
Abstract
Background:
A novel hybrid transtibial (HTT) approach to femoral tunnel drilling in anterior cruciate ligament reconstruction (ACLR) has been developed that circumvents the need for knee hyperflexion and orients the graft in the most anatomic position without sacrificing the tunnel length or aperture.
Hypothesis:
Patients who underwent ACLR utilizing the HTT technique would achieve excellent patient-reported outcome scores and experience low rates of graft failure and reoperations.
Study Design:
Case series; Level of evidence, 4.
Methods:
Patients who underwent primary ACLR at a single institution between 2005 and 2020 were retrospectively reviewed. Patients treated with the HTT, anteromedial portal (AMP), and transtibial (TT) approaches were matched based on age, sex, and body mass index ±3 kg/m2. Demographic and surgical data as well as femoral tunnel angle measurements on anteroposterior and lateral radiographs were collected for the 3 groups. However, clinical outcomes were only reported for the HTT group because of concerns of graft heterogeneity.
Results:
A total of 170 patients (median age, 26.5 years [interquartile range (IQR), 18.0-35.0 years]) who underwent ACLR using the HTT approach were included. The median coronal- and sagittal-plane femoral tunnel angles were 47° (IQR, 42°-53°) and 40° (IQR, 34°-46°), respectively. The sagittal-plane femoral tunnel angles in the HTT group were significantly more horizontal compared with those in the TT group (P < .0001), whereas the coronal-plane femoral tunnel angles in the HTT group were found to be significantly more vertical compared with those in the AMP group (P = .001) and more horizontal compared with those in the TT group (P < .0001). The graft failure and reoperation rates in the HTT group at a minimum 2-year follow-up were 1.8% (3/170) and 4.7% (8/170), respectively. The complication rate was 6.5% (11/170), with the most common complication being subjective stiffness in 7 patients. The median Lysholm score was 89.5 (IQR, 79.0-98.0); the median International Knee Documentation Committee score was 83.9 (IQR, 65.5-90.8); and the median Veterans RAND 12-Item Health Survey physical and mental component summary scores were 55.0 (IQR, 52.6-55.9) and 56.2 (IQR, 49.1-59.3), respectively.
Conclusion:
ACLR using the HTT technique was associated with low graft retear and revision surgery rates and good patient-reported outcome scores at medium-term follow-up and demonstrated femoral tunnel obliquity on postoperative radiographs that correlated with optimal parameters previously reported in cadaveric and biomechanical studies.
Keywords
An anterior cruciate ligament (ACL) tear remains one of the most common orthopaedic injuries, occurring in an estimated 120,000 patients each year. 16 Arthroscopic-assisted ACL reconstruction (ACLR) remains the gold-standard treatment to restore long-term knee joint stability.8,12,20 The rate of ACLR has increased more than 12-fold over the past 20 years, and despite the successful nature of ACLR, there remains significant controversy over the optimal surgical technique that offers the best long-term outcomes. 1 The influence of anatomic graft placement during ACLR has been investigated by numerous studies, with results demonstrating that both biomechanical and clinical outcomes are optimized when grafts are placed in the center of the native femoral and tibial insertion sites.3,4,7,14,21,26,30,35
Traditionally, the femoral tunnel has been prepared via the transtibial (TT) technique; however, the resulting constraint on the femoral drill guide may prevent anatomic femoral tunnel placement and increases the likelihood of a vertically oriented graft postoperatively.5,28,35,36 A modified TT technique has been described for a more anatomic graft position; however, this comes at the cost of sacrificing the femoral anatomic footprint with regard to the tibial tunnel length/aperture, is more technically demanding, and increases the risk of tibial plateau fractures.13,28,37,39
Alternatively, the anteromedial portal (AMP) approach in which the femoral tunnel guide is inserted through the medial portal eliminates tibial tunnel constraints and allows the surgeon greater accuracy in placing the graft in an anatomic position. However, a different set of challenges is faced with the AMP approach such as the need for knee hyperflexion, the risk of injuring medial femoral condylar articular cartilage, and/or posterior wall blowout.4,10,17 Furthermore, the femoral tunnel length is typically shorter and is more horizontal in orientation compared to that with the TT technique and thus subjects the graft to greater stress loads because of increased acuity of the graft bending angle.24-26,32
To leverage the strengths of both the TT and AMP techniques while mitigating the drawbacks inherent to both, a novel hybrid TT (HTT) approach to femoral tunnel drilling was developed in which a flexible TT guide wire is introduced through the tibial tunnel and captured by an over-the-top guide from the medial portal, circumventing the need for knee hyperflexion and to orient the graft in the most anatomic position without sacrificing the tunnel length or aperture.18,27,32
The purpose of this study was to evaluate the medium-term clinical outcomes of patients who underwent ACLR using the HTT technique for femoral tunnel drilling. We hypothesized that patients who underwent ACLR utilizing the HTT technique would achieve excellent patient-reported outcome (PRO) scores and experience low rates of graft failure and reoperations.
