
Abstract
Background:
Treatment of primary patellar dislocation (PPD) with chondral or osteochondral injury without patellar stabilization in the adolescent population may lead to unsatisfactory outcomes. Surgical treatment, with or without traditional medial patellofemoral ligament (MPFL) reconstruction, is a topic of interest.
Purpose:
To compare postoperative outcomes and rates of patellar redislocation and return to the operating room (OR) in patients who sustained a PPD with chondral or osteochondral injury and were surgically treated with versus without suture tape augmentation repair of the MPFL.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Adolescents who sustained a PPD with chondral or osteochondral injury confirmed via magnetic resonance imaging (MRI) and who were treated by a single surgeon between January 2009 and November 2020 were retrospectively reviewed. Patients were grouped into those who underwent chondral or osteochondral treatment with suture tape augmentation repair of the MPFL (ST group; n = 20) and those who did not have suture tape augmentation or repair (no-ST group; n = 20; 11 patients within the no-ST group did undergo medial imbrication). Demographic characteristics, postoperative knee range of motion, pre- and postoperative radiographic measurements, and preoperative MRI parameters were recorded, and minimum 2-year patient-reported outcomes were collected. Data were compared between the ST and no-ST groups.
Results:
The mean patient age was 15.02 years (range, 12.64-17.61 years) in the ST group and 14.18 years (range, 10.56-16.38 years) in the no-ST group, with a mean follow-up of 3.63 years (range, 2.01-6.11 years) in the ST group and 4.98 years (range, 2.23-9.03 years) in the no-ST group. Significantly more patients returned to the OR in the no-ST group compared with the ST group (7 [35%] vs 0 [0%]; P = .008). Further patellar stabilization with an MPFL allograft (n = 5) and manipulation under anesthesia (n = 2) were reasons for returning to the OR. There were no redislocation events in the ST group.
Conclusion:
Treating PPDs with chondral or osteochondral injury using suture tape to augment and repair the MPFL has promising advantages over not repairing it—including lower rates of postoperative patellar instability and return to the OR.
Keywords
Patellar dislocations are a common injury in the pediatric and adolescent population. Treatment of primary patellar dislocations (PPDs) is often nonoperative—including activity modification, bracing, and physical therapy. Children and adolescents who have sustained a PPD treated nonoperatively have reported redislocation or subluxation rates as high as 71%.8,17,24,27 Patients with concomitant patella alta, trochlear dysplasia, or skeletal immaturity at the initial dislocation may be at even greater risk for recurrent instability, with rates reported as high as 88%. 11 Even if recurrent instability does not ensue, these patients may have subsequent patellar tilt, abnormal patellar tracking, and resulting patellofemoral pain syndrome and potential for early osteoarthritis. 7 Furthermore, patient compliance with bracing and physical therapy can be challenging in this young age group, putting them at greater risk for redislocation.
An alternative treatment to nonoperative management after PPD is medial patellofemoral ligament (MPFL) repair. In a meta-analysis by Le et al, 15 the mean redislocation rate for patients who sustained a PPD treated with MPFL repair was 7%. Other studies have reported the redislocation rate as high as 17% to 46% after MPFL repair.2,5 The increasing evidence of continued patellar instability after MPFL repair or nonoperative management of PPDs requires improved treatment modalities in the acute setting to prevent long-term adverse consequences.
Current treatment for recurrent patellar instability includes autograft or allograft reconstruction of the MPFL. The superior outcomes with ligamentous reconstruction21,22,23,25 and high dislocation rates with nonoperative management have sparked interest regarding the treatment of PPDs. 26 Of patients with patellar instability, 5% to 50% will have osteochondral damage resulting in loose bodies.3,14,20,24,29 One of the initial indications for surgical intervention in the setting of an acute PPD is the presence of a chondral or osteochondral defect with or without a loose body. 6 However, the treatment beyond the chondral or osteochondral defect repair is still controversial.
