
Abstract
Background:
Various arthroscopic rotator cuff repair techniques are being used for the treatment of rotator cuff tears with the development of surgical instruments. However, retears after repair are not completely avoidable, and efforts to reduce retears remain a challenge.
Purpose/Hypothesis:
To introduce a new repair technique, the double-row modified Mason-Allen technique with a single knot, and to compare clinical outcomes and retear rates with the single-row modified Mason-Allen technique. It was hypothesized that this new technique would have a better clinical outcome and significantly lower retear rate than the single-row modified Mason-Allen technique.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A total of 110 patients with small- to medium-sized (<1.5 cm) full-thickness supraspinatus tears were enrolled into 2 groups, with 65 patients receiving the single-row modified Mason-Allen technique (group A) and 45 patients receiving the double-row modified Mason-Allen technique with a single knot (group B). The clinical and functional outcomes were evaluated using the American Shoulder and Elbow Surgeons (ASES) score; Disabilities of the Arm, Shoulder and Hand (DASH) score; and visual analog scale (VAS) for pain and satisfaction scores. All patients enrolled in this study were monitored for a minimum of 24 months. Magnetic resonance imaging was performed to analyze the integrity of tendons and retear at 6 months after surgery.
Results:
No statistically significant differences between the 2 groups were found regarding the VAS for pain, ASES, and DASH scores. However, retear was found in 9 patients (13.8%) in group A and 1 patient (2.2%) in group B. The difference in the retear rate was statistically significant between the 2 groups (P = .037).
Conclusion:
A significantly lower retear rate and comparable clinical outcomes were seen after the double-row modified Mason-Allen repair technique with a single knot when compared with the single-row modified Mason-Allen technique. Based on these findings, the double-row modified Mason-Allen repair technique with a single knot can be considered a surgical treatment option that can provide sufficient stability in small- to medium-sized supraspinatus tears.
Keywords
Rotator cuff tears are one of the most common diseases of the shoulder joint, often accompanied by shoulder joint pain and dysfunction.13,34 Various double-row repair techniques and transosseous-equivalent techniques have been reported for the treatment of rotator cuff tears.20,24,25,27 However, previous studies have reported that the retear rate after rotator cuff repair is 17% to 47%, despite advances in arthroscopic repair techniques.4,14,16,30 Lee et al 18 reported that retears were observed in 24.4% of 102 patients with small- to medium-sized rotator cuff tears in a magnetic resonance imaging (MRI) follow-up 6 months after surgery. In a study by Longo et al, 19 retears were reported in approximately 12.5% of small- to medium-sized rotator cuff tears and up to 37% of large-sized rotator cuff tears. Although low in frequency, retears after the repair of small-sized rotator cuff tears are not completely avoidable. Therefore, reduction of the retear rate after rotator cuff repair remains a challenge.
Rotator cuff repair techniques are broadly divided into single-row and double-row repairs. Some studies have reported the double-row repair to be biomechanically superior to the single-row repair, as it increases the footprint coverage and contact surface.2,23 Furthermore, Brady et al 1 reported that patients who underwent surgery using a single-row repair method had only 47.3% of the original footprint covered; however, the original footprint was completely covered (100%) in all the patients who underwent double-row repair, with clinically better results. In addition, the knotless repair technique was introduced as one of the methods for successful rotator cuff repair. This technique has strengths that minimize problems that occur because of knot-tying, and several satisfactory clinical results have been reported.3,12,21,26 The knotless repair technique reduces the occurrence of undue tension in the suture-tendon interface of the medial row 31 and provides the advantage of reducing tissue necrosis or strangulation that may occur locally in the knot-tying area.26,33
In the present study, we describe a new repair technique that we call the “double-row modified Mason-Allen technique with a single knot.” It combines the advantages of the double-row technique, which widens the contact surface based on the previously reported modified Mason-Allen technique, 29 and minimizes knot-tying with a single knot, which reduces knot-induced problems such as undue tension and strangulation. Our aim was to compare the differences in clinical outcomes and retear rates after repair of small- to medium-sized rotator cuff tears between this new technique and the previously reported single-row modified Mason-Allen technique. 29 We hypothesized that better clinical outcomes and significantly lower retear rates would be seen after the double-row modified Mason-Allen technique with a single knot.
