
Abstract
Background:
Anterior cruciate ligament (ACL) tears are commonly seen with concomitant injuries to the posterolateral tibial plateau, while the occurrence of ACL injuries in posterolateral tibial plateau fractures (PTPFs) remains unclear.
Purpose:
To (1) explore the incidence of knee ligament (anterior or posterior cruciate ligament, medial or lateral collateral ligament) and medial or lateral meniscus injuries in patients with PTPF and (2) find reliable PTPF-related parameters to predict the risk of knee ligament and meniscal injuries.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Patients diagnosed with PTPF who had computed tomography and magnetic resonance imaging (MRI) data were identified. Morphological parameters of the PTPF were measured on sagittal computed tomography images. Knee ligament and meniscal injuries were assessed using MRI. The association of ACL injuries with meniscal injuries was analyzed. Receiver operating characteristic (ROC) analysis was used to determine the value and cutoff point of the PTPF morphological parameters for diagnosing complete in-substance ACL tears.
Results:
Overall, 113 patients with PTPF were included. ACL injuries were present in 94 (83.2%) patients, including 43 (38.1%) avulsion fractures and 28 (24.8%) complete in-substance tears. Patients with in-substance ACL tears had a higher incidence of lateral meniscus posterior horn tears compared with the other patients (PBonferroni < .001). ROC analysis revealed that both the fracture depression angle (cutoff point, 25.5°) and the posterior articular surface loss percentage (cutoff point, 37.5%) had a sensitivity >90% and a specificity >80% for the diagnosis of complete in-substance ACL tears.
Conclusion:
ACL injuries were seen in 83.2% of the study patients. Complete in-substance ACL tears were associated with an increased incidence of lateral meniscus posterior horn tears. Among PTPF parameters, fracture depression angle and posterior articular surface loss percentage showed a high predictive value for the presence of complete in-substance ACL tears, thereby reducing delays in diagnosis and treatment.
Posterolateral tibial plateau fractures (PTPFs) account for approximately 15% of all tibial plateau fractures and are closely associated with knee ligament and meniscal injuries.33,37 In general, the primary aim in surgical treatment of PTPF is to obtain a congruent knee joint with adequate stability allowing for early range of motion exercise. Despite a variety of approaches and fixation methods for optimizing the prognosis of PTPF,7,30 there are few studies on accompanying knee ligament and meniscal injuries. In clinical work, the management of tibial plateau fractures and soft tissue injuries also tends to be clearly divided, with the 2 not forming a holistic solution like the Lauge-Hansen classification system for the time being. 16
With the evolution of treatment concepts and imaging technologies in recent years, knee ligament and meniscal injuries related to tibial plateau fractures have drawn increased attention from orthopaedic surgeons. The force causing a PTPF can pose a threat to knee soft tissue, especially the anterior cruciate ligament (ACL), as corroborated by the connection between PTPF and ACL injury.2,17,33 Although there is no consensus on the role of knee ligament and meniscus in the management of PTPFs, joint instability has been found in certain PTPFs in cases of knee ligament and meniscal injuries.4,18 A few researchers have suggested that knee ligament and meniscal injuries should be considered as one of the key determinants when selecting therapeutic strategies for PTPFs.17,33 Thus, investigations on associated knee ligament and meniscal injuries in PTPFs can assist surgeons in gaining a complete picture of the overall injury, thereby helping develop holistic solutions for these injuries.
The incidence of PTPF in individuals with ACL tears has been shown in sports medicine studies,2,14 yet there are no large-sample studies on associated knee ligament and meniscal injuries in PTPFs with both computed tomography (CT) and magnetic resonance imaging (MRI) data. Given the lack of MRI data or arthroscopic records, most morphological studies investigating tibial plateau fractures have been unable to identify ligament in-substance tears.11,38 Therefore, the objectives of this study were to (1) explore the incidence and characteristics of knee ligament (anterior or posterior cruciate ligament, medial or lateral collateral ligament) and medial or lateral meniscus injuries in patients with PTPF and (2) find reliable PTPF-related parameters to predict the risk of knee ligament and meniscal injuries. We hypothesized that the morphological characteristics of PTPF could be used to predict associated knee ligament and meniscal injuries.