Recent literature has identified a recurrent instability rate of 61% in children who sustained a PPD with retained loose bodies and who underwent management for their chondral or osteochondral defect with or without MPFL repair. 26 In these patients undergoing surgical intervention, the argument can be made to perform an MPFL allograft reconstruction at the time of chondral or osteochondral treatment or perform patellar stabilization in a staged, 2-step fashion. However, others have suggested that the MPFL can be repaired with augmentation using high-strength suture, which produces biomechanics and joint kinematics similar to those of the traditional MPFL allograft or autograft reconstruction. 19 We postulated that this could serve as an intermezzo between an MPFL repair and MPFL reconstruction, negating the need for an autograft or allograft.
The purpose of this study was to evaluate postoperative outcomes and rates of patellar redislocation and return to the operating room (OR) for children and adolescents who sustained a PPD with chondral or osteochondral injury and who were surgically treated either with or without suture tape augmentation MPFL repair using high-strength ultrahigh molecular weight polyethylene (UHMWPE) suture. The proposed null hypothesis was that there would be no difference in postoperative instability rates, rates of return to the OR, or patient-reported outcomes between patients who underwent treatment with versus without suture tape augmentation repair of the MPFL.
Methods
An institutional review board–approved retrospective comparative cohort study was conducted on patients who underwent chondral or osteochondral treatment with or without augmentation repair using suture tape for PPDs between January 2009 and November 2020. Patients were identified using patellar dislocation and patellar ligament sprain International Classification of Diseases-10th Revision codes S83.0 and S83.1 for the initial diagnosis of PPDs. Patients were identified as having PPDs in their initial presentation through their documented history. Patellar dislocations were confirmed via magnetic resonance imaging (MRI). These records were reviewed to identify patients who sustained chondral or osteochondral lesions with or without a loose body at the time of initial dislocation. Patients who underwent suture tape augmentation repair of the MPFL were identified via Current Procedural Terminology codes 27420 and 27422. Patients aged 10 to 18 years with at least a 2-year follow-up evaluation were included in the study. Patients with a history of ipsilateral knee surgery or those who did not sustain a chondral or osteochondral injury at the time of initial patellar dislocation were excluded. Participants provided informed consent for all surgical procedures.
Surgical Procedures and Postoperative Rehabilitation
All procedures were performed by the same fellowship-trained pediatric sports medicine orthopaedic surgeon (J.A.S.). Treatment of the chondral or osteochondral defect was based on its location and size and the surgeon's discretion. Treatments included osteochondral fixation utilizing bioabsorbable screws and/or darts, marrow stimulation, or chondroplasty with or without loose body removal. The indication to address the osteochondral fracture with fixation was if the fragment was at least 10 × 10 mm. Fragments found to be smaller or not amenable to fixation were removed, and the defect was treated with microfracture or chondroplasty. The decision to perform either the medial imbrication or lateral retinacular lengthening in patients was based on the location of their cartilage pathology, which determined the surgical approach.
Patients undergoing MPFL suture tape augmentation repair were treated with a 2-mm braided UHMWPE suture tape (FiberTape; Arthrex Inc). The approach was medial patella–based for the MPFL suture tape augmentation repair; no midsubstance or femoral-sided MPFL repair was performed. The medial cortex of the patella was prepared and decorticated with a rongeur. The suture tape was affixed onto the patella between the middle and superior third using an absorbable 3.5-mm suture anchor (SwiveLock; Arthrex Inc), and the suture tape was shuttled through layer 2 of the medial aspect of the knee deep to the gracilis and semitendinosus using a 1- to 2-cm incision centered at the region of the medial epicondyle with the knee at 30° of flexion. The suture tape was affixed to the anatomic femoral insertion with an absorbable 4.75-mm suture anchor (SwiveLock) under fluoroscopic guidance using the technique described by Schöttle et al. 28 The patella was held with its lateral border aligned to the lateral aspect of the femoral trochlea, and a curved hemostat was placed under the tape before final fixation to prevent overtightening of the suture. 31 The knee was taken through a range of motion (ROM) to confirm appropriate patellar tracking before sutures were tied and cut (Figure 1).