Methods
Patients and Study Design
From March 2018 to November 2020, 152 patients with small- to medium-sized (<1.5 cm) full-thickness rotator cuff tears were treated at our institution. We included patients with at least 2 years of follow-up. Excluded from this study were patients with (1) a partial-thickness tear, (2) a combined subscapularis tendon tear or biceps lesion requiring concomitant repair, (3) labral pathology amenable to surgical repair, (4) degenerative arthritis of the glenohumeral joint, (5) symptomatic arthritis of the acromioclavicular joint, and (6) a history of previous surgery in the involved shoulder or associated cervical lesions. Of the 152 patients, 22 (14.5%) were lost to follow-up before 2 years postoperatively or refused to participate in this study. Ultimately, we included 65 of 74 consecutive patients who underwent the single-row modified Mason-Allen technique from March 2018 to September 2019 (group A) and 45 of 56 consecutive patients who underwent the double-row modified Mason-Allen technique with a single knot (group B). Images of the repair techniques are shown in Figure 1. The protocol for this study received institutional review board approval, and written consent was obtained from all included patients.

Arthroscopic rotator cuff repair with the (A) single-row modified Mason-Allen technique and (B) double-row modified Mason-Allen technique with a single knot. Schematic diagrams depicting the appearance after repair are on the left, and arthroscopic views showing the appearance before (top) and after (bottom) repair are on the right.
Surgical Technique of Double-Row Modified Mason-Allen Repair With a Single Knot
All operations were performed by a single surgeon (Y.S.J.) at a single institution. Patients were placed in the lateral decubitus position to perform tendon repair. After placing the interscalene nerve blocks and administering general anesthesia, we performed a complete inspection of the glenohumeral joint via standard posterior viewing and anterior working portals. Then we moved the arthroscope into the subacromial space. A lateral portal was created at the midpoint of the torn rotator cuff tendon. A shaver and radiofrequency device were used for arthroscopic debridement for all supraspinatus tears. Using a tendon grasper, we evaluated the tissue quality of the rotator cuff tendon for arthroscopic reparability and identified the mobility of the tear apex in the medial-to-lateral and anterior-to-posterior directions. The medial-to-lateral length and anterior-to-posterior width of the tear were measured using a calibrated probe. Acromioplasty was conducted when osteophytes were detected under the acromion or the acromion exhibited a hook shape.
Double-row modified Mason-Allen repair with a single knot uses double-row suture anchors and involves only 1 knot that is present in the horizontal mattress suture. After decortication of the rotator cuff footprint area using a high-speed bur, the anchor (Healicoil PK; Smith + Nephew) with double-loaded FiberWire suture was placed into the medial margin of the footprint. Next, a pair of suture limbs was passed with a suture passer in a horizontal mattress stitch at the anterior and posterior edges of the rotator cuff tear. The other pair of suture limbs was passed in a vertical mattress stitch at approximately 2 to 3 mm more medial to the horizontal mattress stitches (Figure 2).

The procedure after insertion of the medial anchor in the double-row modified Mason-Allen technique with a single knot. The medial anchor with a double-loaded FiberWire suture was placed into the medial margin of the footprint. First, a pair of suture limbs (striped pattern) was passed in the articular-to-bursal direction by a shuttle relay through the anterior and posterior edges of the rotator cuff tear for horizontal mattress stitches. Next, the other pair of suture limbs (plain pattern) was passed just medial to the horizontal strand situated at the bursal side of the rotator cuff for vertical mattress stitches.
After passage of all the medial row sutures, the horizontal mattress stitches were tied using an arthroscopic knot pusher. Then, the vertical mattress stitches of the same color were connected to 1 lateral anchor (Footprint Ultra PK; Smith + Nephew) and fixed by the knotless technique without undue tension. The lateral anchor was placed into the lateral row of the greater tuberosity (Figure 3). In this novel technique, 2 anchors were used to cover the entire surface of the medial-to-lateral footprint, unlike the single-row modified Mason-Allen repair method. This new technique has the effect of increasing the contact surface and reducing the undue tension by using 2 anchors.

The procedure of inserting a lateral anchor in the double-row modified Mason-Allen technique with a single knot. First, the horizontal mattress stitches (striped pattern) were tied using a knot pusher. Next, the vertical mattress stitches (plain pattern) were passed through the lateral anchor and secured using a knotless technique. The lateral fixation point was placed into the lateral row of the greater tuberosity to maximize the contact surface.
