had a significantly lower extension-flexion range of motion at 1- and 3-month follow-up (P = .03 and P = .02, respectively) but no difference at 6-month follow-up (P = .27). The low group attended fewer physical therapy visits than the high group (24.82 ± 10.55 vs 37.81 ± 18.07, respectively; P < .001). The low group had significant deficits in quadriceps strength at 3, 6, and 9 months at 180 deg/s (P = .03, P < .001, and P = .01, respectively) and at 6 months at 300 deg/s (P = .002).
Conclusion:
In this study, we found that the COI was associated with disparities in key clinical outcomes including time to surgery, postoperative range of motion, and postoperative strength.
Social determinants of health (SDOH) are the set of factors and conditions within a patient's environment that can influence health outcomes. The study of SDOH has increasingly become an area of interest; the World Health Organization has named SDOH as an overarching focus in its Healthy People 2030 initiative.2,3,23 As in other medical specialties, research on the relation between SDOH and orthopaedic outcomes has become an area of active exploration, and recent literature has indeed demonstrated that SDOH can predict disparities in a wide array of orthopaedic outcomes.1,3,20 Previously, Bram et al 4 demonstrated that race and insurance status were associated with differences in severity of the injury, time to surgery, and postoperative outcomes in pediatric patients with anterior cruciate ligament (ACL) injuries. Increasingly, the investigation of SDOH has acknowledged that while individual social characteristics such as race and insurance status may influence health outcomes, it may be that the aggregate influence of multiple interrelated and overlapping conditions in the social environment is also an important predictor of outcomes, and understanding this may provide powerful insights into the design of effective interventions. To aid in the study of aggregate social conditions, a validated composite measure to holistically quantify SDOH—the Child Opportunity Index (COI)—was developed in 2014. The COI is an index measure composed of 29 different pediatric-focused social factors across 3 domains (education, health and environment, and social and economic) that quantifies the relative level of social opportunities for children present within a US census tract.18,19 An individual patient's address can be used to look up the COI score associated with that census tract. While the COI does not provide information about a child's individual social characteristics, it permits an aggregated investigation of neighborhood-level social circumstances as a potential predictor of outcomes.
Recently, Rosenberg et al 21 utilized the COI to examine the relationship between neighborhood conditions and time to ACL reconstruction. Our study aimed to expand on prior literature by further examining the relationship between both patient characteristics (race and insurance status) and aggregate social circumstances (COI score) and outcomes after an ACL rupture. We hypothesized that race, insurance status, and a lower COI score would be correlated with delayed ACL reconstruction and poorer functional outcomes and follow-up care.
Methods
After institutional review board approval, a query was conducted for all patients aged ≤18 years old who underwent primary ACL reconstruction at our institution between 2009 and 2019 with prior informed consent. Exclusion criteria included an insufficient follow-up or inadequate records for a chart review, a history of ipsilateral ACL surgery, concurrent multiligament reconstruction or fractures, congenitally absent ACLs, tibial or fibular hemimelia, patients who required a staged procedure for any reason, and patients who did not have satisfactory addresses recorded for COI data extraction. All procedures were completed by 3 fellowship-trained pediatric orthopaedic surgeons (T.J.G.).
Demographic information was extracted. Variables of interest included age, sex, self-reported race, body mass index classification, insurance status and type, home address, and zip code. Insurance types were divided into public versus private, with public insurance options comprising Medicaid or the Children's Health Insurance Program. Clinical variables of interest included date of presentation, date of surgery, concurrent injuries, intraoperative findings, postoperative complications, physical therapy attendance, and range of motion. During physical therapy, patients were evaluated for quadriceps and hamstring strength deficits. Deficits were calculated as a percentage difference between the contralateral extremity and the operative extremity. Postoperative complications were recorded as graft ruptures, contralateral ACL ruptures or medial or lateral meniscal injuries, hardware failure, infections, ipsilateral medial or lateral meniscal injuries, wound care issues, and other. Our institution's rehabilitation protocol after ACL reconstruction typically allows return-to-sports clearance after the 9-month follow-up appointment.
The COI was jointly developed by the Kirwan Institute for the Study of Race and Ethnicity at The Ohio State University and diversitydatakids.org, which is a project housed at the Heller School for Social Policy and Management at Brandeis University. Scores were extracted from diversitydatakids.org by generating a geographic identifier (GEO)ID for each patient and searching the COI database for the corresponding GEOID. 6 This GEOID was generated by converting the patient's address at the time of surgery into a census tract identifier. 5 We corresponded with the developers of the COI to ensure that scores were comparable across the time points included in this study. COI scores are generated through compositing 29 individual contemporary indicators of neighborhood features across 3 domains (education, health and environment, and social and economic) for over 72,000 census tracts (Appendix Table A1). The education domain consists of education-related resources and subsequent attainment; the health and environment domain focuses on the health resources and environmental factors that influence health behavior and outcomes; and the social and economic domain focuses on economic and social opportunities and resources, as captured through an economic resources index that factors several different facets of household wealth and income. Each indicator was then weighed and validated, and COI scores were standardized using Z scores.
