
Abstract
Background:
While the biomechanical properties of the native medial patellofemoral ligament (MPFL) have been well studied, there is no comprehensive summary of the biomechanics of MPFL reconstruction (MPFLR). An accurate understanding of the kinematic properties and functional behavior of current techniques used in MPFLR is imperative to restoring native biomechanics and improving outcomes.
Purpose:
To provide a comprehensive review of the biomechanical effects of variations in MPFLR, specifically to determine the effect of graft choice and reconstruction technique.
Study Design:
Systematic review.
Methods:
A systematic review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. A total of 32 studies met inclusion criteria: (1) using ≥8 human cadaveric specimens, (2) reporting on a component of MPFLR, and (3) having multiple comparison groups.
Results:
Gracilis, semitendinosus, and quadriceps grafts demonstrated an ultimate load to failure (N) of 206.2, 102.8, and 190.0 to 205.0 and stiffness (N/mm) of 20.4, 8.5, and 21.4 to 33.6, respectively. Single-bundle and double-bundle techniques produced an ultimate load to failure (N) of 171 and 213 and stiffness (N/mm) of 13.9 and 17.1, respectively. Anchors placed centrally and superomedially in the patella produced the smallest degree of length changes throughout range of motion in contrast to anchors placed more proximally. Sutures, suture anchors, and transosseous tunnels all produced similar ultimate load to failure, stiffness, and elongation data. Femoral tunnel malpositioning resulted in significant increases in contact pressures, patellar translation, tilt, and graft tightening or loosening. Low tension grafts (2 N) most closely restored the patellofemoral contact pressures, translation, and tilt. Graft fixation angles variably and inconsistently altered contact pressures, and patellar translation and tilt.
Conclusion:
Data demonstrated that placement of the MPFLR femoral tunnel at the Schöttle point is critical to success. Femoral tunnel diameter should be ≥2 mm greater than graft diameter to limit graft advancement and overtensioning. Graft fixation, regardless of graft choice or fixation angle, is optimally performed under minimal tension with patellar fixation at the medial and superomedial patella. However, lower fixation angles may reduce graft strain, and higher fixation angles may exacerbate anisometry and length changes if femoral tunnel placement is nonanatomic.
The medial patellofemoral ligament (MPFL) serves as the primary restraint against lateral patellar translation.3,18 Lateral patellar dislocation results in tearing of the MPFL and medial retinaculum, which can contribute to recurrent patellar instability. 25 MPFL reconstruction (MPFLR) is the primary operative treatment (isolated or with concomitant procedures) for patellar instability that is refractory to nonoperative management. Data demonstrate reliably improved functional and clinical outcomes at both short- and midterm follow-up with low rates of recurrent instability.25,43,45,47
Several technical variations of MPFLR, as well as medial quadriceps tendon–femoral ligament (MQTFL) and the medial patellotibial ligament (MPTL) have been studied.# However, clinical reports of poor function, persistent pain, and recurrent dislocations resulting from malpositioned tunnels and improper graft tensioning continue to be seen.6,11,43 While the biomechanical properties of the native MPFL have been well studied,7,19,49 there is no comprehensive review of MPFLR biomechanics. An accurate understanding of the kinematic properties and functional behavior of current techniques used in MPFLR is imperative to improving outcomes and restoring native biomechanics.
The aim of this study was to systematically review the biomechanical effects of the variations in MPFLR techniques. Specifically, we sought to determine the effect of graft choice and reconstruction technique (single- vs double-bundle, patellar fixation, femoral fixation, fixation angle, and graft tension) on patellofemoral biomechanics; the effect of concomitant procedures, such as MQTFL and MPTL reconstruction; and which combination of techniques, procedures and implants most closely restores patellofemoral kinematics and functionality to the native state. We hypothesized that anatomic reconstructions with centromedial and superomedial patellar fixation and femoral tunnel placement at the native MPFL attachment would provide the most favorable biomechanical data.