Methods
Participants
The protocol for this study received institutional review board approval; the need for informed consent from participants was waived. We conducted a search in the picture archiving and communications system at a level 1 trauma center for CT data on patients diagnosed with the keywords “tibia” and “fracture” between January 2019 and August 2022. We first identified individuals with tibial plateau fractures. The following criteria were used for exclusion: (1) postoperative CT of fractures; (2) interval between CT and fracture >3 weeks; (3) other fractures that were not tibial plateau fractures; (4) polytrauma with an injury severity score >16; (5) open or pathological fractures; (6) fractures concomitant with an ipsilateral tibial shaft, femoral, or patellar nonavulsion fracture; and (7) skeletal immaturity (age, <16 years). Consecutive patients with PTPF (defined as an isolated posterolateral column fracture 34 ) who were treated at our department were subsequently screened, and patients without available MRI scans were excluded. Ultimately, 113 knees in 113 patients were deemed eligible for this study. All patients had a fracture of the 41-B type according to the AO Foundation/Orthopaedic Trauma Association (AO/OTA) classification. The patient inclusion process is shown in Figure 1.
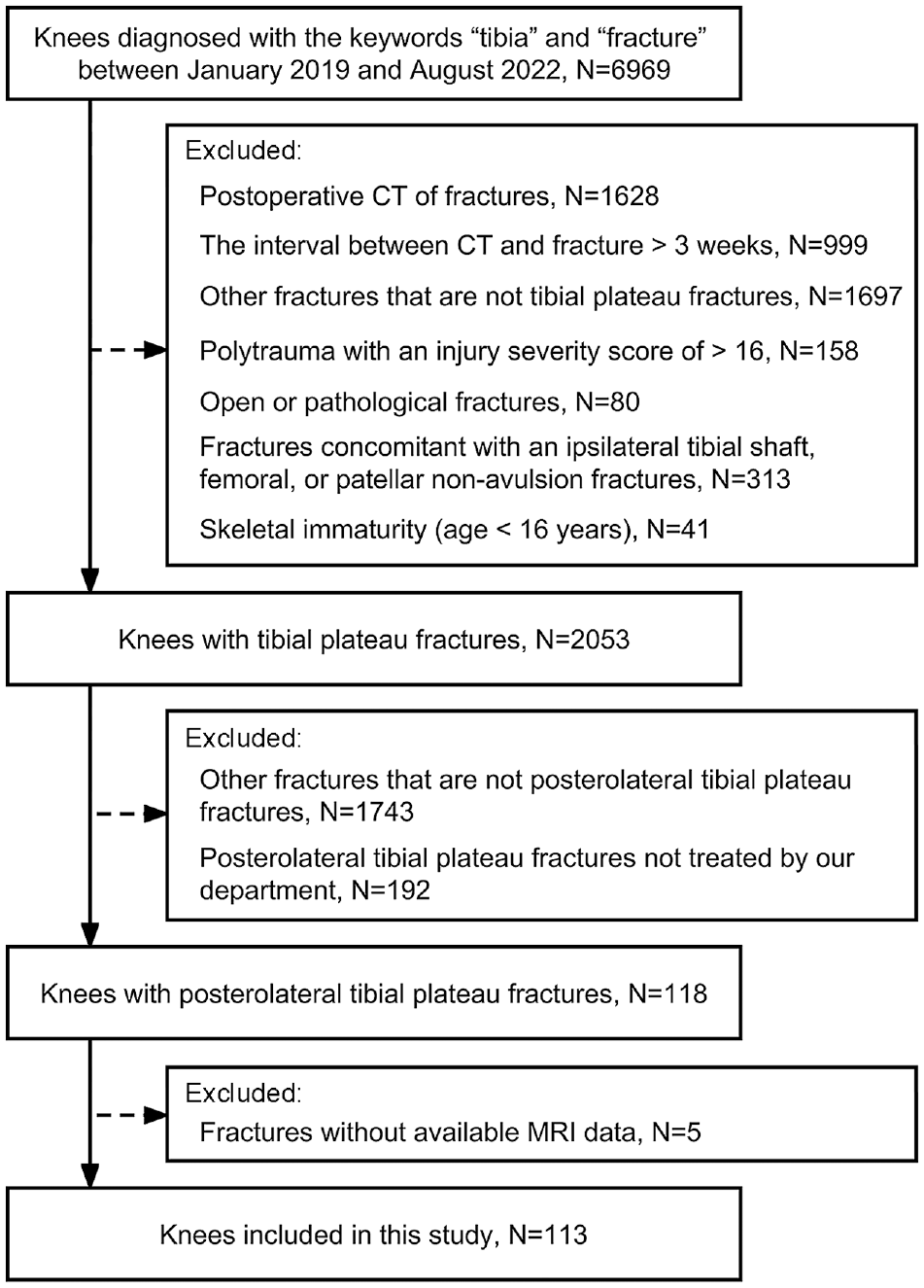
Flowchart demonstrating patient exclusion and inclusion. CT, computed tomography; MRI, magnetic resonance imaging.
Measurement of PTPF Parameters
The CT imaging data were acquired from a picture archiving and communication system workstation and subsequently imported into RadiAnt DICOM viewer (Version 2021.2; Medixant) for analysis. The morphometric parameters of the PTPF were measured with reference to the method described by Bernholt et al. 2 The CT sagittal slice at the 50th percentile of the lateral tibial plateau width was selected for measurement (Figure 2). Line A was drawn first along the articular surface from the anterior to the posterior aspect; line B was then drawn vertically perpendicular to this line and tangent to the most posterior aspect of the proximal tibia. The point at which line A intersects line B was noted as point O. The fracture edge sites on lines A and B were denoted as P and