Methods
After obtaining institutional review board approval for the study protocol, we reviewed a registry consisting of all patients with ACL tears who underwent primary ACLR at a single center between 2005 and 2020. Inclusion criteria were patients aged ≥13 years at the time of index ACLR, isolated ACL tears with or without concomitant meniscal/chondral abnormalities, a minimum 2-year follow-up, and surgical records indicating that the HTT technique was used. Patients with open physes, prior surgical interventions on the ipsilateral knee, chondral abnormalities treated with high tibial osteotomy/distal femoral osteotomy, treatment for other concurrent ligamentous abnormalities, and preoperative knee radiographs demonstrating Kellgren-Lawrence grade ≥2 19 indicative of mild to severe osteoarthritis were excluded. After a review, we identified 195 patients who underwent primary ACLR using the HTT technique.
The same registry and inclusion criteria were utilized to search for patients who underwent ACLR with the TT or AMP technique, except the surgical records indicating that the TT or AMP femoral tunnel drilling approach was required for inclusion. Propensity score matching was utilized to control for differences in patient demographic characteristics for the 3 groups (HTT vs AMP vs TT), with patients matched based on age, sex, and body mass index ±3 kg/m2. After propensity score matching, 170 patients in the HTT group, 162 patients in the AMP group, and 163 patients in the TT group were included in the study.
Data Collection
Baseline injury data included side affected, history of ACLR in the contralateral knee, athlete level and preoperative sport leading to the injury if applicable, mechanism of injury (defined as ultra-low velocity [activities of daily living], low velocity [sports injuries], or high velocity [motor vehicle accident]), concurrent meniscal or articular cartilage abnormalities, and Kellgren-Lawrence osteoarthritis grade on preoperative radiographs. Surgical data that were reported were femoral tunnel drilling technique (including AMP and TT), femoral fixation technique, tibial fixation technique, graft type (autograft, autograft augmented with allograft, or allograft), and choice of graft tissue. Postoperative plain radiographs taken at the most recent clinical follow-up were used to measure the femoral tunnel angle in anteroposterior and lateral views using methods described by Sohn et al 34 (Figure 1).

Postoperative (A) anteroposterior and (B) lateral radiographs in a patient who underwent anterior cruciate ligament reconstruction using the hybrid transtibial technique, demonstrating femoral tunnel angle measurements (dotted lines).
After obtaining operative data and radiographic measurements for all 3 groups, preliminary statistical analyses were performed. However, the surgeons who performed the majority of the AMP and TT techniques utilized mainly hamstring tendon autografts, and the surgeons who performed the HTT technique utilized predominantly bone–patellar tendon–bone autografts. Given the significant heterogeneity in graft selection, we determined that the influence of such a confounding variable would complicate the interpretation of clinical outcomes based solely on the femoral tunnel drilling technique. Therefore, the study protocol was amended, and the postoperative outcomes for only the HTT group were collected, as this was the primary focus of the study.
HTT Surgical Technique
The HTT technique utilized in our patient cohort was consistent with that described by Trofa et al. 37 The initial starting point for the tibial tunnel was determined at 30 mm below the joint line and 15 mm medial from the medial edge of the tibial tubercle. At this junction, a rigid guide wire was inserted, aimed toward the center region of the tibial insertion site. The tunnel was subsequently created by overreaming the wire with a 10-mm cannulated reamer. With the knee positioned at 90° of flexion, a 7 mm–offset ACL femoral drill guide (DanaMed) was introduced via the standard medial portal and positioned to ensure that its slot entrance sat above the tibial tunnel opening (Figure 2A). A flexible nitinol guide pin enclosed in a custom sheath (DanaMed) was introduced and advanced through the tibial tunnel, ensuring its alignment with the open slot of the drill guide (Figure 2B). Care was taken to position the wire’s tip near the center of the femoral ACL footprint, and the drill guide was advanced to the lateral wall of the condylar notch (Figure 2C). After confirming optimal positioning of the wire, the guide wire was drilled through the distal femur (Figure 2D). Subsequently, the sheath encompassing the guide wire was removed, allowing the drill guide to be easily extracted via the medial portal (Figure 2E), leaving behind an anatomically positioned transtibial guide wire.