Postoperative Management
Postoperative rehabilitation was the same in all patients. Patients wore shoulder abduction braces for 4 weeks after surgery, and pendulum exercises started 2 weeks after surgery. After 4 weeks postoperatively, the brace was removed, and passive range of motion (ROM) was performed as tolerated to prevent shoulder stiffness. Active-assisted ROM was allowed 6 weeks after surgery, and resisted ROM was allowed 3 months after surgery.
Clinical and Radiological Evaluation
Functional outcomes were assessed using the visual analog scale (VAS) for pain; American Shoulder and Elbow Surgeons (ASES) score; and Disabilities of the Arm, Shoulder and Hand (DASH) score. To evaluate functional outcomes, we used an electronic patient-reported outcome measure system (Proscore). The patients were instructed to complete the questionnaires at our clinic at the 1-, 2-, 3-, 6-, 12-, and 24-month follow-ups.
Radiological examinations for tendon integrity were confirmed by MRI at 6 months postoperatively in all enrolled patients. In addition, retears were checked again through ultrasonography 1 year after surgery. MRI and ultrasound findings were interpreted by a single musculoskeletal radiologist who was not involved in this study. A failure of rotator cuff repair was defined as the presence of a major discontinuity of the repaired tendon or complete detachment from the footprint of the greater tuberosity.
Statistical Analysis
Data were reported as means ± standard deviations and ranges. Using SPSS software (Version 18.0; IBM), we utilized paired and Student t tests to analyze continuous variables and the chi-square test to analyze dichotomous variables, with 95% CI. Statistical significance was indicated by P < .05.
Results
Of the 65 patients who underwent repair using the single-row modified Mason-Allen technique (group A), 27 were male patients and 38 were female patients, their mean age was 62.1 ± 8.5 years old (range, 40-78 years old), and the mean follow-up period was 27.3 ± 2.3 months (range, 25-31 months). In the 45 patients who underwent the double-row modified Mason-Allen repair technique with a single knot (group B), 20 were male patients and 25 were female patients, their mean age was 60.8 ± 9.3 years old (range, 41-78 years old), and the mean follow-up period was 26.5 ± 2.1 months (range, 24-30 months). No statistical differences were found in the characteristics between the 2 groups in terms of sex, age, body mass index, symptom duration, history of trauma, operation time, or mean follow-up period (Table 1).
Comparison of Patient Characteristics Between the Study Groups a

Data are expressed as mean ± SD unless otherwise specified. Group A, patients who underwent single-row modified Mason-Allen repair; group B, patients who underwent double-row modified Mason-Allen repair with a single knot. BMI, body mass index.
At the final follow-up, the mean VAS pain score improved significantly in both groups (Table 2). In addition, the mean ASES score significantly increased and the DASH score significantly decreased in both groups (P < .001 for both). There were no significant differences between the 2 groups regarding VAS pain, ASES, or DASH scores.