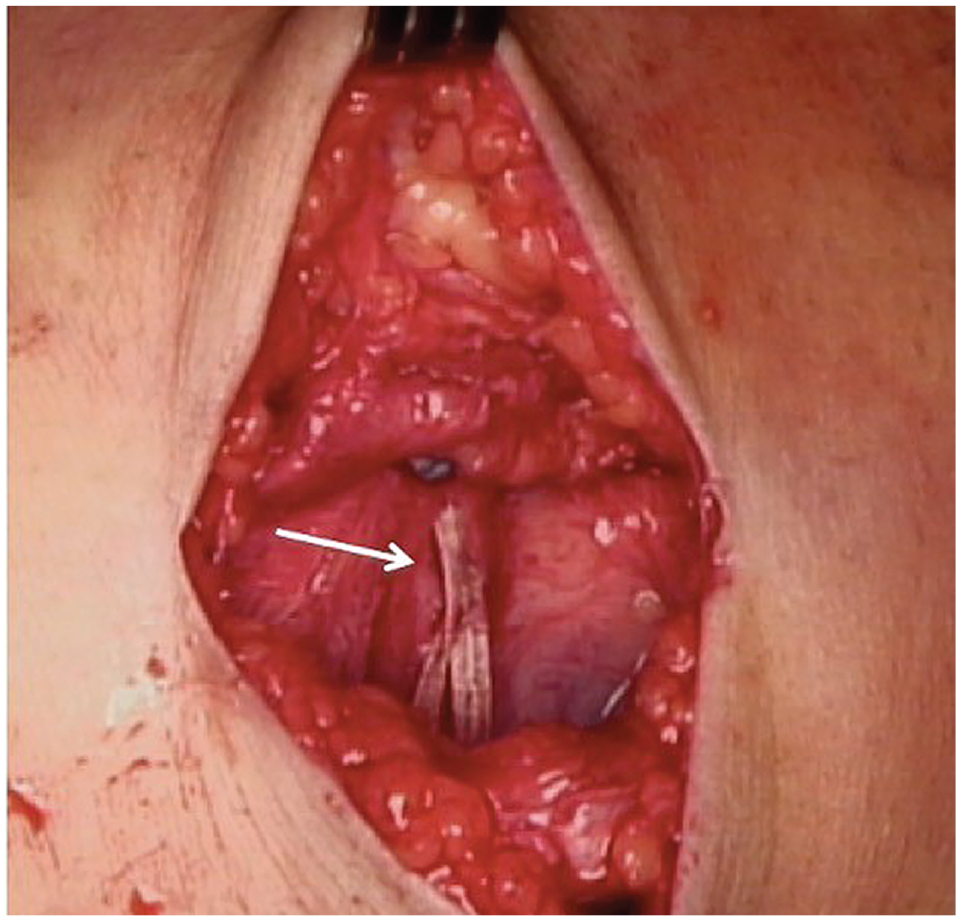
A high-strength ultrahigh molecular weight polyethylene suture (arrow) implanted as an internal brace.