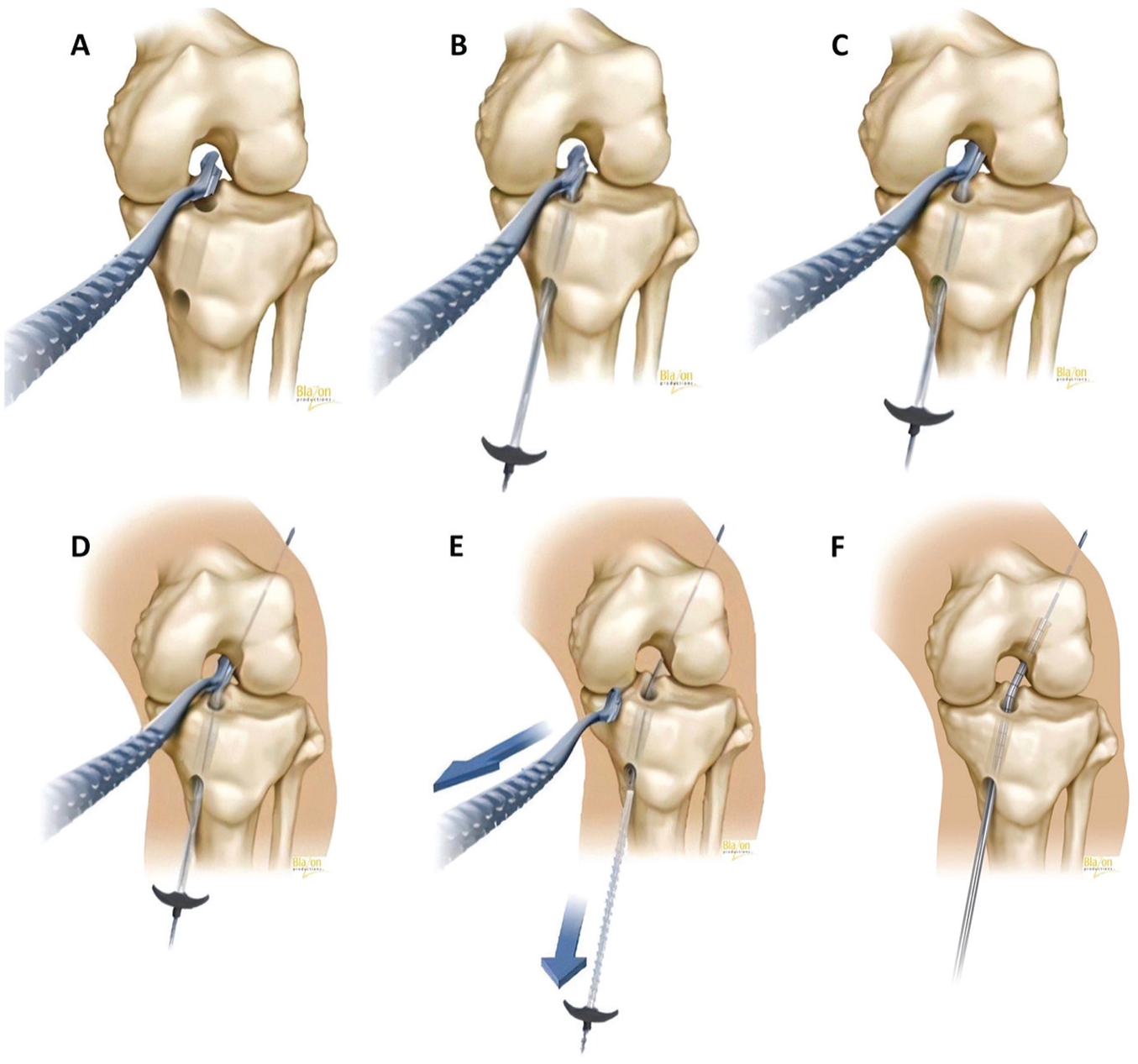
Drilling the tibial and femoral tunnels with the hybrid transtibial technique. (A) A 7 mm–offset anterior cruciate ligament (ACL) femoral drill guide was inserted via the medial portal. (B) A flexible guide pin enclosed in a custom sheath was advanced through the tibial tunnel. (C) The wire’s tip was positioned near the center of the femoral ACL footprint. (D) Drilling of the guide wire through the distal femur. (E) Removal of the custom sheath. (F) Drilling of the femoral tunnel using a 10-mm flexible reamer over the wire.
