
Abstract
Background:
Destabilizing shoulder injuries are common in high school American football players; however, the rate of recurrent glenohumeral instability and return to play after arthroscopic labral stabilization surgery remains unknown.
Purpose/Hypothesis:
The purpose of this study was to determine the rate of recurrent instability on return to competitive high school football after arthroscopic shoulder labral stabilization and capsulorrhaphy procedures. It was hypothesized that the instability rate would be greater in players with more years of eligibility remaining (YER) to play at the high school level.
Study Design:
Case series; Level of evidence, 4.
Methods:
Consecutive male high school football players with at least 1 YER who sustained at least 1 anterior traumatic inseason shoulder instability episode and underwent arthroscopic stabilization between 2012 and 2017 were identified. Patients and/or families were contacted by phone to discuss (1) recurrent instability episodes and (2) return to competitive sport and/or recreational athletic activity. Statistical analysis was conducted using chi-square tests to compare recurrent shoulder instability with return to play and YER.
Results:
A total of 45 football players aged 14 to 17 years were included, with a mean follow-up of 4.1 years. Most patients (60%) chose not to return to competitive football, due mainly to fear of recurrent injury. Overall, the recurrent instability rate was 15.6% (7/45). The instability rate in players who returned to football was 16.7%, with 66.7% requiring revision surgery. The instability rate in patients who did not return to football was 14.8%, with no revision procedures required. In players who returned to football, the instability rate in YER group 4 was significantly higher than that in YER groups 1 to 3 (42% vs 10.5%, respectively, P = .03), with each year of play conferring an additional 10% risk of reinjury. There was a significant difference in the type of recurrent instability in players who returned to any sport versus those who did not (P = .029).
Conclusion:
High school football players who returned to competitive play after arthroscopic shoulder stabilization surgery experienced a higher rate of recurrent instability that was dependent on their YER. Over half of the players chose not to return to football, with fear of reinjury being the most common reason.
Keywords
American football is a high-energy contact sport with one of the highest rates of acute shoulder destabilization injuries in high school athletics,3,4,19 conferring increased risk of glenohumeral instability and shoulder girdle injuries in young athletes.6,23 The overall prevalence of shoulder instability has been documented as up to 14% in collegiate football players, with 0.40 injuries reported per 1000 athlete-exposures.12,16 Acute traumatic shoulder instability can range anywhere from sensation of instability to frank glenohumeral dislocation, with subluxations comprising 85% of events in contact athletes.7,17 Depending on the degree of underlying capsulolabral pathology and suspensory complex disruption, shoulder injuries can terminate a season and even the career of a football player.10,13
Arthroscopic labral repair techniques have evolved rapidly as standard of care in surgical candidates to decrease recurrence, mitigate glenohumeral articular injury, and optimize functional outcomes in the context of return to play (RTP).1,2,5 Dickens et al 8 investigated RTP after an index instability event in collegiate military contact athletes with remaining National Collegiate Athletic Association (NCAA) eligibility, demonstrating a recurrence rate of 10% their first year back after an arthroscopic Bankart repair compared with 60% in the nonoperative cohort. Patients younger than 25 years old were evaluated prospectively after arthroscopic capsulolabral repair for isolated anterior instability and demonstrated an overall rate of RTP of 87% at final follow-up, with 6 of 58 patients returning to less competitive activities than preinjury level. 18 High school football players similarly constitute a high-risk population for destabilizing shoulder pathology; however, there is a paucity of literature investigating operatively managed high school football players. 22 The rate of recurrence and career longevity in high school patients who return to football after arthroscopic stabilization remains unknown.
The purpose of this study was to determine the risk of recurrent shoulder instability after arthroscopic labral repair in high school athletes on return to competitive football. The hypothesis was that the rate of recurrent shoulder instability would be greater in players with increasing years of eligibility (YER).
