
Abstract
Background:
Diminished postoperative knee extension strength may occur after anterior cruciate ligament reconstruction (ACLR) with quadriceps tendon (QT) autograft. Factors influencing the restoration of knee extensor strength after ACLR with QT autograft remain undefined.
Purpose:
To identify factors that influence knee extensor strength after ACLR with QT autograft.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The authors performed a retrospective review of patients who underwent primary ACLR with QT autograft at a single institution between 2010 and 2021. Patients were included if they completed electromechanical dynamometer testing at least 6 months after surgery. Exclusion criteria consisted of revision ACLR, <6 months of follow-up, concomitant procedure (osteotomy, cartilage restoration), and concomitant ligamentous injury requiring surgery. Knee extension limb symmetry index (LSI) was obtained by comparing the peak torque of the operated and nonoperated extremities. Univariable and multivariable analyses were performed to identify factors associated with knee extension LSI in the patient, injury, rehabilitation, and preoperative patient-reported outcomes score domains.
Results:
A total of 107 patients (58 male; mean age, 22.8 years) were included. Mean knee extension LSI of the overall cohort was 0.82 ± 0.18 at 7.5 ± 2.0 months; 35 patients (33%) had a value of ≥0.90. Multivariable analysis demonstrated significant negative associations between knee extension LSI and female sex (−0.12; P < .001), increased age at the time of surgery (−0.01; P = .018), and larger QT graft width (−0.049; P = .053).
Conclusion:
Factors influencing knee extensor LSI after ACLR with QT autograft in this study population spanned patient and surgical factors, including female sex, older age at the time of surgery, and wider graft harvest. Surgeons should consider the association between these factors and lower postoperative knee extensor LSI to optimize patient outcomes.
The selection of quadriceps tendon (QT) autograft as a primary graft in anterior cruciate ligament reconstruction (ACLR) has increased over the past decade. 1 The reported benefits of QT autograft in ACLR include favorable donor site morbidity profile, with decreased risk of anterior knee pain and hamstring weakness when compared with bone-patellar tendon-bone (BPTB) and hamstring tendon (HT) autograft, respectively.5,24,32 Moreover, QT autograft can be obtained without a bone block, diminishing the risk of patellar fracture compared with BPTB autograft.9,28
Regaining full knee extension strength after ACLR with the use of QT autograft can be challenging as quadriceps weakness is often present in the postoperative rehabilitation period.18,22,31,38 Persistent knee extensor strength deficit after ACLR is concerning, as correlation with graft retear, inferior patient-reported outcomes (PROs), lower rate of return to sport, altered knee joint kinematics and loading patterns, and increased risk of osteoarthritis have been reported.10,13-17,33 Accordingly, postoperative rehabilitation after ACLR often emphasizes restoration of knee extensor strength, with return-to-sport testing protocols frequently measuring knee extension strength during the rehabilitation process.
Factors that influence restoration of knee extensor strength after ACLR with alternative grafts to QT autograft, such as HT and BPTB autografts, have been reported previously.27,40,41 The factors influencing the restoration of knee extensor strength after ACLR with QT autograft, however, remain undefined. Therefore, the purpose of this study was to identify factors that influence knee extensor strength after ACLR with QT autograft. We hypothesized that patient, injury, surgical, and rehabilitation factors would be associated with postoperative knee extensor limb symmetry index (LSI).
Methods
Patient Selection
Institutional review board approval was obtained for the study protocol. We retrospectively reviewed a cohort of patients who underwent ACLR with QT autograft between 2010 and 2021 among 10 sports medicine fellowship-trained surgeons at a single institution. Patients were included in the analysis if a primary single bundle ACLR with QT autograft was performed and at least 1 isometric strength testing session via electromechanical dynamometer (Biodex Medical Systems) was completed at a minimum of 6 months postoperatively. Patients who underwent meniscal repair, meniscal debridement, and cartilage debridement were included. Patients were excluded if they had <6 months of follow-up, concomitant ligamentous injury requiring surgical intervention, concomitant cartilage restoration surgery, concomitant osteotomy, or revision surgery. The need for informed consent was waivered.
Postoperative Rehabilitation
Patient rehabilitation after ACLR was at the discretion of the operating surgeon and treating physical therapist. A general rehabilitation protocol consisting of pain and swelling control with quadriceps activation and gait normalization occurred during the first month after surgery. Strengthening to include the quadriceps was subsequently performed, with initiation of running 3 to 4 months postoperatively. Sport-specific activities were then initiated 5 to 6 months postoperatively with progression under the direction of the physical therapist.