Methods
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines were followed to conduct the study. A review of the literature was performed on May 4, 2022, using 3 databases: PubMed, Scopus, and Ovid. The following string was utilized for searching: (“Medial knee” or “medial restraint” or “medial restraints” or “medial patellofemoral ligament” or “medial patellofemoral ligaments” or “medial Patellofemoral complex” or “medial structures” or “medial structure” or “medial retinacululum” or “MPFL” or “MPFC”) AND (“Biomechanics” or “Biomechanical study” or “Cadaver biomechanical study” or “Cadaver” or “Cadaveric” or “Cadaver knee” or “cadaveric knee”). The search string was kept broad to minimize the possibility of overlooking relevant biomechanical studies on the medial patellar restraints. The initial title and abstract screening yielded 1684 studies (Figure 1), which were then imported into Covidence systematic review software (Veritas Health Innovation; www.covidence.org). Only 871 studies remained after duplicates were removed.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart exhibiting inclusion and exclusion technique for extraction. *Several studies reported on multiple biomechanical analysis categories.
Study Selection
Full-text screening was performed by 2 orthopaedic surgery residents (K.C., J.W.). Any disagreements on studies were resolved through consensus. If a consensus could not be reached, the final decision was made by the senior author (A.Y.). Studies were reviewed based on the following inclusion criteria: (1) studies in the English language, (2) studies using human cadaveric specimens, (3) studies including ≥8 cadaveric specimens in analysis, (4) studies reporting on a component of isolated MPFLR, and (5) studies having multiple comparison groups. MPTL and MQTFL data were included for their contributions to the medial patellofemoral complex (MPFC). Exclusion criteria included (1) studies not in the English language; (2) nonbiomechanical studies, such as any clinical studies, systematic reviews, meta-analyses, and expert opinions; (3) animal-based studies; (4) studies addressing significant concomitant anatomic pathology such as patella alta or elevated tibial tubercle–trochlear groove (TT-TG) measurements requiring tibial tubercle osteotomies; and (5) descriptive studies that did not include ≥2 comparison groups. Ultimately, 37 studies were included for qualitative synthesis: 7 studies reported on patellar fixation,13,15,29,34,37,39,44 8 studies reported on femoral fixation,5,13,17,28,31,42-44 20 studies reported on patellofemoral contact pressures and kinematics, ** 15 studies reported on patellar force and translation, †† and 12 studies reported on graft biomechanics ‡‡ (several studies reported on multiple biomechanical analysis categories).
Results
Graft Types
Eleven studies evaluated the biomechanics of graft type. §§ Several graft choices were utilized for MPFLR, including the gracilis, tensor fasciae latae, semitendinosus, quadriceps, and adductor magnus tendon (Table 1). Gracilis and tensor fasciae latae tendon allografts showed no significant differences in lateral patellar tilt, lateral patellar translation, or medial or lateral joint contact pressures.23,43 While the semitendinosus tendon autografts demonstrated significantly lower load to failure and stiffness than gracilis tendon autografts, these differences are likely attributed to fixation techniques and a 100% failure rate by patellar soft anchor pullout in the semitendinosus reconstructions and may not represent the true qualities of this graft.33,46 Quadriceps tendon grafts, which are created by harvesting the central third of the superficial layer of the quadriceps tendon, detaching it proximally, and folding the harvested portion medially 90°, yielded similar results.16,28,33 Given the proximity of the adductor tubercle to the MPFL insertion, the adductor magnus tendon is also used, albeit less commonly, as a graft for MPFLR as seen in the adductor-transfer technique (Table 1).30,48
Biomechanical Data of Native MPFL and Various Reconstruction Graft Types a

Tensor fascia lata grafts were excluded from the table due to unavailable raw numerical data.MPFL, medial patellofemoral ligament.