Methods
After institutional review board approval was obtained, we conducted a retrospective chart review for patients who were clinically indicated for, and underwent, arthroscopic labral repair procedures at our institution between 2012 and 2017. Inclusion criteria were adolescent male athletes aged 14 to 18 years who had sustained at least 1 anterior traumatic shoulder instability event during high school football practice or game play. Instability characteristics included acute or recurrent, uni- or multidirectional, and subluxation or dislocation. For the purposes of this study, subluxation was defined as a transient glenohumeral translational event without requirement for manual reduction. 24 Dislocation was defined as glenohumeral articular incongruency on subjective, clinical, and/or radiographic evaluation typically requiring manual reduction. A player was included in the instability cohort if he had participated in competitive team practice and/or game play. Excluded were patients below the 8th grade or above the 11th grade and those unable to be contacted by telephone for interview. As part of this study, we calculated the YER, defined as the seasons of eligibility for return to high school football after the instability event. For example, 8th graders were credited with 4 YER, and 11th graders were credited with 1 YER. Therefore, athletes who sustained an instability event and/or underwent surgery during their final year of high school were not included in this study.
Surgical Technique
All surgeries were conducted by 2 orthopaedic sports surgeons (A.T.P. and E.W.E.) at a single institution. Arthroscopic capsulolabral reconstruction was performed with the patient in a lateral decubitus position with posterior and anterosuperior viewing portals, an anterior working portal, and percutaneous portal placement at the 5-o’clock position. An anchor was placed roughly at every clockface position of the labral tear, with a minimum number of 3 anchors placed. Before anchor placement, the labral tear was debrided of unstable/unsalvageable tissue, the glenoid neck was prepared to expose bleeding cancellous bone, and anchors were placed at the labro-articular junction per standard technique.
Postoperative Management
The postoperative rehabilitation protocol involved placing the patient in a shoulder immobilizer for 2 weeks followed by transition to a sling for an additional 4 weeks to protect from excessive early activity. Patients began performing pendulum swings during the sling phase, progressing to formal physical therapy with passive and active-assisted range of motion. Once 80% range of motion was achieved (usually 6-8 weeks postoperatively), strength rehabilitation was initiated until >80% of strength and >90% of range of motion were achieved. Patients were typically released to full activity including contact sports at 6 months postoperatively.
Data Collection
Athletes were followed though subsequent competitive seasons after the index instability event and shoulder stabilization surgery. Patients and/or families were contacted by phone to discuss (1) postoperative pain, (2) recurrent instability per aforementioned criteria, (3) return to football, (4) return to noncontact activity, and (5) subjective shoulder postoperative function. If the patient did not return to competitive football, then they were asked an open-ended question: “Why did you not return to football after surgery?” The various responses were recorded: fear of return, parental/family concerns with the sport in general, shift to recreational athletics, weightlifting, general academic pursuits, and pursuit of noncontact activities. All data collection and interviews were conducted by a single orthopaedic surgery resident (J.R.S.) with a structured interview script to circumvent interobserver variability. 9
Statistical Analysis
Statistical analysis was conducted using chi-square hypothesis testing to compare groups regarding recurrence of instability with return to sport. All analyses and comparisons were performed using SPSS (Version 25; IBM Corp) with a type 1 error rate of P < .05 to declare significance.
Results
Patient Demographics
Of 64 patients who met the inclusion criteria, 45 patients were available for survey completion and included in the analyses. The 19 patients not included in analyses could not be reached or were lost to follow-up. The mean age of the included athletes was 15.5 years (range, 14-18 years), with a mean follow-up time of 4.1 years (range, 1-8 years). The most common football position among high school players undergoing surgical stabilization for shoulder instability was linebacker at 26% of the cohort, followed by wide receiver at 16%. We elected to not record the other positions because they were so varied, many of the athletes played multiple positions, and some could not recall the position they injured themselves at the time of the survey.
Return to Football
Overall, 40% (18/45) of high school football players returned to competitive football after arthroscopic shoulder stabilization. Of the remaining 60% (27/45) of patients who did not return to football, the overwhelming reason, reported by 93% of the nonreturners (25/27), was fear of recurrence, despite no recurrent shoulder instability reported in this subgroup. All patients in this subgroup of nonreturners also described a volitional change to at least 1 of the following pursuits in lieu of return to football: noncontact sport, recreational athletics, weightlifting, or general academics. Noncontact activities included but were not limited to baseball, 11 running, weightlifting, and yoga.