Isometric Strength Testing
Patients completed isometric strength testing throughout the postoperative period as part of a rehabilitation treatment plan with individualized postoperative protocols. The measurements obtained during these sessions were used to monitor return of quadriceps strength and assess symmetry to the contralateral limb, as well as guide advancement of activity type and intensity during the rehabilitation process. Given that the number of testing visits, latency period to first testing session, and interval between sessions were not standardized across patients, data were included only from sessions that occurred at least 6 months postoperatively. If multiple testing sessions were conducted, this was noted, and data were recorded from the 3 most recent timepoints. Isometric strength testing was performed using a System 3 electromechanical dynamometer (Biodex Medical Systems) and conducted by trained physical therapists familiar with operation of the Biodex equipment and appropriate patient positioning. Patients were seated in the electromechanical dynamometer with the operated knee flexed to 60° and then placed in a knee attachment positioned proximal to the medial malleolus. The axis of knee rotation was aligned with the dynamometer shaft. Shoulder, waist, and thigh straps were used to secure the patient to the seat of the dynamometer. In-line extension and flexion strength were then assessed via alternating 5-second maximal contractions of the quadriceps and hamstrings, respectively, for a total of 3 repetitions per muscle group, ensuring at least 30 seconds of rest between each contraction. This process was then repeated for the contralateral (ie, nonoperated) limb. Peak extension torque values were then compared between the operated knee and nonoperated knee to obtain a ratio of knee extensor strength symmetry, also known as LSI, to obtain normalized values of knee extensor strength for comparison. This system is accurate to 1% of the full scale (500 ft-lbs, 678 Nt·m) testable for torque.
Variables Assessed
All data were obtained from the patients’ electronic medical records. The included variables were categorized into domains: patient, injury, surgical, and both preoperative and postoperative rehabilitation. A preoperative PRO domain was also utilized for a subset of patients with complete data collection. Patient variables included age at the time of surgery, sex, level of sports participation, and body mass index (BMI). Injury variables included laterality, presence of a cartilage lesion, time from injury to surgery, and time from surgery to isometric strength testing. Surgical variables included tourniquet time, preoperative regional anesthesia, QT autograft harvest length, QT autograft harvest width, QT autograft harvest thickness (full versus partial), fixation method, and concomitant meniscal treatment at the time of ACLR. The rehabilitation domain included preoperative rehabilitation (categorized as whether or not a formal therapy program was completed before surgery) and postoperative rehabilitation (categorized as whether or not blood flow restriction [BFR] therapy was received during formal therapy after surgery). Preoperative PROs included visual analog scale for pain, mental and physical domains of the Patient-Reported Outcomes Measurement Information System score, Marx score, and International Knee Documentation Committee (IKDC) score.
Statistical Analysis
All statistical analyses were performed with SAS Version 9.4 (SAS Institute). Univariable associations with continuous variables were examined with the Pearson correlation coefficient (r), with the null hypothesis that r is equivalent to zero. Univariable associations with binary categorical variables were tested with the independent-samples t test. Univariable associations with multicategorical variables were tested with the 1-way analysis of variance F test. Tourniquet time was classified into 3 categories based on the median value (92 minutes) of the current cohort: no tourniquet used, <92 minutes, and ≥92 minutes. Time from injury to surgery was classified into 2 categories: ≤1.5 months and >1.5 months. Tourniquet time and time from injury to surgery were categorized due to skewed values not amenable to correction by data transformation. All tests were 2-sided.
Variables that had a univariable association with the outcome of P < .15 were selected for inclusion in the within-domain analysis. Within each domain, the selected variables were added into a multivariable linear regression, and stepwise backward elimination was employed until all variables in the model had associations of P < .15. The remaining variables from each domain were then added into a multivariable linear regression, and backward elimination with P < .15 was again employed.
The PRO domain was then analyzed with a subsample of 60 patients who had completed the PRO measures. Backward elimination as described previously was employed to find a final set of predictors among the PROs. The identified PROs were subsequently entered into a linear regression with the associated variables from the previous multivariable linear regression analysis. This sensitivity analysis was used to determine whether the predictors found using the cohort of 107 remained significant in the smaller sample when controlling for significant PROs.