All surgeries were performed as same-day procedures, with patients discharged on the day of surgery. All patients were prescribed postoperative-guided physical therapy with immediate passive and active-assisted ROM exercises at home. Postoperative weightbearing status depended on the type of procedure performed. Patients who underwent isolated loose body removal or patellar chondroplasty were allowed to bear weight as tolerated in the immediate postoperative period. Patients who underwent MPFL suture tape augmentation repair used a locked ROM knee brace (Breg T Scope; Breg Inc) and were allowed toe-touch protected weightbearing for 4 weeks, removing the brace for physical therapy and ROM exercises. Patients who underwent osteochondral fixation or marrow simulation of a patellar lesion were allowed toe-touch protected weightbearing for 4 to 6 weeks, and patients treated for a condylar lesion of the weightbearing articular surface were nonweightbearing for 4 to 6 weeks. These patients used a locked ROM knee brace (Breg T Scope), removing the brace for physical therapy and ROM exercises. At weeks 4 to 6, patients began unlocking their brace 0° to 30° and progressed to weightbearing as tolerated as quadriceps control returned. The primary goal was to unlock the brace fully at 6 to 8 weeks postoperatively and discontinue the brace when there was a return of quadriceps control and full terminal knee extension, with no lag with supine straight-leg raise. A patella-stabilizing brace was used until 8 to 12 weeks postoperatively then as needed for activity and return to sports at 6 months.
Data Collection and Outcome Measurements
Descriptive data—including date of birth, sex, insurance status, location of osteochondral lesion, procedure performed, and laterality of the injured knee—were recorded.
All patients underwent preoperative MRI and pre- and postoperative plain film radiographs. Postoperative radiographs were taken at the 3-month postoperative visit. Pre- and postoperative imaging was evaluated using Synapse PACS (Fujifilm) and Joints (Medstrat Inc) software. Tibial tubercle-trochlear groove (TT-TG) distance and trochlear morphology represented by lateral trochlear inclination were measured on MRI. The pre- and postoperative sulcus angle, congruence angle, lateral translation, lateral patellofemoral angle, and Caton-Deschamps index were measured on the plain radiographs. All procedures were performed by a single fellowship-trained pediatric sports medicine orthopaedic surgeon (J.A.S.).
Postoperatively, all patients were monitored for patellar instability events. Final contact with the patient was considered the final follow-up, whether by telephone or in-person clinic visit. Validated patient-reported outcome measures—including the Pediatric International Knee Documentation Committee, 12 Lysholm Knee Scoring System, 18 Tegner activity scale, 32 and Kujala anterior knee pain scale 13 —were completed at the final follow-up evaluation. The International Knee Documentation Committee questionnaire was used if the patient was ≥18 years old at the 2-year follow-up. 10 The outcome scores were collected by a research coordinator and an orthopaedic surgery resident physician (B.R.G. and K.Z.K.), blinded to the treatment group. In addition, all patients were asked whether they had experienced any recurrent dislocation and/or subluxation events or required a subsequent stabilization operation.
Statistical Analysis
The study patients were divided into those who underwent chondral or osteochondral treatment with suture tape augmentation repair of the MPFL (ST group) and those who underwent chondral or osteochondral treatment without suture tape augmentation or repair (no-ST group). Characteristics and outcomes between the 2 cohorts were compared utilizing analysis of variance for continuous dependent variables that satisfied the normality and homogeneity assumptions. The Mann-Whitney U test was utilized for variables that violated 1 or both assumptions. Categorical variables were compared between cohorts using the Fisher exact or chi-square test. Data were analyzed utilizing SPSS Version 27 (IBM Corp). The alpha level was set at .05 to declare significance.
Results
A total of 40 patients were included in the study—20 patients each in the ST and no-ST groups. All patients had sustained 1 PPD and did not have another instability episode before surgical intervention. The patient and surgery characteristics of the study group are shown in Table 1. The mean patient age was 15.02 years (range, 12.64-17.61 years) in the ST group and 14.18 years (range, 10.56-16.38 years) in the no-ST group. All patients in the ST group were skeletally mature at the time of surgery, while 10 patients were skeletally mature and 10 were skeletally immature in the no-ST group. Chondral or osteochondral injury occurred at the medial facet of the patella, lateral femoral condyle, or lateral trochlea, with some patients sustaining injuries to multiple sites. Within the no-ST group, 11 patients underwent medial imbrication. Four of the 11 patients also underwent lateral retinacular lengthening. Significantly more patients underwent medial imbrication in the ST group compared with the no-ST group (20 vs 11 patients, respectively; P = .002). In addition, there was a significant group difference in the mean follow-up time, which was 3.63 years (range, 2.01-6.11 years) in the ST group and 4.98 years (range, 2.23-9.03 years) in the no-ST group (P = .028).