Recurrent Instability
The overall rate of recurrent instability on release to full activity was 15.6% (7/45). The majority of recurrent instability events occurred during high school football. The rate of instability in football players who returned to competitive play was 16.7% (3/18) compared with nonreturners at 14.8% (4/27) (P = .87). Of the 3 patients who sustained recurrent instability events after return to football, 2 required revision procedures (66.7%), whereas no nonreturners with recurrent instability underwent a second operation (0%; P = .14). One of the patients who underwent revision returned to collegiate-level football, while the other patient discontinued all high school contact sports including football. Furthermore, we found that those patients with recurrent instability who had returned to competitive football experienced it as a “dislocation” event, whereas the patients with recurrent instability who did not return to football only experienced a sensation of “subluxation” without frank dislocation (Table 1). In a subgroup analysis of patients who returned to any high school sport, a statistically significant difference was observed regarding type of recurrent instability (P = .029) (Table 2). Of the patients who did not return to football, 18.5% (5/27) changed to a competitive noncontact sport during high school (most commonly baseball), with no recurrent instability events reported.
Recurrent Instability Events in Patients who Returned to High School Football Versus Nonreturners a

There was no significant difference between returners to football and nonreturners regarding type of recurrent instability (P = .065).
Recurrent Instability Events in Patients who Returned to any High School Sport Versus Nonreturners a
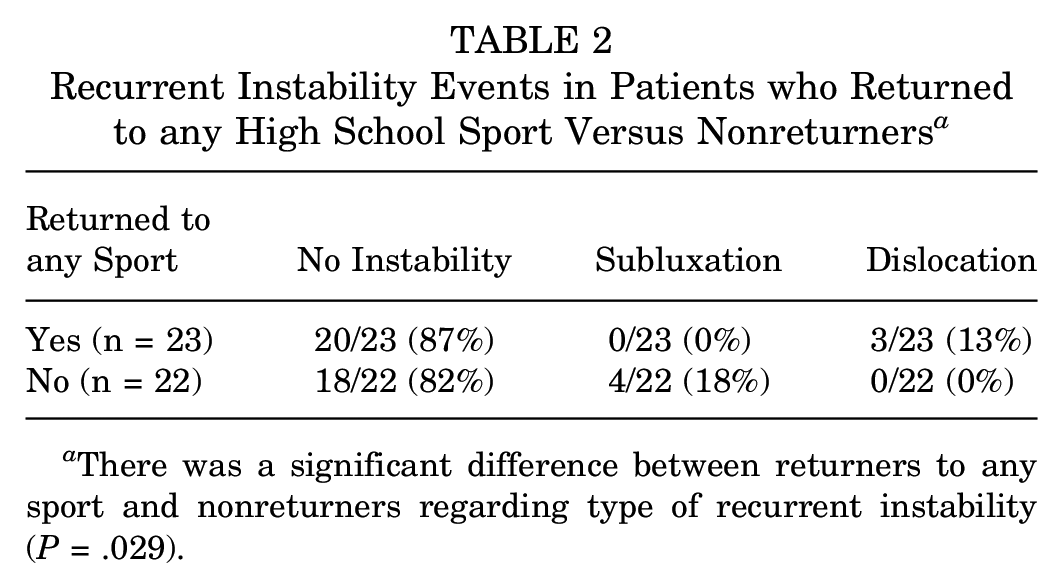
There was a significant difference between returners to any sport and nonreturners regarding type of recurrent instability (P = .029).
Years of Eligibility Remaining
A positive association was observed in high school football players based on YER (Table 3), with the highest rate of recurrence in the youngest group (YER = 4). Of the high school players who returned to football after surgery, there was an approximately 10% increase in risk of recurrence for each additional year of YER remaining. The 42% rate of recurrent instability in YER group 4 was significantly higher than the overall rate of recurrent instability in YER 1 to 3 (10.5%; P = .03) (Table 3).
Number of Recurrent Instability Events Stratified by YER a

YER, years of eligibility remaining.