Q, respectively. The point at the most anterior edge of the joint surface on line A was noted as R. The line passing through points P and Q was recorded as line C. The ratio of the distance between points P and O to the distance between points R and O was defined as posterior articular surface loss percentage. The distance between points Q and O was recorded as the articular surface depression depth. The angle between lines A and C was defined as fracture depression angle.

Measurement of posterolateral tibial plateau fracture morphological parameters. Posterior articular surface loss percentage was defined as the ratio of the distance between points P and O to the distance between points R and O. Articular surface depression depth is recorded as the distance between points Q and O. Fracture depression angle is defined as the angle between lines A and C.
The distance between points P and O, the distance between points R and O, the articular surface depression depth, and the fracture depression angle were measured by 2 reviewers (B.Z. and Y.W.) who were blinded to the patient information.
Measurement of Ligament and Meniscal Injuries on MRI
The MRI data were obtained following a standard imaging protocol using a 3.0-T scanner. We employed T1-weighted, T2-weighted, and proton density–weighted sequences to measure knee ligament and meniscal injuries. Ligament injuries included avulsion fractures, complete in-substance tears, and partial in-substance tears. Avulsion fractures referred to those of the tibial or femoral ligament footprint. A complete in-substance tear was defined as the complete disruption of ligamentous fibrous tissue continuity, whereas a partial in-substance tear was described as partial continuity of local ligamentous fibrous structures with an enhanced high signal on T2-weighted images.13,28,33,39 Increased signal intensity within the meniscus is the hallmark of meniscal imaging pathology, which ranges in grading from 1 to 4. 29 Only grade 3 and 4 lesions were considered indicators of meniscal tears in this investigation.
Two senior physicians (Y.Z. and X.X.), both with expertise in musculoskeletal radiology, analyzed the MRI data and used a panel consensus discussion to resolve disagreements. Both reviewers were blinded to the patient information.