In lieu of biologic grafts, polyester suture tape has also been proposed for use in MPFLR, both as a standalone graft27,38,46 and for augmentation. 27 Notably, however, native patellofemoral pressure distributions have also been shown to be inadequately restored after MPFLR regardless of graft choice (Table 1). 23
Single- Versus Double-Bundle Reconstruction
Single- and double-bundle MPFLR differ primarily in their patellar attachment points. Single-bundle reconstruction utilizes 1 anchor point in the middle third of the medial patella while double-bundle reconstruction uses 2 fixation points—typically one at the midline of the patella and the other at the superomedial patella. Double-bundle reconstructions demonstrated higher ultimate load to failure and stiffness compared with single-bundle constructs (Table 2). 32
Biomechanical Data for Single- Versus Double-Bundle Techniques 32

Patellar Fixation
Location
Concerning the optimal patellar attachment points, anchors located distally in the superomedial patella produced the smallest degree of length change throughout range of motion. Anchors placed centrally in the superomedial patella demonstrated graft length changes of 0 mm to 2.6 mm of slackening through a full range of knee flexion; proximally located, 0 mm to 2.0 mm of slackening; and distally located, 0.5 mm of tightening to 0.8 mm of slackening. 44
Similarly, when using nonanatomic femoral attachments, anchors located proximally in the superomedial patella demonstrated the greatest anisometry (4.53-8.22 mm) compared with distal patellar anchors (2.55-8.17 mm) and central patellar anchors (3.68-8.21 mm). 13
Fixation Methods
Several studies reported on the biomechanical properties of the various patellar fixation methods, including transosseous tunnels with and without interference screws, sutures only, and a variety of suture anchors, among others (Table 3).15,29,34,37,39
Biomechanical Data for Different Patellar Fixation Techniques

Femoral Tunnel Position
Eight studies evaluated the effects of femoral tunnel positioning (Table 4).5,3,17,28,31,42-44 Several studies demonstrated that femoral tunnels positioned at the anatomic footprint of the MPFL—at the midpoint between the adductor tubercle and medial epicondyle—under low tension most closely restores native patellofemoral contact pressures and isometry.43-45 Specifically, anatomic reconstructions demonstrated patellofemoral contact areas of 108.5 to 276.4 mm2 medially and 153.5 to 254.1 mm2 laterally, contact pressures of 59.6 to 108.0 N/cm2 medially and 54.0 to 130.0 N/cm2 laterally, graft length variability as little as 1.1 to 2.1 mm through the range of knee flexion, stiffness of 2.5 to 2.8 N/mm, and strain of 120% to 130%.5,17,28,42-44 Deviating from the anatomic femoral position was found to significantly alter contact pressures and patellar kinematics, which was further exacerbated by increased graft tension during fixation (Table 4). 42
Graft Length Changes by Femoral Fixation Position (relative to anatomic)

ME, medial epicondyle.
Proximal malpositioning tended to increase medial contact pressures in deep knee flexion and cause graft tightening through the range of knee flexion, whereas distal malpositioning increased medial contact pressures in near full knee extension and caused graft loosening. Both increased patellar translation and lateral contact pressures (Table 4).5,42-44