Key COI data extracted for each patient included quintiles for the national COI score as well as for the 3 domains that compose the COI (health and environment, social and economic, and education). These quintiles were identified as “very low,”“low,”“moderate,”“high,” and “very high.” The very low and low groups were then pooled and compared with the high and very high groups, thus creating a way to compare the bottom 2 quintiles (low group) with the top 2 quintiles (high group). The moderate group was excluded for the purpose of these analyses. All analyses were completed using SAS (Version 9.4; SAS Institute) with an alpha level of 0.05.
Descriptive statistics and 1-way analysis of variance were used to compare continuous variables (age, body mass index, and postoperative strength), and categorical variables (sex and postoperative complications) were compared using the chi-square test or Fisher exact test as appropriate.
Results
Our total patient population was 1154 patients; after eliminating patients in the middle quintile, there were 1027 patients remaining. Overall, 226 (22.0%) were pooled into the low group, while 801 (78.0%) were in the high group. Of these patients, 49.9% (n = 512) identified as men, while 50.1% (n = 515) identified as women. Non-Hispanic White patients comprised 695 of our patients, while 202 patients were Black, 22 were Asian, 20 were Hispanic, and 88 identified as “other.” In the low group, 143 of the 226 (63.3%) patients identified as Black, and 59 of the 801 (7.4%) in the high group identified as Black. Additionally, 5 of 226 (2.2%) Hispanic patients were in the low group versus 15 of 801 (1.9%) in the high group (Table 1). There was a significant difference in race between the low and high groups (P < .001).
There were also differences between the low and high groups in terms of sex (P < .001), age (P < .01), body mass index (P < .001), and body mass index classification (P < .001), with older, Black, and obese patients making up a higher proportion of the low group than the high group (Table 1).
Patient Characteristics a

Data are shown as n (%) unless otherwise indicated.
Statistically significant at alpha = .01.
Insurance utilization data were available for 726 patients; 33.2% of the low group had public insurance (n = 75), while only 5.9% of the high group had public insurance (n = 47). There was also a greater delay in the time from injury to surgery between the low and high groups (98.15 ± 102.65 vs 71.79 ± 101.88 days, respectively; P < .001). The high group was also less likely to have a concomitant meniscal tear (odds ratio, 0.65 [95% CI, 0.44-0.98]; P = .04) (Table 2).
Injury and Treatment Characteristics a

Data are shown as mean ± SD unless otherwise indicated.
Statistically significant at alpha = .01.
Statistically significant at alpha = .05.
Postoperatively, there were no differences in the time to or rates of complications. A significant difference in knee extension-flexion range of motion between the low and high groups at 1 month (108°± 19° vs 113°± 17°, respectively; P = .03) and at 3 months (133°± 9° vs 137°± 9°, respectively; P = .02) was noted, although there was no difference in range of motion at 6-months (137°± 9° vs 141°± 6°, respectively; P = .27). There was also a significant difference in the number of physical therapy visits attended between the 2 groups, with the low group attending a mean of 24.82 ± 10.55 visits versus 37.81 ± 18.07 visits for the high group (P < .001) (Table 2).
When comparing the 2 COI groups, we found significant differences on isokinetic dynamometer testing at 180 deg/s for quadriceps (extension) strength at 3 months (P = .03), 6 months (P < .0001), and 9 months (P = .01) postoperatively (Table 3). Extension strength was again different at 300 deg/s at 6 months (P =.002) but not at 3 months (P = .10). There were no differences between the 2 groups at 180 and 300 deg/s for flexion at 3, 6, and 9 months postoperatively (P > .05 for all).
Postoperative Limb Strength a

Data are shown as mean ± SD (percentage deficit from contralateral limb).
Statistically significant at alpha = .05.
Statistically significant at alpha = .01.
Education Domain
When patients were divided into groups by their education domain, there was a significant difference in time to surgery (P < .001), public insurance utilization (P < .01), and number of physical therapy visits (P < .001).
Social and Economic Domain
When examining the low and high groups as determined by only the social and economic domain, we found a significant difference in time to surgery (P = .001) and number of physical therapy visits (P < .001) (Table 4).