Once the pin was placed via the tibial tunnel, our technique involved viewing from the anteromedial portal to confirm the appropriateness of the pin location. This approach provides us with a satisfactory view to ensure the pin’s proper placement without necessitating additional procedures (notchplasty or the use of a 70° scope). To create the femoral tunnel, a 10-mm flexible VersiTomic reamer (Stryker) was utilized and passed over the wire (Figure 2F). A typical depth of 35 to 40 mm was obtained.
Outcome Evaluation
The primary outcomes that were evaluated were any graft failure, defined as revision ACLR or the confirmation of a graft tear on magnetic resonance imaging, and reoperations to the ipsilateral knee, documented on patients’ medical charts or determined via answers to questionnaires administered to patients via telephone or email. Postoperative outcomes including complications, reoperations, and mechanisms of the reinjury were collected from patients in the HTT group with a minimum 2-year follow-up, alongside the following PRO scores: Lysholm, International Knee Documentation Committee (IKDC), Veterans RAND 12-Item Health Survey (VR-12; Mental component summary and Physical component summary), Knee injury and Osteoarthritis Outcome Score (KOOS; Pain, Symptoms, Activities of daily living [ADL], Sports and recreation [Sports], and Quality of life [QoL] subscales), and Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC; Pain, Stiffness, and Function subscales). Patients provided informed consent prior to answering the PRO questionarres.
Statistical Analysis
All data underwent descriptive statistical analysis using SAS (Version 9.4; SAS Institute). Continuous variables with normally distributed data were reported as the mean ± standard deviation, and nonparametric continuous variables were reported as the median and interquartile range (IQR). Categorical variables were reported as frequencies and proportions. Bivariate analysis of the HTT, AMP, and TT groups was performed using the Wald chi-square test to analyze categorical variables, and the t test was used to compare the difference in mean values for continuous variables. P≤ .05 was considered statistically significant.
Results
In the HTT group, the median age at the time of ACLR was 26.5 years (IQR, 18.0-35.0 years), the median body mass index was 25.1 kg/m2 (IQR, 22.5-28.0 kg/m2), 91 of 170 patients (53.5%) were male, and 16 of 170 patients (9.4%) had undergone previous ACLR to their contralateral knee. The mean clinical follow-up was 60.62 ± 19.44 months (Table 1).
Demographic Characteristics of Patients a

Data are reported as median (interquartile range) or n (%) unless otherwise indicated. Dashes denote variables that have been omitted, as the focus of the study was the clinical outcomes of the HTT group. ACLR, anterior cruciate ligament reconstruction; AMP, anteromedial portal; HTT, hybrid transtibial; TT, transtibial.
Comparative analyses were not conducted for variables that were used for propensity score matching.
At the time of ACLR, 56 of 170 patients (32.9%) in the HTT group had a concurrent meniscal injury, and 4 of 170 (2.4%) had a concurrent articular cartilage injury. Data collected from operative notes revealed that the most common method of femoral and tibial fixation of the ACL graft was an interference screw (162/170 [95.3%]) (Table 2).