While anterior and posterior malpositioning were not significantly different from the anatomic tunnel position, anterior malpositioning demonstrated initial graft loosening up to 2.0 mm in early knee flexion followed by gradual tightening from 0.4 to 10.2 mm in deep knee flexion. Posterior malpositioning, in contrast, caused graft loosening through the range of knee flexion by as much as 3.8 mm in deep flexion (Table 4).5,44
Femoral tunnels created at the medial epicondyle were found to increase graft length variability by as much as 5.8 mm. 13 Femoral fixation of the graft around the intact adductor tendon, as seen in the adductor-sling technique, caused graft tightening from 1.95 to 13.38 mm through the range of knee flexion. 48
Graft Tension Angle
Seven studies reported on the implications of knee flexion angle during graft tensioning (Table 5).5,17,24,26,38,42,50 When tensioned in low angles of knee flexion, strain was found to be significantly lower in reconstructed knees compared with the native state, but significantly higher in high angles of knee flexion. 17 Varying graft tension angle had a negligible effect on lateral contact pressures even as MPFLR demonstrated a mild offloading effect on lateral pressures overall.23,24,38,42,50
Biomechanical Data by Graft Tension Angle
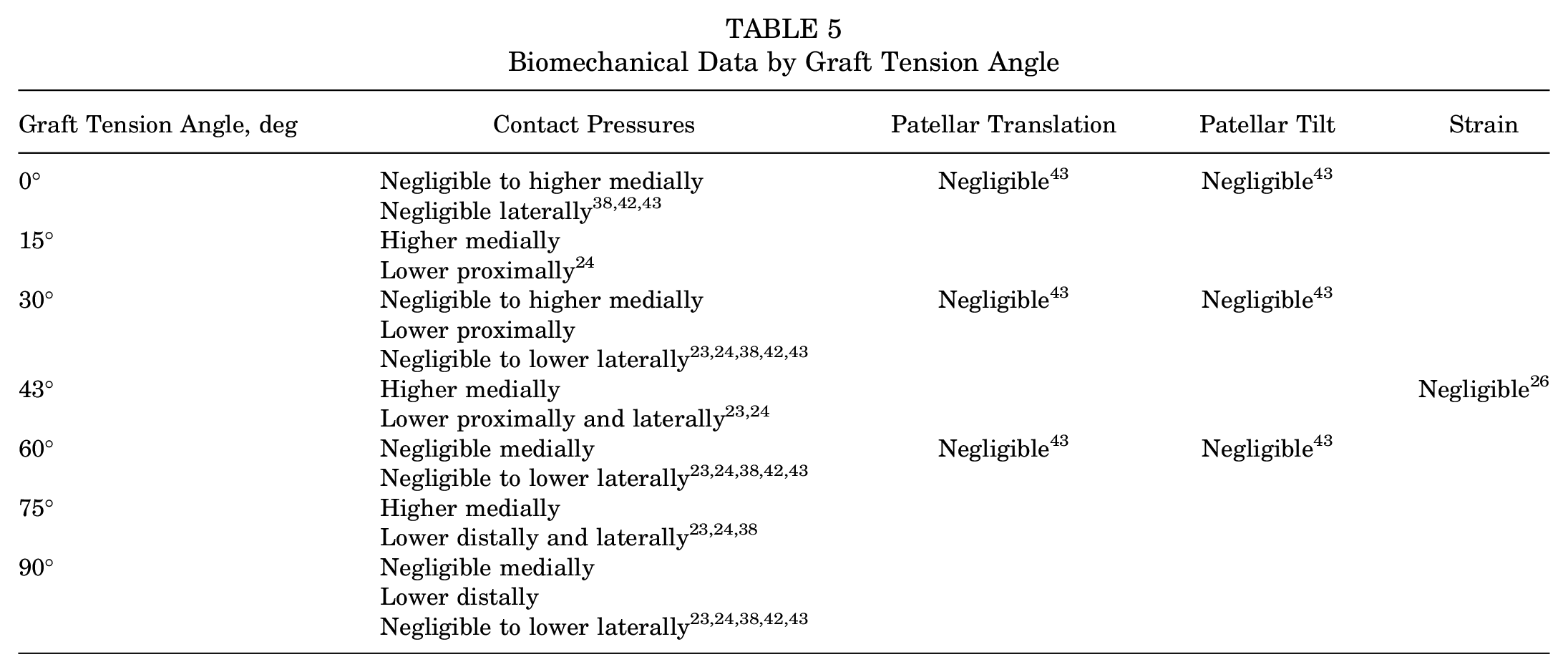
Burrus et al 5 showed that when nonanatomic femoral tunnels were used, fixing the grafts in higher degrees of knee flexion caused significantly greater graft anisometry than those fixed at lower angles of knee flexion from 30° to 45°. Regarding selective bundle tensioning in double-bundle reconstructions, Zumbansen et al50 found that tensioning the proximal bundle at 30° of knee flexion and the distal bundle at 75° most closely restored patellofemoral contact pressures to the native state.
Graft Tension
Four studies evaluated the mechanical effects of graft tension.1,4,42,43 The use of low (2 N) tension most closely restored the patellofemoral contact pressures, patellar translation, and patellar tilt to the native knee.4,42,43 Overtensioning the MPFL with as little as 10 N was reported to have several deleterious effects, including significantly increased medial patellar tilt, restricted lateral patellar translation, increased medial patellofemoral contact pressures, and reduced lateral patellofemoral contact pressures.4,42,43 Increasing graft tension beyond 10 N was found to further exacerbate these effects in a dose-response manner. 42
The use of a femoral interference screw was found to increase graft tension by as much as 100% to 552% (P < .01), demonstrating a post screw insertion tension of 13.0 N, 16.5 N, and 20.1 N when preloaded with 2 N, 5 N, and 10 N, respectively. 1 While interference screw size did not influence graft tension, larger diameter grafts (7-8 mm) demonstrated significantly higher graft tension as compared with smaller diameter grafts (5-6 mm) (16.0 N vs 9.1 N, respectively; P < .001). 1 Additionally, a looser graft-tunnel interference fit (ie, grafts that had a diameter >2 mm smaller than the femoral tunnel diameter) was shown to have a significantly smaller increase in tension than a tighter graft-tunnel interference fit (0-1 mm) (P < .001). 1
Last, a study by Saper et al 39 examined patellar fixation of all-soft suture anchors and classic solid suture anchors by setting a standard graft length of 55 mm to mimic the length of the intact native MPFL rather than tensioning. However, this study did not make comparisons with graft tensioning or the native MPFL.