Statistical Analysis
Descriptive statistics were used for demographic data and the incidence of knee ligament and meniscal injuries. The Shapiro-Wilk test was used to evaluate the normality of continuous data. Comparisons of continuous data between groups were performed using 1-way analysis of variance (normal distribution), the Mann-Whitney U test (nonnormal distribution), or the Kruskal-Wallis test (nonnormal distribution). Comparisons of categorical data between groups were performed with the chi-square test. The correlation between ACL injuries and meniscal injuries was analyzed by the Fisher exact test.
The intraobserver and interobserver reliability for the PTPF measurements were determined with the intraclass correlation coefficient (ICC), in which the 2 reviewers who conducted the measurements (B.Z. and Y.W.) independently measured 40 randomly selected cases twice with an interval of 2 weeks between the measurements. ICCs ≥0.75 were defined as good and those of 0.50 to 0.74 as moderate. 26 The intraobserver and interobserver reliability of the ligament and meniscal injuries was determined using the Cohen kappa (κ), in which the 2 reviewers who conducted the measurements (Y.Z. and X. X.) independently reviewed 40 randomly selected cases twice with an interval of 2 weeks between review. The κ values were interpreted according to the guidelines proposed by Landis and Koch. 15
In patients without ACL avulsion fractures, receiver operating characteristic (ROC) curves were built to determine the diagnostic value of the PTPF morphological parameters for complete in-substance ACL tears, and the areas under the ROC curves (AUCs) were measured to evaluate diagnostic accuracy. The cutoff values for the parameters were determined by the maximum Youden index (sensitivity+specificity– 1).
All statistical analyses were performed using SPSS (Version 26.0; IBM Corp). Statistical significance was set at P < .05. Bonferroni adjustments were performed for multiple comparisons.