Patient and Surgery Characteristics by Study Group a

Data are reported as number of knees unless otherwise indicated. Bold P values indicate statistically significant differences between groups (P < .05). No-ST group, patients who did not have suture tape augmentation or repair; MPFL, medial patellofemoral ligament; ST group, patients who underwent chondral or osteochondral treatment with suture tape augmentation repair of the MPFL.
Mann-Whitney U test.
Some knees had multiple areas of osteochondral fracture. Some patients underwent multiple procedures on the same knee.
There was a statistically significant difference in patients who returned to the OR between the 2 cohorts (P = .008). In the no-ST group, 7 patients (35%) returned to the OR for additional intervention: 5 patients for additional stabilization procedures due to recurrent instability and 2 patients for manipulation under anesthesia (MUA) due to postoperative arthrofibrosis. No patients in the ST group returned to the OR.
Details regarding the 5 patients who returned to the OR for additional stabilization procedures are shown in Table 2. Four of the patients were skeletally immature. The time from the initial injury to the OR was 17 to 129 days. One patient who was skeletally mature (patient 1) also underwent chondroplasty for peripheral cartilage fraying for the lateral femoral condyle and medial patellar lesions that had previously undergone fixation. One patient (patient 2) had 2 subsequent returns to the OR after the index surgery for a chondral lesion on the patella—the first being chondroplasty of the medial patellar facet (18 × 18 mm for a chondral defect) and concomitant chondrocyte harvest, with an additional planned return to the OR for open implantation of autologous cultured chondrocytes on a porcine collagen membrane for a 20 × 15–mm full-thickness chondral defect, MPFL reconstruction with an allograft, and lateral retinacular lengthening.
Patients Who Returned to the Operating Room for Additional Stabilization Procedures a

MACI, autologous cultured chondrocytes on porcine collagen membrane; MPFL, medial patellofemoral ligament.
This patient returned to the operating room 2 times. The first procedure was chondroplasty for chondral defects in the medial patellar facet and chondrocyte harvesting. The second procedure included open implantation of autologous cultured chondrocytes on a porcine collagen membrane (MACI implant), MPFL allograft reconstruction, realignment of extensor mechanism, and lateral retinacular lengthening.
Of the 2 patients with arthrofibrosis, the first patient had removal of loose body, lateral release, internal fixation of the osteochondral fracture, and medial imbrication performed 22 days from their initial injury. In addition, the second patient had left knee open treatment of patella dislocation with internal fixation of osteochondral fracture of the patella and was treated 14 days after the initial injury. The second patient did not have a medial imbrication or lateral retinacular release. These patients had MUAs performed within 81 and 42 days after their initial surgery, respectively. We did note that the second patient had delayed physical therapy due to insurance issues. The ROM of both patients improved after MUA, and they were compliant with physical therapy. At a minimum 2 years postoperatively, no instability episodes were reported in patients in the ST group. This was statistically significant compared with the 5 patients in the no-ST group who continued to have instability and returned to the OR for an MPFL reconstruction (P = .047). Of the patients who had fixation of their osteochondral lesions, none needed to return to the OR for revisions related to osteochondral fracture healing, symptomatic, or failed implants.
Table 3 compares MRI and radiographic measurements between cohorts. No statistically significant difference was found for the TT-TG distance; lateral trochlear inclination; and pre- and postoperative sulcus angle, congruence angle, lateral translation, lateral patellofemoral angle, or Caton-Dechamps index between the 2 cohorts. All patients regained full knee ROM.