MPTL Reconstruction
Adjacent to the MPFL, the MPTL serves as a secondary restraint to lateral patellar displacement providing stability beyond 30° of knee flexion and is responsible for patellar rotation and tilt beyond 45°.2,14 MPTL deficiency does not create significant patellar instability on its own but has been found to exacerbate instability in the MPFL-deficient knee. 14
Isolated MPTL reconstruction was found to generate similar contact pressures to native and MPFL-reconstructed knees but failed to adequately restore the medial patellar restraints and patellar stability.2,14 While MPFLR has been shown to restore medial stability, combined MPFLR and MPTL reconstruction more closely approximated native patellar tracking compared with MPFLR alone. 14
Medial Quadriceps Tendon–Femoral Ligament Reconstruction
Similarly, MQTFL reconstruction, first described by Fulkerson and Edgar, 12 is another technique aimed at restoring the medial patellar restraints. 41 The MQTFL is an anatomically distinct component of the medial retinaculum lying in proximity to the MPFL extending from its femoral attachment just proximal to the native MPFL footprint and inserting anteriorly into the distal quadriceps tendon. 12
According to Spang et al, 41 both MQTFL reconstruction and MPFLR caused medialization of the patella and significantly lower patellofemoral contact pressures and areas compared with the native state. Compared with MPFLR, MQTFL reconstruction was found to be significantly less constrained in lateral translation and better approximated the native medial restraining forces. MQTFL and MPFL demonstrated equivalent contact areas between 30° and 90° of flexion, but the MQTFL had a significantly larger contact area in deep flexion at 110°. Additionally, compared with the native state, medial contact pressures were higher after MPFLR and lower after MQTFL reconstruction, and lateral contact pressures were lower for both reconstructions; however, these were not statistically significant.
Discussion
The present systematic review summarizes the current data on how variations in different aspects of MPFLR technique may affect postoperative biomechanics. In general, it appears that graft selection has minimal effect on mechanics. Both single- and double-bundle techniques tend to produce stronger and stiffer grafts than the native MPFL. Identifying the isometric points for fixation on the patellar side and femoral side (ie, Schöttle point) is critical to minimize anisometry. For standard, isolated MPFLR, a femoral fixation point more proximal to the Schöttle point results in increased tension and contact pressure with flexion, whereas a more distal femoral fixation point results in increased contact pressure with extension and graft loosening. The graft should also be fixated under low tension (ie, with the patella centered in the trochlea in flexion or centered above the trochlea in extension). However, per the senior author's experience, it can be difficult to intraoperatively gauge exact graft tension. Therefore, we recommend setting the graft length intraoperatively such that it can have no tension when the knee is in full extension. It is possible that MPTL or MQTFL reconstruction may help improve tracking. The data from the present study may help surgeons fine-tune techniques to optimize kinematics to most similarly replicate native anatomy.
The most common graft choices for MPFLR are gracilis and semitendinosus allografts. 22 Each of these allografts may result in appropriate mechanical properties to approximate those of the native MPFL. In the studies included, the gracilis may have a greater ultimate load to failure (206.2 N) and stiffness (20.4 N/mm) relative to semitendinosus (102.8 N load to failure, 8.5 N/mm stiffness). Nevertheless, the exact graft selection may not substantially influence outcomes, as mechanical properties also depend on the configuration of the graft. For example, double-bundle techniques tended toward greater ultimate load to failure and stiffness in the available data relative to single-bundle techniques. Ultimately, it remains unknown the optimal level of load to failure and stiffness and whether it is necessary for these variables to be high or as close to those of the native MPFL as possible.
The fixation location of the graft is one of the most discussed and well-described aspects of MPFLR mechanics. Location of patellar and femoral fixation can have substantial effects on graft isometry, and suboptimal graft isometry (or greater anisometry with knee flexion) can lead to more tensioning and lengthening of the graft over repeated cycles of knee flexion. The native MPFL is a dynamic structure and is anisometric in extension and early flexion. 21 Furthermore, beyond 30° of knee flexion, the MPFL displays isometry without substantial length change.9,19,21,44,49 However, in the setting of other pathologies such as patella alta, significant slackening of the native MPFL has been demonstrated at elevated Caton-Deschamps indices (CDI) above 1.4, and significant graft slackening has been observed at a CDI of 1.6 for MPFLR and MQTFL reconstruction techniques.9,49 Another study by Redler et al 35 found that elevated CDI and TT-TG distances >20 mm resulted in significantly altered MPFL isometry. The data in the current review, however, excluded studies with pathologies such as patella alta and lateralized tibial tubercles; the data suggest that the patellar fixation points of anchors for isolated MPFLR should be centered in the superomedial patella and centered on the medial patella for a double-bundle graft and central for a single-bundle technique.13,44 These findings are further supported by a cadaveric study of the native MPFL by Huddleston et al, 19 who found the greatest length changes through flexion at the quadriceps tendon insertion as compared with insertions at the superomedial patella, osseous footprint, and patellar midpoint.