Results
The study population (N = 113) comprised 48 male and 65 female patients, with 60 cases affecting the left side and 53 cases affecting the right side. The patients were all ethnic Han Chinese, with a mean age of 42.4 years (range, 18-85 years). Overall, 98 (86.7%) patients showed evidence of knee ligament and meniscal injuries around the knee. The incidence of ligament and meniscal injuries according to patient age, sex, and fracture side is shown in Table 1.
Knee Ligament and Meniscal Injuries Overall and Stratified by Patient Age, Sex, and Fracture Side a
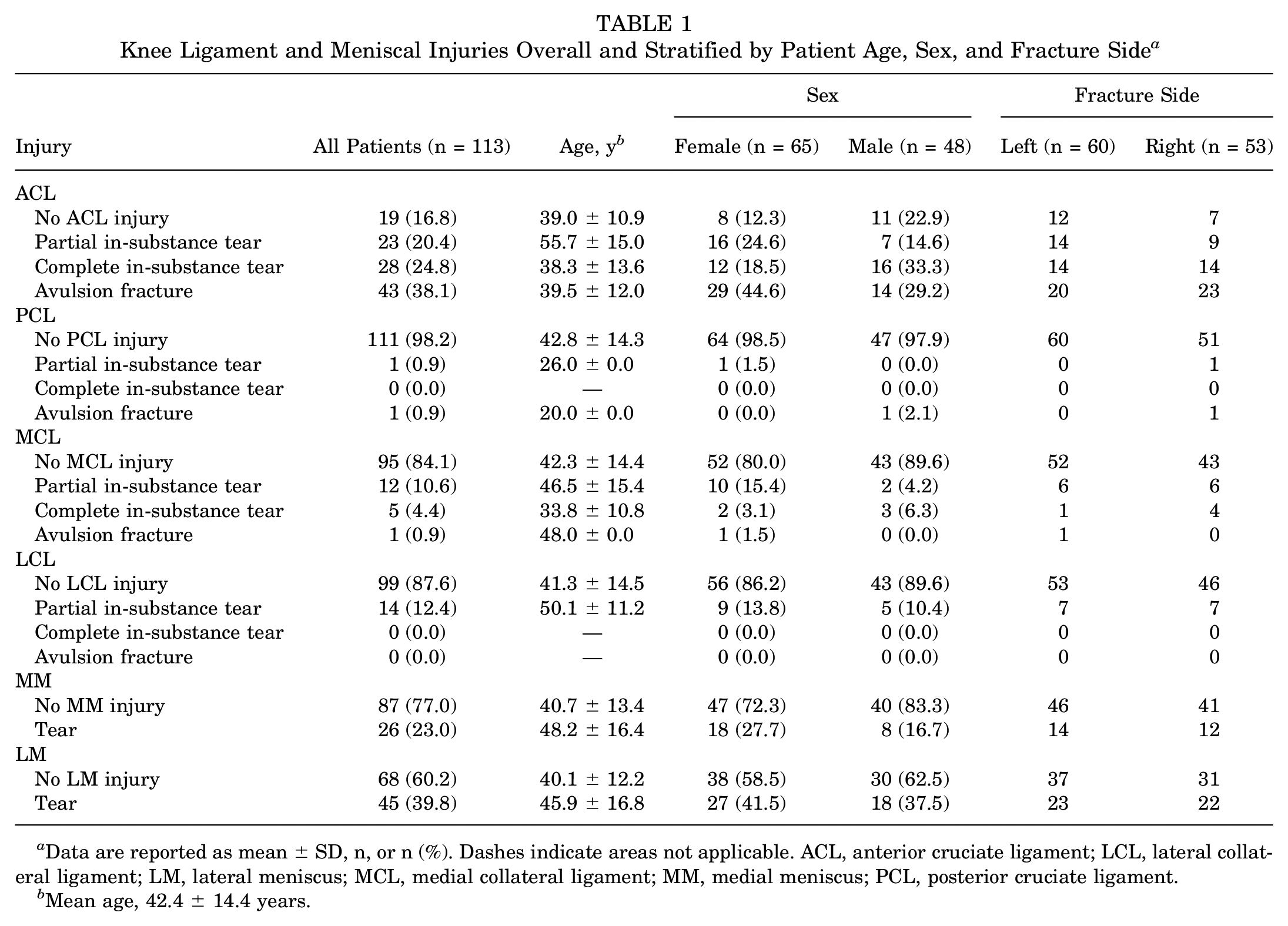
Data are reported as mean ± SD, n, or n (%). Dashes indicate areas not applicable. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; LM, lateral meniscus; MCL, medial collateral ligament; MM, medial meniscus; PCL, posterior cruciate ligament.
Mean age, 42.4 ± 14.4 years.
The intraobserver and interobserver reliability of the PTPF measurements were good (ICC, ≤0.833; 95% CI, 0.706-0.908) (Appendix Table A1). The intraobserver and interobserver reliability for the identification of ACL injuries and lateral meniscus (LM) posterior horn tears was almost perfect (κ≤ 0.827), and intraobserver and interobserver reliability for the identification of other injuries showed at least substantial agreement (Appendix Table A2).
Incidence of Cruciate Ligament Injuries
ACL injuries were the most frequent soft tissue injury (83.2%). For patients with PTPF, the group with partial in-substance ACL tears was older (PBonferroni < .05 for all). There were no significant sex-based differences in the incidence of cruciate ligament injuries. No significant differences were found between the injury pattern of the ACL and those of other ligaments (Appendix Table A3). Notably, the incidence of LM posterior horn tears was higher in patients with complete in-substance ACL tears than in all other patients (60.7% vs 16.5%; PBonferroni < .001) (Table 2).