Time to Surgery and Physical Therapy Visits by Domain a
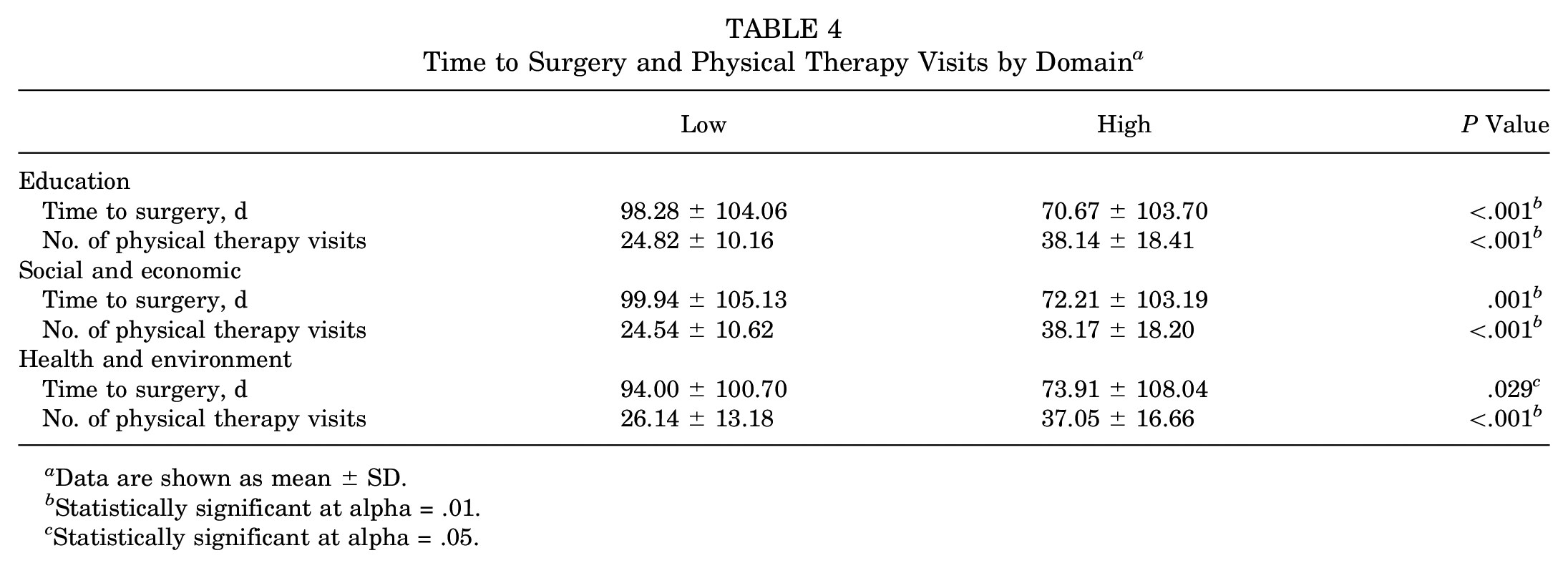
Data are shown as mean ± SD.
Statistically significant at alpha = .01.
Statistically significant at alpha = .05.
Health and Environment Domain
Between the low and high groups as determined by only the health and environment domain, there was a significant difference in time to surgery (P = .03), number of physical therapy visits (P < .001), and range of motion at 1 month (P = .04) and 3 months (P = .01) (Table 4).
Discussion
Current evidence supports a detrimental relationship between a variety of SDOH deficiencies and orthopaedic care deficiencies, including time to ACL reconstruction. 4 However, many of these studies use metrics including Area Deprivation Index scores, race, or proxies such as median household income to draw these conclusions.4,7,12,13,16 A major advantage of the COI over these metrics in characterizing the relationship between SDOH and health outcomes is the direct incorporation of a diverse set of factors into the measure and dividing them across 3 different but equally important domains. As such, the present study supports recent work done by Rosenberg et al 21 (which utilized metropolitan-normalized data) while also expanding the scope to include functional outcomes and comparisons of the lower and upper 2 quintiles of each domain. Additionally, this study opted to be inclusive of patients regardless of the state/type of locale and use the COI's nationally normalized data, thereby increasing the generalizability of the study's results. Composite indices such as the COI may be a valuable tool in not only identifying specific neighborhoods that may benefit from increased socioeconomic support but also identifying patients who may benefit from early interventions.
In this study, significantly longer delays to surgery were noted when comparing the low and high COI groups. This difference persisted on subanalysis by each domain as well, supporting the complex multifactorial nature of these factors on patient health care. Compounding the delay to surgery and the additional resulting burden placed on families in the low group were worse functional outcomes after surgery and lower physical therapy attendance rates. There were noted decreases in quadriceps strength across all time points at both 180 and 300 deg/s for the low group, in line with expectations. 17
The COI domains serve to highlight possible resource accessibility, utilization, and availability gaps. Factors under the education domain, such as adult educational attainment, may contribute to this in the form of a utilization gap due to low health literacy. The number of hazardous waste dump sites and volume of industrial pollutants are accounted for under the health and environment domain, providing biological mechanisms and possible potential barriers to the local availability of physical therapists, thus creating an availability gap. Finally, under the social and economic domain, poverty and public assistance rates are included; as a result, patients in the lower quintiles may have untenable financial barriers to scale to obtain the same quantity of appointments. Additionally, while the COI does take into account the percentage of patients with health insurance under the health and environment domain, it does not consider whether insurance is public or private or the extent of coverage. 19 Therefore, 1 other possible factor not accounted for in the COI domains is noted in our data; the low group had a significantly higher rate of public insurance utilization and therefore may have had more difficulty in accessing physical therapy appointments.