Results
Analysis of Overall Cohort
From 705 patients initially considered, 107 patients (58 male) with a mean age of 22.8 years (range, 14-47 years) were included in this study (Figure 1). The mean ± SD of knee extensor strength LSI of the overall cohort was 0.82 ± 0.18 at a mean of 7.5 ± 2.0 months; 35 patients (33%) had a value of ≥0.90. 50% of patients were tested between 6 and 8.7 months and 75% were tested between 5 and 8.7 months.

Flowchart of final cohort included in statistical analysis. ACLR, anterior cruciate ligament reconstruction; PL, posterolateral; QT, quadriceps tendon.
After univariable analysis, associations with patient age, patient sex, and BMI were identified in the patient domain (Table 1). Within the injury domain, no associations were identified (Table 2). Surgical characteristics including QT autograft harvest width, tibial fixation method, and use of regional anesthesia were identified as factors to be included in the final multivariate analysis (Table 3). Rehabilitation factors did not reach statistical significance to be included in the final multivariate model (Table 4).
Patient Domain Characteristics Associated With Knee Extensor LSI (N = 107 Patients) a

Data are presented as mean ± SD or n (%) unless otherwise indicated. Boldface P values indicate variables that were included in the multivariate analysis (P < .15). LSI, limb symmetry index; BMI, body mass index.
Injury Domain Characteristics Associated With Knee Extensor LSI (N = 107 Patients) a

Data reported as mean ± SD or n (%) unless otherwise indicated. LSI, limb symmetry index; IQR, interquartile range [180.3 days – 259.3 days].
Mean ± SD, 4.3 ± 1.7 months; median [IQR], 1.3 months [1.2 months] [0.9 - 2.0]; range, 0-160 months.
Surgery Domain Characteristics Associated With Knee Extensor LSI (N = 107 Patients) a

Data reported as mean ± SD or n (%) unless otherwise indicated. Boldface P values indicate variables that were included in the multivariate analysis (P < .15). LSI, limb symmetry index.
Rehabilitation Domain Characteristics Associated With Knee Extensor LSI (N = 107 Patients) a
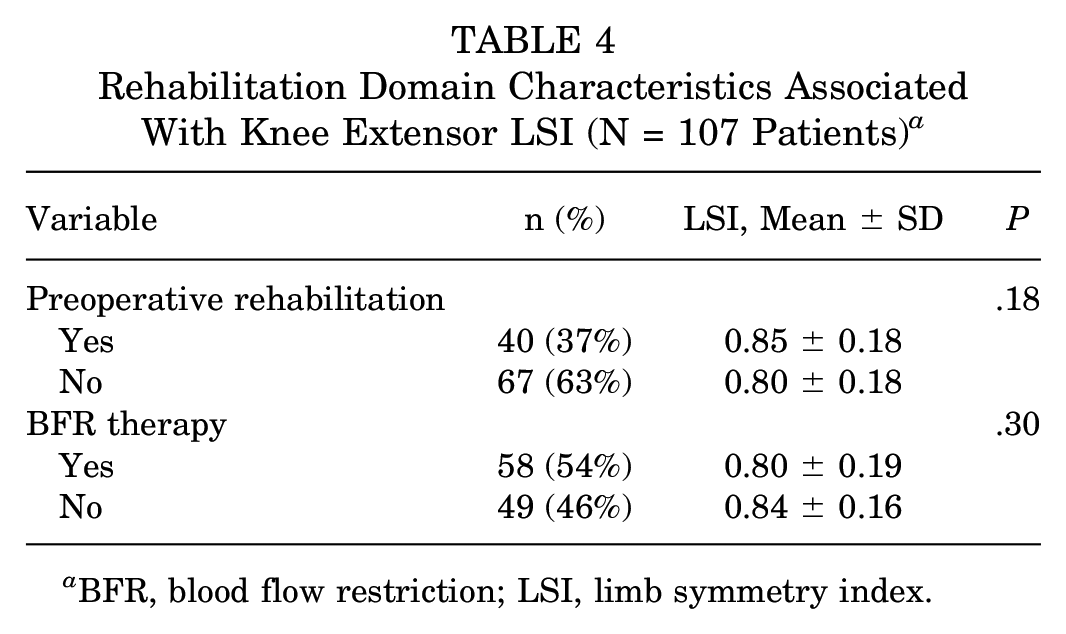
BFR, blood flow restriction; LSI, limb symmetry index.