Association Between ACL Injury Patterns and Meniscal Tear Patterns a
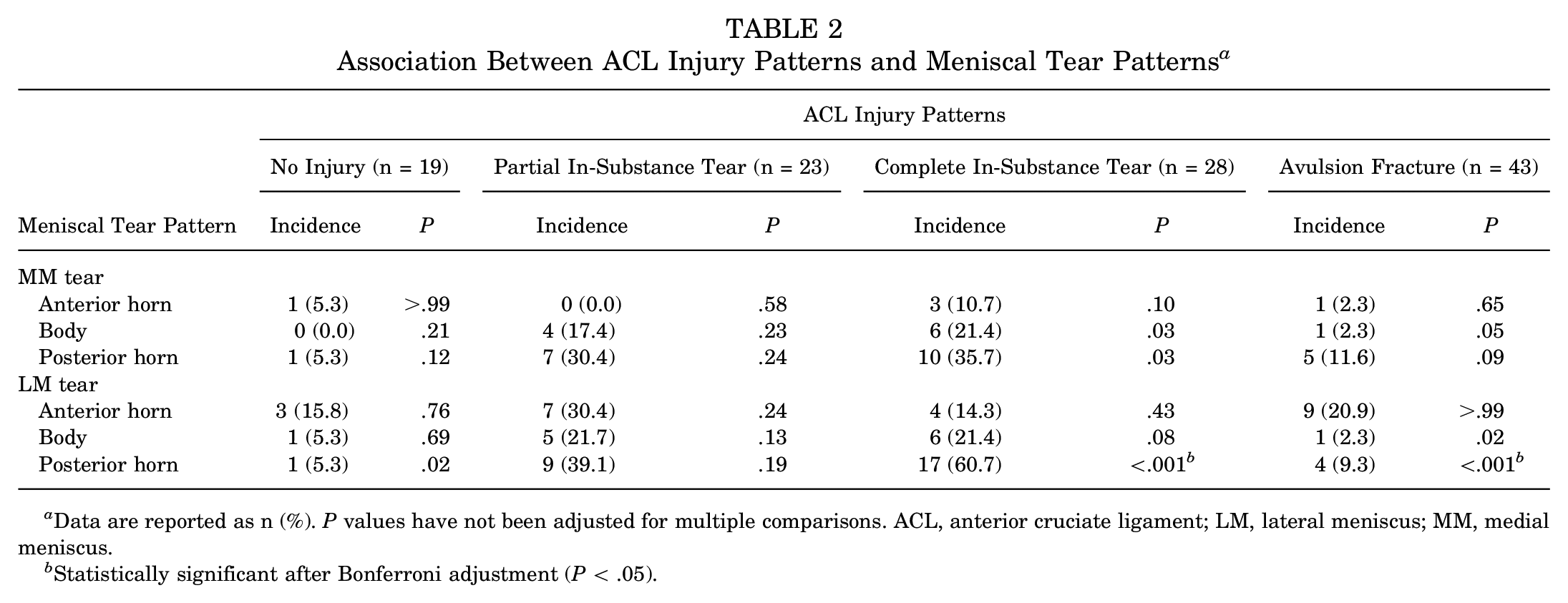
Data are reported as n (%). P values have not been adjusted for multiple comparisons. ACL, anterior cruciate ligament; LM, lateral meniscus; MM, medial meniscus.
Statistically significant after Bonferroni adjustment (P < .05).
Incidence of Collateral Ligament Injuries
Patients with LCL injuries were younger than those who were not injured (P = .02). No statistical differences were found in the age distribution among MCL injury types (P = .38). There were no significant sex-based differences in the incidence of collateral ligament injuries.
Incidence of Meniscal Tears
The LM posterior horn had the highest rate of meniscal tears (27.4%) (Figure 3). The group with MM tears was older (P = .05); however, there was no statistical difference in the age distribution between LM tears or not (P = .12). The incidence of meniscal tears showed no difference between the sexes.

Incidence of tears in different regions of the meniscus.
Analysis of PTPF Parameters
The ROC analysis indicated that 2 PTPF parameters, the fracture depression angle and the posterior articular surface loss percentage, were favorable for the diagnosis of complete in-substance ACL tears, with AUCs of 0.956 and 0.917, respectively (Figure 4 and Table 3). The cutoff value for the fracture depression angle was 25.5° (sensitivity, 96.4%; specificity, 81.0%), and the cutoff value for the posterior articular surface loss percentage was 37.5% (sensitivity, 96.4%; specificity, 81.0%).