MRI and Radiographic Measurements by Group a

Data are reported as mean (range). MRI, magnetic resonance imaging; MPFL, medial patellofemoral ligament; no-ST group, patients who did not have suture tape augmentation or repair; Postop, postoperative; Preop, preoperative; ST group, patients who underwent chondral or osteochondral treatment with suture tape augmentation repair of the MPFL; TT-TG, tibial tubercle–trochlear groove.
Mann-Whitney U test.
No significant differences were found in patient-reported outcome scores according to the study group (Table 4). Patients who underwent MPFL allograft reconstruction (n = 5) due to continued patellar instability were considered to have failed initial treatment and were not included in the postoperative patient-reported outcome scoring.
Patient-reported Outcomes and Return to the Operating Room by Group a
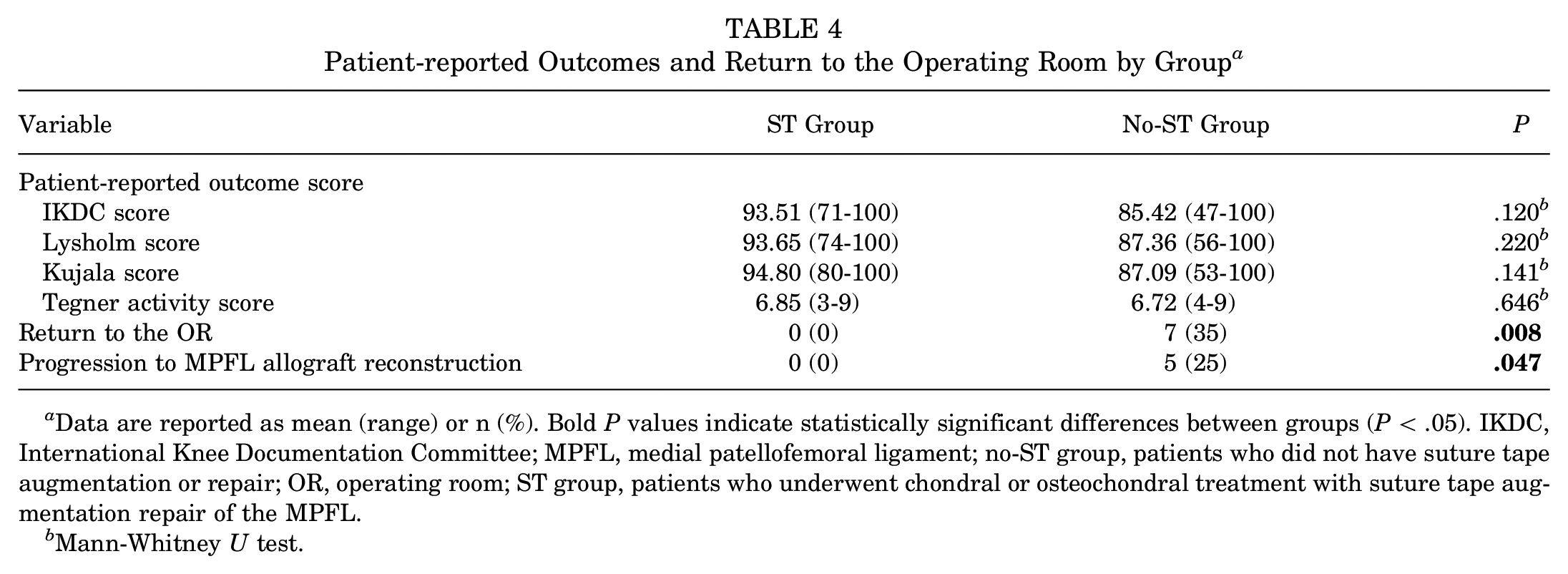
Data are reported as mean (range) or n (%). Bold P values indicate statistically significant differences between groups (P < .05). IKDC, International Knee Documentation Committee; MPFL, medial patellofemoral ligament; no-ST group, patients who did not have suture tape augmentation or repair; OR, operating room; ST group, patients who underwent chondral or osteochondral treatment with suture tape augmentation repair of the MPFL.