Surgical Characteristics and Findings a
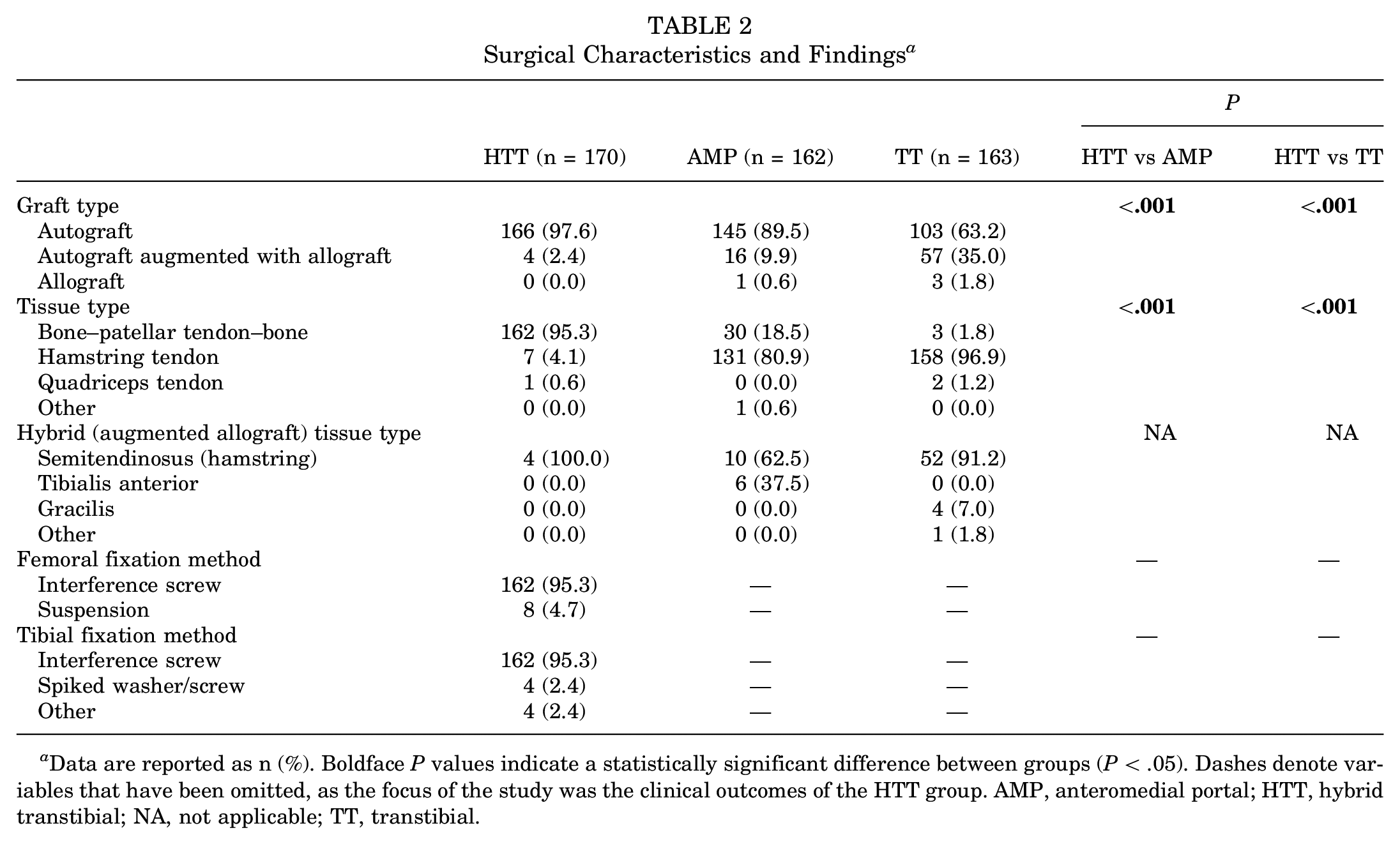
Data are reported as n (%). Boldface P values indicate a statistically significant difference between groups (P < .05). Dashes denote variables that have been omitted, as the focus of the study was the clinical outcomes of the HTT group. AMP, anteromedial portal; HTT, hybrid transtibial; NA, not applicable; TT, transtibial.
The most common graft of choice for ACLR was a bone–patellar tendon–bone autograft (162/170 [95.3%]) in the HTT group. A hamstring tendon autograft was used in 7 of the 170 patients (4.1%), with 4 of 7 (57.1%) augmented with a semitendinosus allograft. The median sagittal- and coronal-plane femoral tunnel angles measured on anteroposterior and lateral radiographs were 40° (IQR, 34°-46°) and 47° (IQR, 42°-53°), respectively. The sagittal-plane femoral tunnel angles in the HTT group were significantly more horizontal compared to those in the TT group (P < .0001), whereas the coronal-plane femoral tunnel angles in the HTT group were found to be significantly more vertical in comparison to those in the AMP group (P = .001) and more horizontal in comparison to those in the TT group (P < .0001) (Table 3).