Multivariable analysis of the overall study population identified female sex, older patient age, and QT autograft harvest width as factors associated with diminished knee extensor LSI (Table 5).
Multivariable Analysis of Overall Cohort Variables Associated With Knee Extensor LSI a

Intercept, 1.46 (0.24); P < .0001. LSI, limb symmetry index; SE, standard error.
Subgroup Analysis With Complete PROs
Univariable analysis of the 60 patients with complete preoperative PROs identified IKDC as a factor to be included in the final model with previously identified variables (Table 6). Including the IKDC in the multivariable model of age, sex, and graft width in the 60 patients with PRO data did not have a large effect on the estimates of the beta coefficients, and IKDC did not reach statistical significance for association (Table 7).
Preoperative PROs in Selected Cohort Associated With Knee Extensor LSI (n = 60 patients) a

Boldface P value indicates variable that was included in the multivariate analysis (P < .15). IKDC, International Knee Documentation Committee; LSI, limb symmetry index; PRO, patient-reported outcome; PROMIS, Patient-Reported Outcomes Measurement Information System; VAS, visual analog scale.
Multivariable Analysis of Selected Cohort Variables Including Preoperative PROs Associated With Knee Extensor LSI a

Intercept, 1.48 (0.30); P < .0001. LSI, limb symmetry index; IKDC, International Knee Documentation Committee; PRO, patient-reported outcome; SE, standard error.
Discussion
This retrospective review of patients who underwent ACLR with QT autograft at a single institution identified factors that were associated with lower postoperative knee extensor LSI at mean of 7.5 ± 2.0 months postoperatively in the study population. The factors that were associated with diminished postoperative knee extensor LSI include female sex, older age at the time of surgery, and larger QT autograft harvest width. Using a subset of patients, preoperative PROs were not found to be associated with knee extensor LSI and did not impact previous associations. The associated factors that were identified include both modifiable and nonmodifiable variables and should be considered in the management and treatment of an individual with an ACL tear undergoing ACLR with QT autograft.
In the current study, we identified the patient factors that may influence knee extensor LSI as being sex and age at the time of surgery. Similar findings were identified in a study that evaluated quadriceps strength recovery after ACLR with HT autograft, in which patient age at the time of surgery and patient sex were associated with strength recovery. 41 The impact of patient sex on knee extensor strength after ACLR has also been established in several previous studies with both HT and BPTB autografts, as female patients consistently demonstrate lower strength measures compared with male patients.25,27,36,40 Specific to QT autograft, female patients who underwent ACLR with all soft tissue QT autograft demonstrated lower knee extensor strength at 6 months postoperatively compared with male patients. 19 Differences in neuromuscular control between men and women, among other factors, probably contribute to the sex-based strength differences. 20 It is important to also consider the role of autograft type in degree of strength deficit, as larger knee extensor strength deficits occur with the use of QT and BPTB autograft compared with HT autograft.18,27,29 Finally, the influence of patient age on knee extensor strength has been investigated in studies utilizing alternative autograft types, with similar results of lower knee extensor strength being associated with older patient age.21,26
The width of the harvested QT autograft was the only significant associated surgical variable in the final multivariate model of the current study. The size of the harvested autograft has been extensively evaluated specifically in HS autograft, given an association of smaller graft diameter with graft failure.30,39 A proposed benefit of QT autograft, in contrast to HT autograft, is the ability to harvest a graft of sufficient size on a consistent basis. However, the results of this study suggest that QT autograft harvest width, and the subsequent defect in the QT, should be considered carefully when performing ACLR with QT autograft. The depth of the harvested graft, in contrast, was compared using partial thickness and full thickness categories, with both groups demonstrating no difference in knee extensor LSI in the current study. Previous investigations have corroborated the findings of the current study, demonstrating similar outcomes with no difference between full thickness and partial thickness QT autograft. 23 Therefore, the QT autograft harvest morphology and residual tendon defect should possibly be considered when performing ACLR with QT autograft. To obtain a desired graft diameter, harvesting a graft with greater thickness and smaller width may be preferred to preserve quadriceps strength in comparison with harvesting a partial thickness graft of larger width. One potential explanation for the influence on knee extensor strength is that harvest of a wider graft, and subsequent closure of the larger defect, changes the biomechanics of the extensor mechanism and results in decreased efficiency and strength.3,6,16 The implications from graft harvest and residual defect in the QT must be balanced with prevention of graft failure and patient outcomes including quadriceps strength.