Mann-Whitney U test.
Discussion
We treated PPDs with chondral and osteochondral injury using suture tape to augment and repair the MPFL. During our study, suture tape augmented repair of other ligaments came into vogue. Viens et al 34 demonstrated that suture tape augmentation repair of the anterior talofibular ligament resulted in a construct that was more biomechanically similar to native tissue. The benefits of a suture tape augmented repair more closely mimicking native tissue while also sparing the patient from additional risks associated with autograft or allograft reconstruction options—including donor site morbidity, infection, and costs, respectively—were compelling. The practices and management of the primary surgeon evolved over time to adapt some of these philosophies and techniques beginning in March 2014.
The results of this study indicate that suture tape augmentation repair of the MPFL in PPDs with concomitant chondral or osteochondral injury produces improved results with respect to lower rates of return to the OR. The addition of the suture tape to an MPFL repair has reduced the postoperative recurrent instability rate from 61% seen in a study by Pedowitz et al 26 to 0% in the present study. As 40% of the patients in the Pedowitz et al 26 study required further stabilization within 5 years of their first dislocation, they strongly recommended reconstruction with an MPFL allograft at the time of initial primary dislocation. However, the results of the present study indicate that a primary MPFL allograft reconstruction may not be required. Our preferred treatment for first-time patellar dislocations with associated osteochondral fractures is primary repair with suture tape augmentation. However, there remains a role for primary MPFL reconstruction using an autograft or an allograft for patients with recurrent patellar instability, typically >2 episodes of recurrent dislocation.
Despite the excellent results seen with MPFL allograft reconstruction, complication rates upwards of 26.1% have been reported. 30 Complications may include allogenic tendon reaction, graft laxity, inappropriate graft tensioning, abnormal patellar tracking, and recurrent dislocations. Although autografts are an option for MPFL reconstruction, the literature has demonstrated a slightly increased failure rate with an autograft when compared with an allograft. 1 Using synthetic, readily available suture tape is advantageous to negate tendon reaction and graft laxity. While suture tape can still lead to over- or undertightening, placing a hemostat under the tape while tightening can help prevent this. All the patients who received suture tape augmentation repair of the MPFL in the present study were also skeletally mature at the time of surgery, as the suture tape was not utilized if there was growth remaining for concerns of overconstraint with growth. In addition, at the time of this writing, MPFL allografts typically cost US$1058, which is significantly more than suture tape, whereas the suture tape augmentation repair kit alone at our institution is approximately US$600. 9 The suture tape augmentation repair can be performed at the index procedure to address the chondral or osteochondral injury that would limit the progression to recurrent patellar instability and prevent a return to the OR in this vulnerable pediatric and adolescent population. This may lead to a better quality of life and more favorable long-term outcomes. Furthermore, if the suture tape augmentation repair fails as an index procedure, an MPFL allograft or autograft can still be performed later.
In a biomechanical comparison model, Mehl et al 19 found that suture tape augmentation of the MPFL produced similar contact pressures and joint kinematics compared with MPFL reconstruction using a tendon graft in all testing conditions. Their study 19 determined that normal patellofemoral kinematics were restored when the suture tape was pretensioned to 2 N. Another study comparing suture tape with knotless anchors to the semitendinosus tendon autograft with soft tissue anchors found that reconstructions with suture were stronger than those with autografts. 33
A prospective study by Lee et al 16 examined the clinical results of patients treated with either suture tape or standard autografts for primary MPFL reconstruction in patients with patellar instability. Their study focused on a patient population with a mean age of 21 to 22 years who sustained >1 patellar dislocation. In both cohorts, not a single patient had an episode of instability in their 2-year follow-up period, with comparable 2-year patient-reported outcomes between those undergoing suture tape versus autograft reconstruction. 16 This finding suggests that suture tape may be useful for first-time dislocations and patients who have already progressed to recurrent patellar instability.