Femoral Tunnel Angle Measurements a

Data are reported as median (interquartile range). Boldface P values indicate a statistically significant difference between groups (P < .05). AMP, anteromedial portal; HTT, hybrid transtibial; TT, transtibial.
At a minimum 2-year follow-up, the graft failure and reoperation rates in the HTT group were 1.8% (3/170) and 4.7% (8/170), respectively; 25.0% of the reoperations (2/8) were revision ACLR, 50.0% (4/8) were meniscal surgery, and 25.0% (2/8) were lysis of adhesions. The complication rate was 6.5% (11/170), with the most common complication being subjective stiffness in 63.6% (7/11) of patients. Of note, 21 patients were not able to be contacted via telephone to obtain the postoperative outcomes or PRO scores beyond the 2-year office follow-up. The median Lysholm, IKDC, VR-12, KOOS, and WOMAC scores are reported in Table 4.
Postoperative Outcomes of HTT Group a
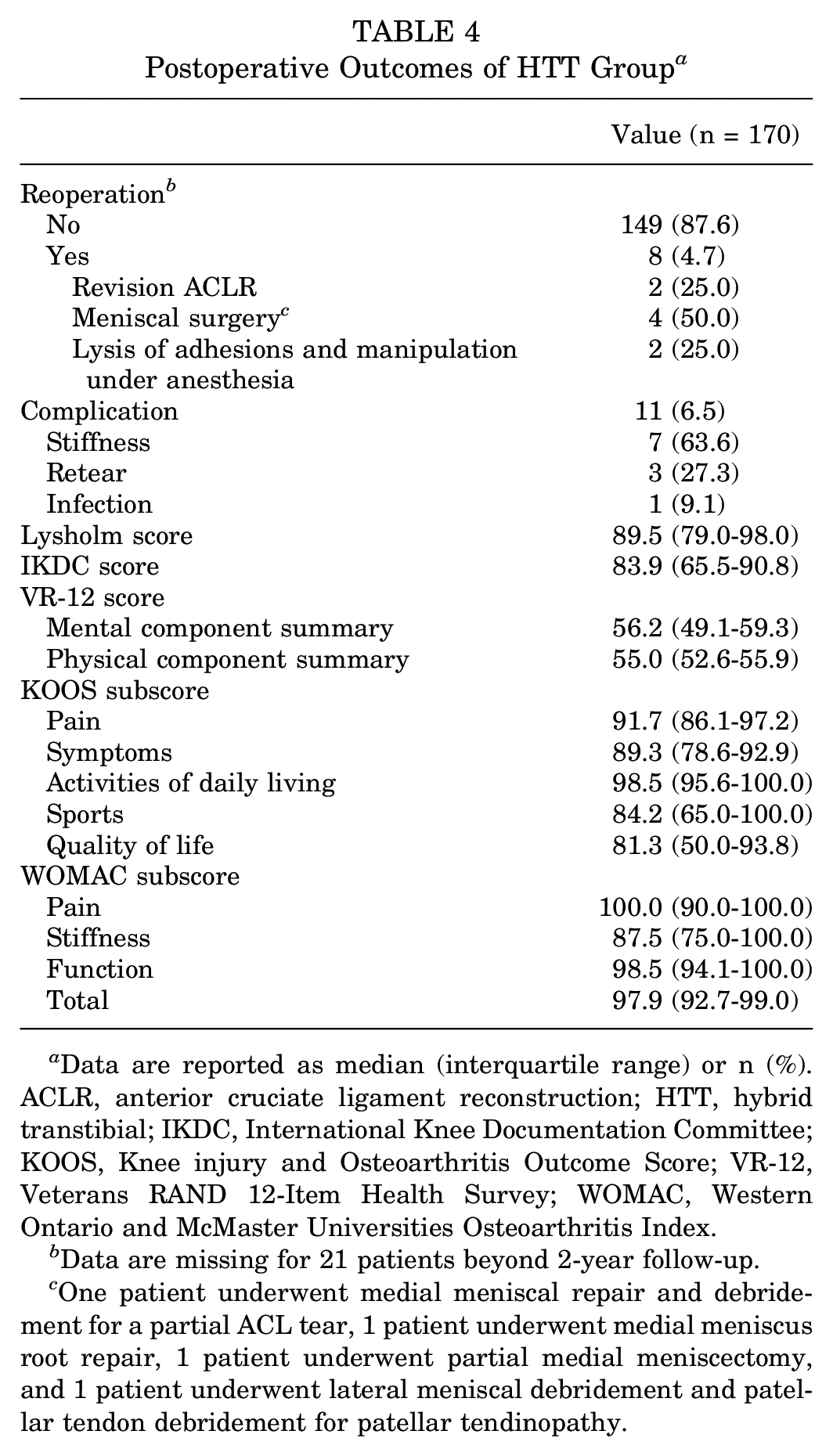
Data are reported as median (interquartile range) or n (%). ACLR, anterior cruciate ligament reconstruction; HTT, hybrid transtibial; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; VR-12, Veterans RAND 12-Item Health Survey; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Data are missing for 21 patients beyond 2-year follow-up.