Comparison of Clinical Outcomes Between the Study Groups a
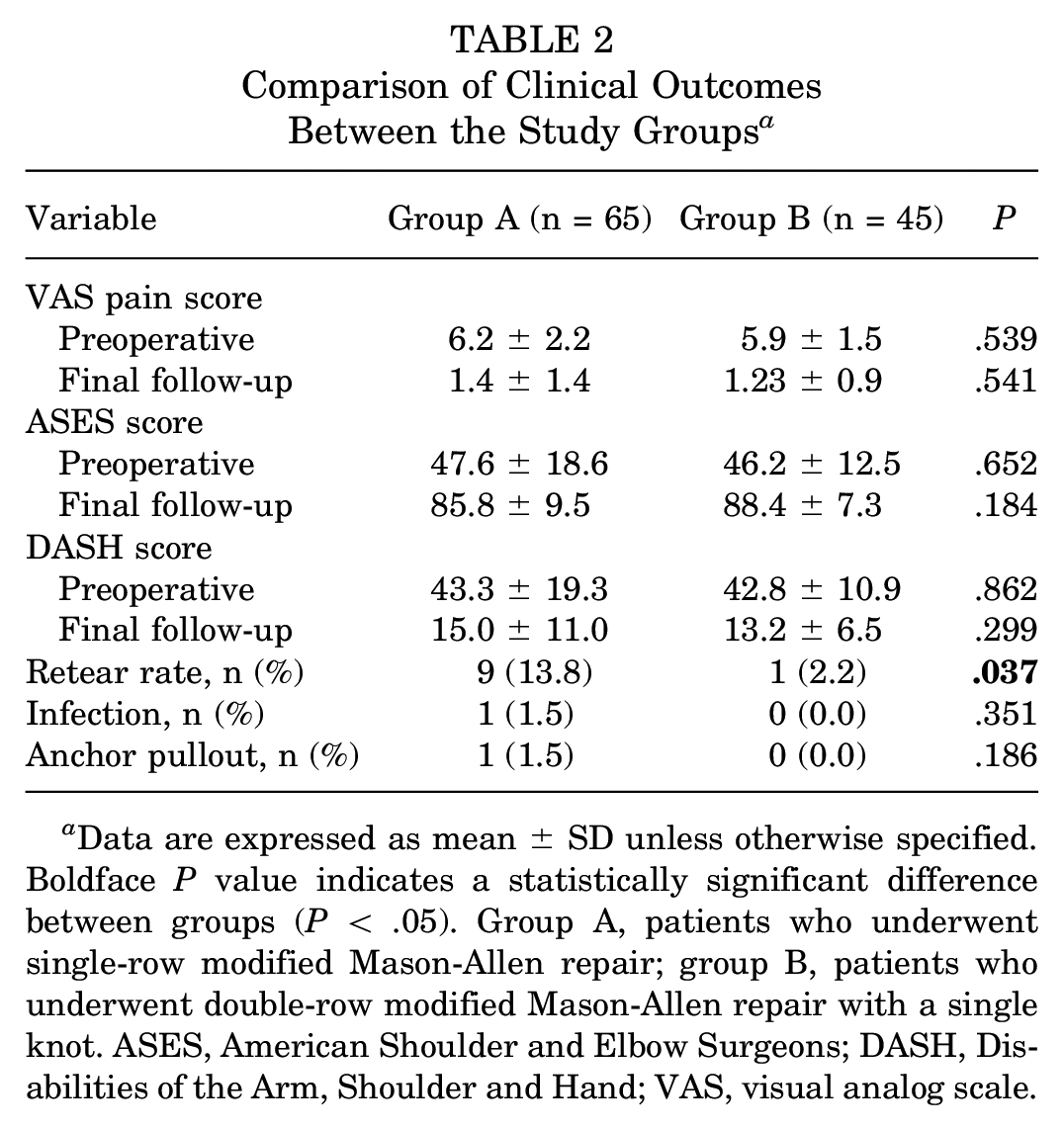
Data are expressed as mean ± SD unless otherwise specified. Boldface P value indicates a statistically significant difference between groups (P < .05). Group A, patients who underwent single-row modified Mason-Allen repair; group B, patients who underwent double-row modified Mason-Allen repair with a single knot. ASES, American Shoulder and Elbow Surgeons; DASH, Disabilities of the Arm, Shoulder and Hand; VAS, visual analog scale.
The difference in the retear rate was statistically significant between the 2 groups (P = .037). A postoperative rotator cuff retear was found in 9 patients (13.8%) in group A and 1 patient (2.2%) in group B. In group A, 1 patient (1.5%) experienced a postoperative infection and 1 patient (1.5%) experienced anchor pullout, whereas there were no other complications, such as infections or catastrophic failures, related to suture anchors in group B.
Discussion
In the present study, patients in both groups showed satisfactory improvement in terms of clinical outcomes after surgery for at least 24 months. However, the retear rate in group B (double-row modified Mason-Allen repair with a single knot) was significantly lower (P = .037) compared with that in group A (single-row modified Mason-Allen repair). In addition, complications of infection and anchor pullout occurred in 1 patient each in group A; however, neither occurred in group B.