Injury characteristics and rehabilitation factors were not associated with knee extensor LSI in the current study. However, the retrospective design of this study requires consideration when interpreting the results, as patients were likely selected for preoperative rehabilitation as well as for BFR during postoperative rehabilitation based on patient factors and surgeon or therapist preference. Without sequential measurements of strength, including preoperative measures, we are unable to determine the starting point for strength as well as change in strength in the early postoperative period. Multiple reports have demonstrated the beneficial role of preoperative rehabilitation before ACLR, including improved knee strength, outcomes, and return to sport.4,11,12 Future investigations on the influence of BFR in specific patient populations should control for patient and surgical factors while also including sequential strength measurements.
There were many factors evaluated in the present study that were not associated with diminished knee extensor LSI. Importantly, time from surgery to isometric strength testing was not correlated with diminished knee extensor LSI, with strength testing being performed between 5 and 12 months postoperatively. Therefore, the confounding effect of time from surgery to strength testing is mitigated despite there being variation in the cohort. This may be due to the dense clustering of this cohort around an approximately 7 month postoperative testing time point, as 50% of patients were tested between 6 and 8.7 months and 75% were tested between 5 and 8.7 months, intervals that could be expected to yield comparable strength testing values in comparison with more distant postoperative testing dates. 22 While debate has surrounded several factors, such as regional anesthesia and tourniquet use during surgery, the results from the present study suggest that these factors do not negatively impact knee extensor LSI after ACLR.2,8,19,34,44 Furthermore, the current study did not find an association with meniscal surgery or the presence of cartilage lesions with knee extensor LSI. These results are similar to other studies showing no influence of meniscal tear/surgery or cartilage damage on knee extensor strength.19,33
Limitations
There are limitations to the study that deserve consideration. First, this study evaluated only knee extensor LSI, which has been shown to overestimate knee function after ACL injury. 43 In addition, the retrospective design of this study with multiple surgeons did not allow for predetermined rehabilitation protocols, which could have influenced the results of the current study. Nevertheless, a general surgical and rehabilitation framework without substantial variation within a single institution was followed. In addition, not all patients in the study had complete PRO data. Because previous studies have found associations between preoperative PROs and outcomes after ACLR, a subset of patients with complete PRO data were analyzed in the current study.35,45 Analysis of the subset of patients with PRO data demonstrated similar findings of age and sex being associated with knee extensor LSI, yet PROs were not associated with knee extensor LSI and did not impact previous associations. Finally, there are variables that were not assessed that could influence the results of the study. In a study of all soft tissue quadriceps ACLR, authors noted that, in addition to female sex, knee extension deficit at 3 months predicted quadriceps LSI at 6 months postoperatively. 19 Due to inconsistencies in range of motion reporting secondary to rater subjectivity, deficits were not assessed, as this study aimed to use objective measures. In addition, higher preoperative strength has been associated with improved postoperative strength and knee function after ACLR.7,21,37 It is important to consider that inclusion of many variables increases the likelihood of a variable being statistically significant just by chance and that variables may be associated with each other. Furthermore, given the relatively small size of this study, conclusions can be drawn only about the specific population from which the sample was drawn. Given the preponderance of true predictor and potential confounder variables that may influence knee extensor LSI after ACLR, there may have been a limited ability of our model to discriminate spurious from true associations; nonetheless, this study posits possible associations to consider when performing QT ACLR. Certainly there remains a need for appropriately designed randomized trials that utilize QT autograft (eg, the STABILITY 2 trial 42 ), which will further elucidate important factors that influence outcomes.
Conclusion
Factors influencing knee extensor LSI after ACLR with QT autograft in this study population spanned patient and surgical factors, including female sex, older age at time of surgery, and wider graft harvest. Surgeons should possibly consider the association between these factors and lower postoperative knee extensor LSI to optimize patient outcomes.
Footnotes
Final revision submitted August 31, 2023; accepted September 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding. J.J.G. has received grant support from Arthrex; education payments from Smith & Nephew, Mid-Atlantic Surgical Systems, and Great Lakes Orthopedics. V.M. has received consulting fees from Smith & Nephew. B.P.L. has received education payments from Mid-Atlantic Surgical Systems. J.D.H. has received grant support from Arthrex, education payments from Mid-Atlantic Surgical Systems and Smith & Nephew, and hospitality payments from SI-BONE. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Pittsburgh (reference No. 19030196).