One patient underwent medial meniscal repair and debridement for a partial ACL tear, 1 patient underwent medial meniscus root repair, 1 patient underwent partial medial meniscectomy, and 1 patient underwent lateral meniscal debridement and patellar tendon debridement for patellar tendinopathy.
Discussion
The principal findings of this large case series of ACLR using the HTT femoral tunnel drilling technique were that 1.8% of patients experienced graft failure and the all-cause reoperation rate was 4.7% at a minimum follow-up of 2 years. Previous studies have directly compared the outcomes after ACLR using the TT versus AMP technique; however, there is no clear consensus as to which technique provides the best outcome postoperatively.15,22,23 Recent literature has provided supporting evidence highlighting the importance of replicating the native footprint of the ACL via anatomic positioning of the femoral tunnel, thus popularizing the AMP technique over the conventional TT approach.22,38,40 However, despite the improved anatomic placement of the ACL graft when using the AMP technique, 33 a unique set of technical challenges associated with this approach has emerged such as the need to hyperflex the knee, a shorter tunnel length, the risk of injuring medial femoral condylar articular cartilage, and/or posterior wall blowout.4,10,17
To combine the technical ease of the TT approach while still maintaining the anatomic placement of the ACL graft, the HTT technique was introduced. 18 The utility of the HTT approach was confirmed in a cadaveric model, 32 and further support for its efficacy was obtained from a subsequent prospective randomized controlled trial. 37 These findings validate the novel technique and suggest that it effectively combines the advantages of the TT and AMP approaches. Trofa et al 37 conducted a prospective randomized controlled trial assessing the efficacy of the HTT technique compared to the traditional TT and AMP approaches in 30 patients. Using 3-dimensional computed tomography of the operative knee at 6 weeks postoperatively, they found that the HTT technique achieved anatomically accurate femoral aperture positions, similar to the AMP approach, while producing longer femoral tunnels with less angulation. These authors hypothesized that their findings may potentially reduce graft strain and mismatch. A finite element analysis study published in 2022 by Saltzman et al 32 evaluated the femoral tunnel length, graft bending angle, and peak graft stress using the HTT, TT, and AMP techniques. They confirmed the true hybrid nature of the HTT technique with regard to the 3 primary outcomes and provided further evidence to suggest that ACLR using the HTT approach may be a successful alternative while ameliorating the drawbacks of both the TT and AMP approaches.
Despite emerging evidence to suggest the technical and biomechanical advantages of utilizing the HTT approach during ACLR, there is a paucity of medium-term clinical evidence and outcomes. A systematic review by Loucas et al 22 comparing clinical outcomes after ACLR using the TT and AMP techniques reported revision rates of 6.2% and 5.9%, respectively. Furthermore, these authors found the overall complication rate to be 2.9% for the TT group and 3.3% for the AMP group. The complication rate found in the current study was higher (6.5%); however, the comparison of complication rates may be limited by the criteria with which an outcome was determined to be a complication by each study included in the Loucas et al 22 review. It should be noted that subjective symptoms such as stiffness as described by the patients were also included in our definition of a complication. In contrast, our study reported a revision ACLR rate of 1.2% in patients who underwent index surgery using the HTT technique.
A 2021 biomechanical study reported that a drilling angle of 45° in both the coronal and sagittal planes for the femoral tunnel during ACLR was optimal to provide the lowest peak stress on the ACL graft while simultaneously providing the lowest peak stress and maximum strain at the femoral and tibial tunnel entrances, respectively. 11 The methodology of evaluating femoral tunnel obliquity in ACLR using plain radiographs in both the coronal and sagittal planes as described by Sohn et al 34 was replicated in our case series. We reported a median coronal-plane femoral tunnel angle of 47° (IQR, 42°-53°) and sagittal-plane femoral tunnel angle of 40° (IQR, 34°-46°) when the HTT technique was used. In contrast, Sohn et al 34 reported mean coronal- and sagittal-plane femoral tunnel angles of 56.4° and 49.4°, respectively, for the TT technique and 39.4° and 50.9°, respectively, for the AMP technique. In summary, utilizing the HTT technique allowed for femoral tunnel obliquity in both planes to be closer to the ideal 45° angle for graft longevity.