Maintaining appropriate tension is imperative for reducing the retear rate of the repaired tendons and facilitating the healing process. The Mason-Allen technique introduced by Gerber et al 9 reduces the bone-to-tendon gap and is a superior repair technique in terms of optimal tensile load, tensile strength, and tissue holding power to other techniques.8,9,21 The modified Mason-Allen technique adds a ripstop suture to create a horizontal loop, thereby reducing the risk of tissue cutout that occurs when using a simple suture or the mattress stitch pattern for repair, and can appropriately distribute the load in the repaired tendon.7,21,32 Based on these advantages, our study was conducted using the modified Mason-Allen technique in both groups to enhance tensile strength and load distribution in the repaired tendon and lower the risk of tissue cutout.
Making the contact surface of the repaired tendon with the original anatomic footprint as wide as possible is also important to maintain the appropriate tension of the repaired tendon. Several studies have reported similar functional outcomes in small- to medium-sized tears when comparing the single-row repair technique and double-row repair technique.17,22 However, numerous studies have reported that double-row repair can more strongly maintain the biomechanical stability of the repaired tendon than single-row repair. In a systematic review, Hein et al 11 reported a retear rate of 19% with single-row repair and 4% with double-row repair for rotator cuff tears <1 cm, and retear rates were 33% for single-row and 10% for double-row in the 1- to 3-cm rotator cuff tears. Cummins et al 5 reported that the double-row repair technique makes the tendon-to-bone contact surface wider than the single-row repair technique and provides satisfactory results through a theoretically better healing process. Therefore, double-row repair, which fixes relatively healthy medial tendon tissue to the footprint using medial anchors, not only increases the contact surface but also maintains tissue retention by appropriately distributing the load in the repaired tendon. 5 The new technique introduced in the present study might increase the contact surface by combining the modified Mason-Allen technique and the double-row repair technique and obtain better results than the conventional single-row modified Mason-Allen technique in terms of retear rates.
The all-knotless repair technique has been attracting attention as a method to reduce operation time and impingement that may occur because of knot-tying.6,10,21 Burns et al 3 compared the operation time of 15 and 22 patients in knot-tying and knotless groups, respectively, using the suture bridge repair technique and reported that the mean of the knot-tying group was 121 minutes while that of the knotless group was 79.5 minutes, and the difference was statistically significant. Park et al 26 reported that while there was no statistically significant difference in the occurrence of acromion erosion after single-row repair using 4 knots and suture bridge repair using minimal knots, better clinical outcomes were observed in the group using minimal knots as evaluated by the VAS score, ASES score, and ROM after surgery. In addition, the knotless repair technique can reduce the possibility of medial rotator cuff failure by decreasing undue tension at the suture-tendon interface of the medial row 31 and tissue necrosis that may occur locally during knot-tying or strangulation that may occur because of overtension in the medial row.28,33 In the present study, repair was performed using only a single knot, unlike the 3 knots of the existing single-row modified Mason-Allen technique. In our study, no significant difference was observed in the clinical outcome between the 2 groups; however, the retear rate was significantly lower in the double-row modified Mason-Allen technique group, wherein repair was conducted with minimal knots.
Limitations
There are some limitations to this study. First, this study involved consecutive groups of patients and was not a randomized controlled trial. Second, because of the inclusion of a relatively small number of patients, this study was underpowered to detect differences in clinical outcomes. Third, all surgeries were performed at a single center by a single surgeon and conducted by limiting the rotator cuff tear size to <1.5 cm. Therefore, it may be difficult to apply our technique to all cases of rotator cuff repair. Fourth, the musculoskeletal radiologist, who was unaware of this study and not involved in it, provided interpretations of the images; however, true blinding could not be achieved because the number of anchors would be clearly visible on MRI. Last, the MRI scan performed to confirm the presence of retear was 6 months after surgery, not at the time of the final follow-up. However, according to a previous study published by Koh et al, 15 the structural condition of the rotator cuff tendon was maintained without significant changes at 6 and 19 months after repair as observed via MRI.
Conclusion
The double-row modified Mason-Allen technique with a single knot, a new repair technique based on the modified Mason-Allen technique in combination with the double-row technique and minimal knots, showed a significantly lower retear rate and comparable clinical outcomes compared with the single-row modified Mason-Allen technique. Based on this, the double-row modified Mason-Allen technique with a single knot can be considered as a surgical treatment option that can provide sufficient stability in small- to medium-sized rotator cuff tears.
Footnotes
Final revision submitted August 30, 2023; accepted October 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by a research grant from Inha University. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. IRB approval was granted from Inha University Hospital (ref No. INHAUH 2021-03-047).