Xu et al 35 performed a retrospective review of 17 patients who sustained a patellar dislocation treated with MPFL reconstruction using suture tape augmentation. Their results indicated that reconstruction with MPFL suture tape significantly improved lateral patellofemoral angle, patellar tilt angle, and congruence angle. In their cohort of 17 patients, with a mean age of 22.1 years, only 1 patient went on to sustain an episode of patellar instability. While their population was slightly older than the present study cohort and their patients did not sustain chondral or osteochondral injuries, the results are similar, indicating the use of suture tape to provide patellar stabilization results in a success rate 35 of 94.1% to 100%. Their study was inconclusive as to the relative contributions of reconstruction versus augmentation.
One could argue that the patellar instability rate was higher in the no-ST group because of the MRI and radiographic parameters of each patient's native anatomy. In a retrospective review of 584 patients with a first-time lateral patellar dislocation, Christensen et al 4 concluded that trochlear dysplasia, elevated TT-TG distance, patella alta, age <18 years at the initial dislocation, and female sex were associated with ipsilateral patellar instability. In that study, all patients were <18 years old at the initial patellar dislocation, and there were 2 more women than men in the suture tape cohort. While postoperative MRIs were not taken on any patient in the present study, the mean preoperative TT-TG distance was slightly higher in the ST group compared with the no-ST group (17.24 vs 16.55 mm, respectively; P = .372). These parameters would suggest patients in the ST group were at greater risk for persistent patellar instability. In addition, no statistically significant difference was found in the Caton-Deschamps index between the 2 cohorts, either pre- or postoperatively (P = .798 and P = .751, respectively), suggesting that neither cohort had more severe patella alta. Last, while the Dejour classification to determine trochlear dysplasia was not measured in this study, the lack of statistically significant difference between groups for pre- and postoperative measurements of the sulcus angle, congruence angle, lateral translation, and lateral patellofemoral angle and preoperative measurements of lateral trochlear inclination ensures that there were no confounding imaging variables that led to the increase in patellar instability seen in the no-ST group.
Limitations
While the findings of the present study are encouraging, some limitations should be considered. All procedures were performed by a single surgeon at a single institution, and the sample size was relatively small. It was a nonrandomized retrospective database review, and the potential for selection bias exists. There is the potential that some eligible patients were not identified. Moreover, the follow-up period in this study was relatively short, and patients in the no-ST group had longer follow-up times and higher failure rates than those in the ST group. Although it may be possible that the failure rate was higher in the no-ST group because of the longer follow-up times, it is likely more attributable to the evolving knowledge and changes in practice over time. On average, the patients in the ST group underwent surgery in 2016, while patients in the no-ST group underwent surgery in 2014. Although there were no group differences in patient-reported outcomes, this could be attributed to type II errors. Furthermore, we did not obtain long-leg standing radiographs to assess coronal mechanical axis malignment. However, it is customary that coronal alignment is assessed during physical examination, and no excessive genu varum or valgum was reported.
Future prospective studies are still needed to evaluate the use of suture tape augmentation repair in patients who did not sustain a chondral or osteochondral lesion. Studies have examined the difference between suture tape and MPFL autografts. However, to our knowledge, no study has examined suture tape augmentation repair of the MPFL compared with traditional MPFL allograft reconstruction.
Conclusion
The results of the present study indicate that treating PPDs with chondral or osteochondral injury using suture tape to augment and repair the MPFL poses promising advantages over not repairing the MPFL, including fewer postoperative patellar instability episodes and lower rates of return to the OR, without the need for traditional MPFL allograft reconstruction.
Footnotes
Final revision submitted September 12, 2023; accepted October 5, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A.S. has received education support from Micromed; speaking fees from Arthrex; and hospitality payments from Smith + Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Children’s Hospital of Orange County (ref No. 1001409-1).