Discussion
The purpose of this study was to investigate the rate of recurrent instability after arthroscopic management of destabilizing inseason shoulder injuries in high school football players.8,14 As expected, patients returning to high school football after surgical stabilization demonstrated a higher rate of recurrent instability requiring revision procedures when compared with patients who transitioned to noncontact sports, recreational activities, or academic studies. Our hypothesis that increasing YER would be associated with increased rates of secondary postoperative instability events after RTP was also confirmed, as the years of high school remaining for younger athletes afforded a greater number of high-risk exposures that may predispose to surgical failure. Thus, informed shared decision-making is especially important for players early in their career (higher YER) with a greater number of expected exposures. Awareness of a correlation between school year and risk of recurrence in young contact athletes who return to high-energy collision game play may guide individualization of perioperative counseling toward the optimization of functional outcomes. While YER refers to high school athletics in the current study, eligibility may similarly affect collegiate, recreational club, or even professional football players.
Unexpectedly, only 40% of high school football players returned to football after surgery. The main driving factor for more than half of the study patients not returning to competitive football was the fear of repeat injury. We found that fear of recurrence was a powerful deterrent in the return to contact sports after shoulder surgery, often accompanied by patient and familial concern for long-term functional implications of further shoulder injuries. Although we recognize and admire the motivational factors that drive young athletes to return to football after shoulder surgery, the widespread fear of recurrence in our cohort (reported by 93% of the nonreturners) reflects a valid concern and consideration in the management of young athletes. 15 Therefore, return to high school football after shoulder arthroscopy requires expectation management with the patient and family.
Patients who hang up their football cleats, however, often transitioned to alternative noncontact or recreational activities. We observed the statistically significant and clinically meaningful finding that patients who elected to transition from competitive high school football to noncontact sport were less likely to experience recurrent instability events. There was no statistically significant difference in the number of patients who experienced recurrent instability after return to football as compared with nonreturners; however, there were increased rates of recurrent complete dislocations and revision procedures among those who returned to football. The collision intensity in football confers heightened risk of recurrent injuries, need for repeat procedures, extended rehabilitation periods, and potential long-term functional sequelae as described in the collegiate literature and corroborated in our novel study in the high school population. 20 While it remains unknown whether patients would have recurrent instability if they gave up football, we suspect these findings may guide perioperative counseling of patients and families in the context of multifaceted clinical decision-making.
Limitations
There are several limitations to the current study, including the inherent restrictions of a retrospective study design involving a telephone survey. The small sample size due to narrow inclusion criteria, loss to follow-up, and inability to reach patients or families despite various contact modalities also limited the power of statistical analysis. Furthermore, our data collection was susceptible to interview, response, and transfer biases associated with telephone interviews. The inability to interview all subjects directly introduces the risk of recall bias associated with interviewing families on behalf of the patient, which precluded quantitative functional scores. There was limited information available in the medical records regarding extremity dominance, ligamentous laxity, and multiplicity of instability events before operative injury. Additional limitations include the lack of reported surgical technique factors including number of anchors, degree of labral injury, and presence of bone loss. With regard to bone loss, Rossi et al 21 found that arthroscopic Bankart repair in competitive rugby players was associated with a significantly higher rate of recurrence (20% vs 4%) as well as reoperation (16% vs 4%) than the Latarjet procedure. Future studies should investigate functional outcomes and recurrent instability after the Latarjet procedure in the high school population. Strengths of the study include a 70.3% response rate and mean follow-up time sufficient to capture recurrent instability events after surgery during the remaining high school career.
Conclusion
Overall, we observed favorable surgical outcomes with relatively low rates of recurrent instability after surgery in the study cohort such that arthroscopic labral repair remains a favorable management option in young high-level athletes. Future improvements in clinical practice management may involve measures to address fear of RTP such as multidisciplinary counseling while continuing to optimize surgical technique and functional outcomes to allow patients to safely return to sport.
Footnotes
Final revision submitted September 11, 2023; accepted September 18, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.R.S. has received education payments from ImpactOrtho and SportsTek Medical and hospitality payments from Stryker. E.W.E. has received education payments from Elevate Surgical and nonconsulting payments from Arthrex. A.T.P. has received education payments from ImpactOrtho and SportsTek Medical and consulting fees from OrthoPediatrics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California, San Diego (reference No. 170519X).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.