Utilizing an anatomic femoral tunnel placement may be even more critical than the patellar fixation points, as variations in femoral tunnel placement appear to produce even greater changes in graft elongation.2,5,13,28,31,42-44 Proximal malpositioning of the graft on the femoral side causes increased pressures, patellar tilt, and elongation in flexion, while distal malpositioning of the graft causes these findings more in extension.5,42-44 Currently, the anatomic footprint of the MPFL, located at the midpoint between the adductor tubercle and medial epicondyle, is approximated during MPFLR using a radiographic surrogate called the Schöttle point.40,42-44 On a lateral radiograph, this point is located 1.3 mm anterior to the posterior cortex extension line and 2.5 mm distal to the posterior origin of the medial femoral condyle (Figure 2). 40 The Schöttle point remains the preferred fixation point on the femoral side, and care should be taken to carefully identify this and confirm tunnel location fluoroscopically.
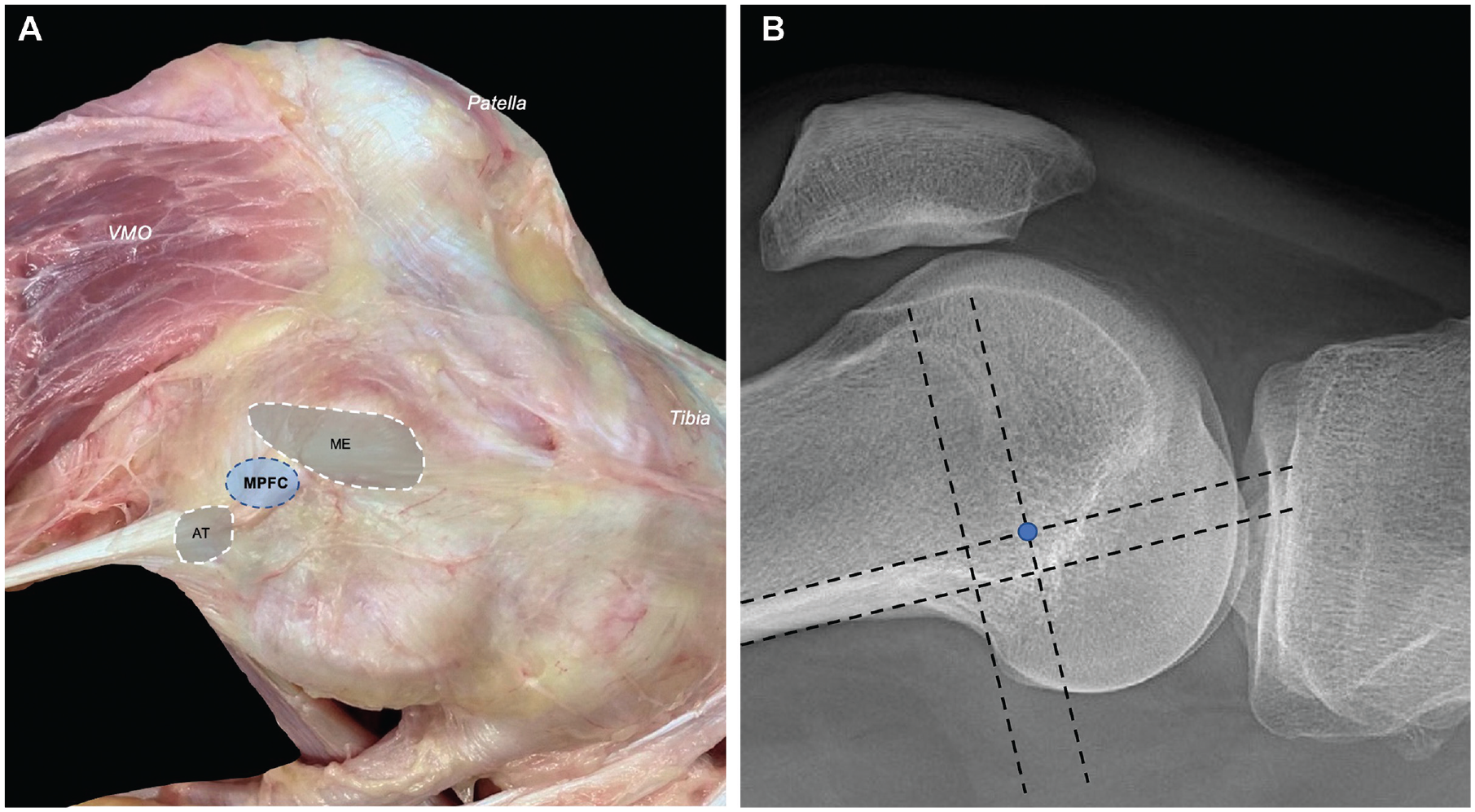
(A) The medial patellofemoral ligament (MPFL) origin is found approximately halfway between the medial femoral epicondyle and the adductor tubercle. (B) The Schöttle point (a radiographic surrogate of the MPFL origin) is demonstrated on a perfect lateral radiograph as the blue point 1.3 mm anterior to the posterior cortex extension line and 2.5 mm distal to the posterior origin of the medial femoral condyle.40,42-44 AT, adductor tubercle; ME, medial epicondyle; MPFC, medial patellofemoral complex (ie, MPFL origin); VMO, vastus medialis oblique.
It is apparent that fixing the graft in low or minimal tension states is beneficial.38,43 Overtensioning the graft was found to not only increase contact pressures medially but also alter patellar tilt.4,42,43 Ackermann et al 1 found that interference screw insertion at the femoral origin increased graft tension by approximately 10 to 11 N regardless of the preload state's being 2 N, 5 N, or 10 N. They additionally found that larger diameter grafts (7-8 mm) and tighter graft-tunnel interference fit demonstrated significantly higher graft tension compared with small diameter grafts (5-6 mm) and looser graft-tunnel interference fit (ie, grafts that had a diameter >2 mm less than the femoral tunnel), potentially because the smaller screws resulted in less friction when secured and less graft advancement in the tunnel. Surgeons should be aware that femoral interference screw insertion, larger diameter grafts, and graft-tunnel interference fit can significantly increase graft tension to avoid the risk of inadvertent graft overtensioning. In the authors’ experience, these data are particularly important to consider intraoperatively, as grafts do not always advance with interference screw placement; but if they do advance, the tension on them can increase. To minimize the risk of overtensioning, the authors recommend setting the graft length intraoperatively while the knee is in full extension (or at the desired fixation angle) to have no tension, rather than selecting predetermined graft lengths. This technique allows appropriate graft length to be set by assessing a firm endpoint at 1 quadrant of lateral patellar translation. 9
The ideal knee flexion angle of graft fixation was less clear in the biomechanical literature. There were disparate results, with recommendations ranging throughout range of motion. However, lower angles of knee flexion may reduce strain on the graft. 17 If femoral tunnel placement is nonanatomic, fixation of the graft in greater degrees of knee flexion may have more detrimental effects in terms of isometry and length changes. 5
The biomechanical data on reconstruction of the MPTL and MQTFL appear favorable. Incorporating and reconstructing structures in the MPFL complex may better represent native anatomy. Further studies on these newer reconstruction techniques will be valuable to best understand their role in primary MPFLR.
In light of these biomechanical data as well as personal experience, the authors’ preferred surgical technique is as follows in Table 6.