The wide range of potential SDOH that may influence outcomes after ACL reconstruction and surgical delays extends beyond the capabilities of the physician; thus, it is of paramount importance to consider interdisciplinary interventions to address possible gaps. For example, 1 potential component of timely interventions and appropriate recovery is equitable access to athletic trainers in schools, who may more easily connect with patients to address day-to-day recovery needs and provide timely feedback and practical adjustments to rehabilitation protocols. Furthermore, the COI may be useful in the identification of neighborhoods that may benefit from tailored interventions as well. Such neighborhood-level interventions can directly address factors such as lower health literacy and insurance coverage. On a hospital systems level, 1 example of how the COI can be used is through integration into patients’ medical records, so that it may help to identify the patients who would benefit from early social worker integration, additional support in accessing local health resources, or increased attention from schedulers in regard to follow-up appointments.2,9,11 One important component of all these interventions is the involvement of community stakeholders, and the COI may also be used to narrow down the neighborhoods and communities that these stakeholders are a part of.10,22 Furthermore, given that there is scant quantitative research available on the value of community stakeholder involvement, the COI can also provide avenues in identifying areas of interventions that could be used for future research. 8
Previous literature has demonstrated that Black and Hispanic populations and publicly insured patients sustain more meniscal injuries compared with White and privately insured patients.4,21 When comparing the low and high groups in the current study, we also found higher rates of meniscal injuries in the low group. Given that the current literature also suggests longer term sequelae such as osteoarthritis, increased time to return to sports, and reduced patient-reported outcomes with delays in surgery and meniscal injuries, prompt treatment is critical.14,15 This study did not obtain patient-reported outcomes; however, this would be a valuable area for future exploration to continue to characterize the effect of SDOH on ACL reconstruction.
This study has several limitations. First, data were collected retrospectively, leading to inherent selection and reporting biases as well as limitations to account for the presence of unmeasured confounding variables. Of note, insurance status at the time of the procedure was not obtainable for each patient and thus was excluded from analysis where appropriate. Specific to this study, COI data were derived from addresses extracted from the medical record, and thus, patients who did not have a stable place of residence or had multiple places of residence (eg, children of parents who are separated and have joint custody) may have had inaccurate COI data. We also were not able to identify specific causes of delay to surgery, and some patients were excluded during functional outcomes analysis given incomplete data. Additionally, this study was completed at a single tertiary care center in a large urban setting, which may limit its generalizability given unavoidable institutional and regional biases. Some of the variables included in our analysis were not normally distributed, and although we used the nonparametric Kruskal-Wallis test in such cases, we still report analysis of variance results. We made that choice to not lose any information and in light of the fact that analyses of variance are generally known to be robust to violations of normality, especially in larger sample sizes (as in this case). Also, while our patient cohort was typically released to sport at their 9-month postoperative visit, future studies could examine differences in return to sports. Finally, the COI is intrinsically a reflection of neighborhood-level social conditions and therefore does not necessarily reflect an individual child's or family's income, education, wealth, or other resilience factors. In encounters with individual patients, consideration should be given to individualized SDOH; nevertheless, the COI remains a valuable tool to quantify and direct systems-level change.
Conclusion
Access to and quality of care are fundamental health equity issues. The disparities between patients in the lower 2 quintiles and those in the upper 2 quintiles of the COI after ACL reconstruction demonstrate the need for continued attention on SDOH to identify areas of interventions outside of the traditional patient-physician relationship. By using composite indices such as the COI, medical professionals may be better able to identify specific patients who would benefit from early focused interventions.
Footnotes
Appendix
Indicators Included in the Child Opportunity Index by Domain and Subcategory a


|
Table from Noelke et al. 19 ACS, American Community Survey; CRDC, Civil Rights Data Collection, via U.S. Department of Education; EDFacts, U.S. Department of Education Facts Initiative; EPA, Environmental Protection Agency; GS, GreatSchools; NAEP, National Association of Educational Procurement; NAEYC, National Association for the Education of Young Children; NCES CCD, National Center for Education Statistics Common Core of Data; SEDA, Stanford Education Data Archive; USDA, U.S. Department of Agriculture.
Final revision submitted November 7, 2023; accepted November 21, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.J.G. has received education payments from Paladin Technology Solutions and hospitality payments from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Children's Hospital of Philadelphia (ref No. 15-012614).