Receiver operating characteristic curves showing the area under the curve (AUC) for fracture depression angle and posterior articular surface loss percentage.
Diagnostic Performance of the Parameters a
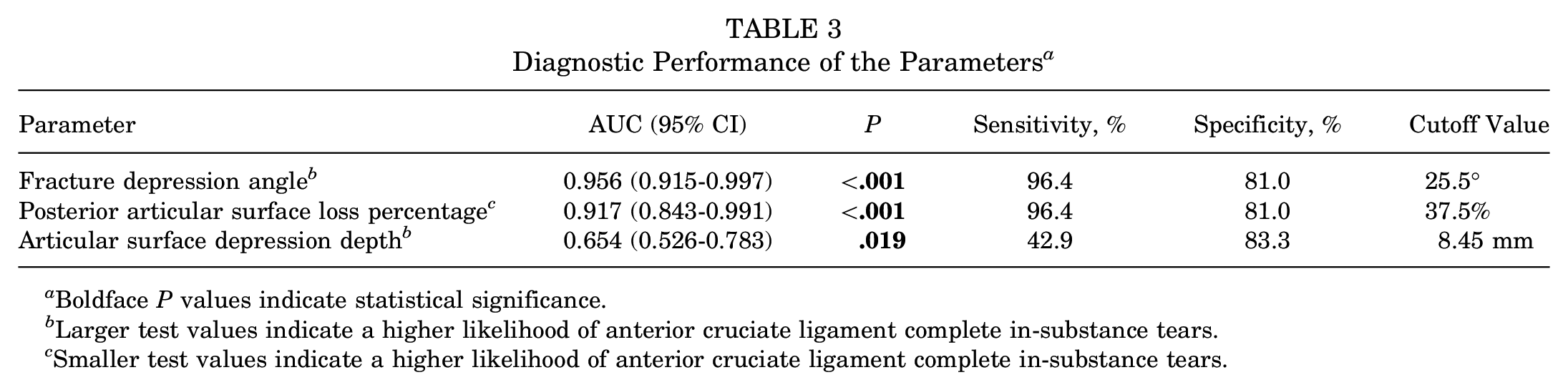
Boldface P values indicate statistical significance.
Larger test values indicate a higher likelihood of anterior cruciate ligament complete in-substance tears.
Smaller test values indicate a higher likelihood of anterior cruciate ligament complete in-substance tears.
Discussion
In this study, the largest series of PTPFs combining CT and MRI to date, the ACL had the highest frequency of injury among the soft tissues investigated. Avulsion fractures were the most common type of ACL injuries (38.1% of patients), followed by complete in-substance tears (24.8% of patients). The incidence of LM tears was 39.8%, second only to ACL injuries, and patients with in-substance ACL tears had a significantly higher incidence of LM posterior horn tears compared with the other patients (PBonferroni < .001). Finally, ROC analysis indicated that in patients with PTPF, a posterior articular surface loss percentage <37.5% and fracture depression angle >25.5° on CT suggested a high risk of complete in-substance ACL tears.
It has been demonstrated that patients with ACL tears frequently present with posterolateral bone bruises or occult fractures.5,14,20 As a result, posterolateral knee bone bruises have consistently been identified as an indirect indicator of an ACL tear. Based on a study of 825 knees, Bernholt et al 2 reported that PTPFs caused by impaction occurred in 49.3% of patients with an ACL tear. In a flexed knee with a noncontact ACL tear, anterior tibial translation and knee valgus allow the lateral femoral condyle to impact the posterolateral tibial plateau, resulting in bone bruises or even fractures, which is a reasonable inference from the studies of patients with ACL injuries.23,36,41 Nevertheless, the specifics of ACL damage in patients with PTPF remain unclear at present. For this reason, we conducted this study to provide a complementary description of the aforementioned flexion valgus injury from the fracture standpoint rather than the soft tissue standpoint, which could assist orthopaedic trauma surgeons in grasping the overall injury in terms of both bone and soft tissue.