Authors’ Preferred Surgical Decision Making for Isolated MPFLR a
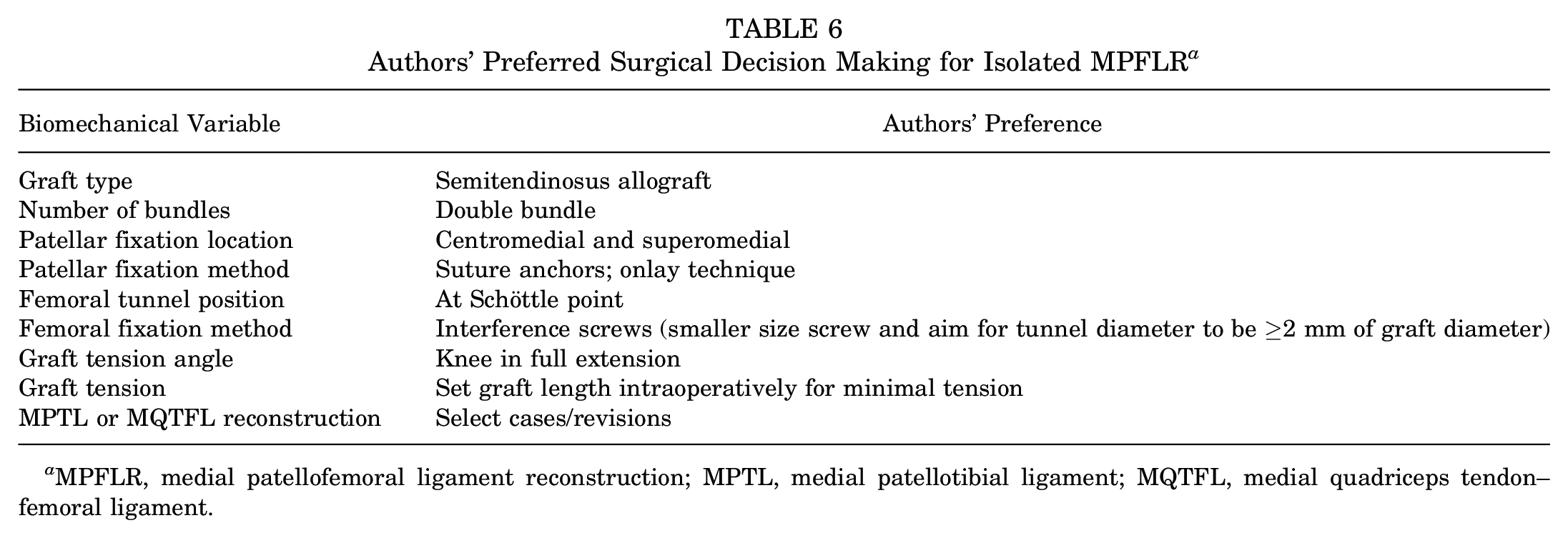
MPFLR, medial patellofemoral ligament reconstruction; MPTL, medial patellotibial ligament; MQTFL, medial quadriceps tendon–femoral ligament.
Limitations
This systematic review is composed of the data of previously published studies, each with its own individual limitations. Variability in handling of specimens, testing conditions, protocols, and data collected did not allow for a meta-analysis and may be a source of confounding results. The inclusion and exclusion criteria selected sought the most relevant and updated studies, but it is possible that useful biomechanical studies may have been omitted. The lack of comparative studies makes drawing of definitive conclusions challenging, but trends within the data may be noted. However, the relative paucity of studies assessing individual variables may confound conclusions and limit the ability to elucidate trends. The biomechanical data reviewed are not a substitute for clinical data, and both types of study should be evaluated critically and in conjunction with one another.
Conclusion
Biomechanical data on MPFLR allow surgeons to understand the effects of alterations in technique on graft isometry, patellar position, contact pressure, and risks of future instability. Data demonstrate that placement of the MPFLR femoral tunnel at the Schöttle point is critical to success. Femoral tunnel diameter should be ≥2 mm greater than graft diameter to limit graft advancement and overtensioning. Graft fixation, regardless of graft choice or fixation angle, is optimally performed under minimal tension with patellar fixation at the medial and superomedial patella. However, lower fixation angles may reduce graft strain, and higher fixation angles may exacerbate anisometry and length changes if femoral tunnel placement is nonanatomic.
Footnotes
Final revision submitted August 21, 2023; accepted October 1, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.A. has received education payments from Smith & Nephew. M.H. has received consulting fees from DJO-Enovis, Moximed, and Vericel; publishing royalties and financial or material support from Elsevier; education support from Arthrex, Foundation Medical LLC, Medwest Associates, and Smith & Nephew; honoraria from Encore Medical LP; hospitality payments from Orthalign, Stryker, and Medical Device Business Services. A.Y. has received consulting fees from AlloSource, Arthrex, JRF Ortho, Stryker, and Olympus America; holds stock or stock options in PatientIQ and Sparta Biomedical; has received education payments from Medwest Associates; and has received honoraria from Joint Restoration Foundation. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.