The PRO scores obtained in the current study demonstrated good results, with no specific score or subscore indicative of a poor outcome. The median Lysholm score was 89.5 (IQR, 79.0-98.0), which is considered a “good” rating (corresponding to scores of 84-94). The median IKDC score was 83.9 (IQR, 65.5-90.8), which is comparable to the mean IKDC scores reported by Cheecharern, 9 with 79.03 ± 19.21 in patients who returned to sports after ACLR and, when stratified by return-to-sports status, 94.00 ± 10.75 in patients who returned versus 71.90 ± 18.34 in those who did not. For the KOOS, the 2 lowest subscores in our study were for the KOOS-Sports (median, 84.2 [IQR, 65.0-100.0]) and KOOS-QoL (median, 81.3 [IQR, 50.0-93.8]), which was also the case in previous studies that surveyed patients after ACLR.2,31 Similarly, the WOMAC-Stiffness had the lowest WOMAC subscore (median, 87.5 [IQR, 75.0-100.0]), which was also similar to that in previous studies.2,6 Roos and Toksvig-Larsen 29 conducted a validation and comparative study of KOOS and WOMAC scores in patients after total knee replacement and found that the KOOS-ADL and WOMAC-Function subscores were equivalent. Although our case series specifically focused on patients who underwent ACLR, we observed that the median KOOS-ADL and WOMAC-Function subscores were 98.5 (IQR, 95.6-100.0) and 98.5 (IQR, 94.1-100.0), respectively, thereby supporting the conclusions drawn by Roos and Toksvig-Larsen. 29
Limitations
This study is not without limitations, primarily that the retrospective review of patients may introduce biases inherent to such methodology. Additionally, there are limitations due to missing demographic information, despite a thorough retrospective chart review. A further limitation is in relation to the femoral tunnel lengths; although we generally perceived that the femoral tunnel was longer because of its more vertical orientation compared to that with the AMP technique, precise data on tunnel lengths were not available through a retrospective review, as they were not routinely documented in the operative notes at our institution. Furthermore, as this study was a case series without a comparative cohort, the clinical outcomes of patients who underwent ACLR using the HTT approach could not be directly compared with those of the TT or AMP group. Lastly, because PRO scores were not collected preoperatively or at routine clinical follow-up visits, we were unable to report changes in PRO scores at different follow-up time points. While PRO scores were obtained at a minimum of 2 years after the index procedure, it is worth noting that data from 21 patients were not available beyond the 2-year mark. Additionally, the absence of anterior laxity measurements and graft imaging limited a more comprehensive insight into the clinical outcomes. Nevertheless, with a 87.6% follow-up rate, the results of this study can be associated with outcomes at medium-term follow-up. Future studies may benefit by conducting a 3-arm prospective randomized controlled trial evaluating outcomes after the HTT, TT, and AMP techniques to determine if the HTT approach is the superior alternative, retaining the advantages while mitigating the challenges inherent to employing either the TT or AMP approach during ACLR.
Conclusion
ACLR performed using the HTT technique exhibited favorable PRO scores and clinical outcomes, including low rates of graft retears and revision surgery, at medium-term follow-up. Additionally, postoperative radiographs revealed femoral tunnel obliquity consistent with optimal parameters identified in previous cadaveric and biomechanical studies. However, to establish HTT femoral tunnel drilling as the gold-standard technique for ACLR, it is crucial to conduct long-term prospective randomized trials.
Footnotes
Final revision submitted September 28, 2023; accepted October 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.P.T. has received research support from Arthrex and education payments from Arthrex and Smith + Nephew. D.P.P. has received education payments from Peerless Surgical and consulting fees from Zimmer Biomet. B.M.S. has received research support from Arthrex, education payments from Arthrex and Smith + Nephew, consulting fees from Bioventus, and publishing royalties from Nova Science Publishers. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Atrium Health (ref No. 11-20-27E).