Several studies have proposed that distinct fracture patterns and soft tissue injuries can arise from specific injury mechanisms involving forces and knee positions.11,24,38,42 In 2016, Wang et al 33 observed 20 cases of ACL injuries in 25 fractures involving the posterolateral tibial plateau, but the varying fracture patterns suggested that they resulted from different injury mechanisms. According to the injury mechanism, the proportion of each injury pattern in the study population may have influenced the observed incidence of knee ligament and meniscal injuries. For instance, if certain injury patterns are more prevalent in the study population, the incidence of knee ligament and meniscal injuries associated with those patterns will be overrepresented in the findings. To obtain an unambiguous incidence of knee ligament and meniscal damage, all PTPFs in this study referred to isolated PTPFs. We found that the incidence of ACL injuries in PTPFs was as high as 83.2%, which is even higher than the incidence of ACL injuries in tibial plateau fractures in most previous studies.1,6,9,31 Furthermore, our study showed an incidence of 20.4% for LM anterior horn tears and 27.4% for LM posterior horn tears, which might result from the pull-out force and impact force on the meniscus from the lateral femoral condyle, respectively, during the injury process. 3 Overall, PTPFs, ACL injuries, and LM tears are closely coupled in the flexion valgus injury pattern that requires special attention.
Without a fundamental understanding of ACL injuries in patients with PTPF, the diagnosis of complete in-substance ACL tears can be readily missed. 22 The incidence of complete in-substance ACL tears remained 40.0% after excluding ACL avulsion fractures in this study. Furthermore, patients with complete in-substance ACL tears in this study had a higher incidence of LM posterior horn tears than all other patients. It is noteworthy that the combination of complete in-substance ACL tears and LM posterior horn tears has been associated with a high-grade pivot-shift phenomenon. 19
To avoid underdiagnosis of knee ligament and meniscal injuries, initial CT screening of PTPF morphological features for patients with a high risk of soft tissue injuries is valuable. In a study of 31 individuals with PTPF, Yang et al 40 showed that ACL injuries were more likely to occur when the articular fragment inclined posteriorly. In the current study, we found that posterior articular surface loss percentage and fracture depression angle can help identify complete in-substance ACL tears in individuals with PTPF, adding quantitative indicators for these parameters.
There is still no consensus on the treatment options for the combination of PTPF and ACL injury. Several studies have advocated early fixation of ACL avulsion fractures along with tibial plateau fractures,1,10,33,40 but the treatment protocol for ACL tears in PTPFs remains controversial. In the past, researchers have recommended deferred treatment of ACL tears in tibial plateau fractures.1,25 However, some case reports have illustrated the technical feasibility of simultaneous surgical management of PTPF and ACL tear.12,21,35 Menzdorf et al 17 reported that surgical treatment of PTPF combined with ACL repair or reconstruction is a safe procedure and reported good short-term clinical outcomes in a limited sample of patients. Moreover, specific types of PTPF combined with ACL tear have been noted to affect not only pivot-shift laxity under anesthesia but also the postoperative outcomes of ACL reconstruction.4,8 Given the close association between fractures and ACL injuries with knee osteoarthritis,27,32 a holistic solution that addresses both factors is needed.
Limitations
There are limitations in this study. First, while MRI is the most commonly used diagnostic tool for knee ligament and meniscal injuries, it has a certain false-positive rate. Second, this study did not include follow-up results. Because it is currently unknown whether knee ligament and meniscal injury in patients with PTPF affects the stability and functionality of the knee over the long term, our future research will investigate this issue.
Conclusion
The incidence of ACL injuries in PTPF was as high as 83.2%, and complete in-substance ACL tears were associated with an increased incidence of LM posterior horn tears. Fracture morphological features such as the fracture depression angle and the posterior articular surface loss percentage can be used to predict complete in-substance ACL tears, thereby reducing delays in diagnosis and treatment.
Footnotes
Appendix
Associations Between ACL Injury Patterns and Other Ligament Injury Patterns a

| Injury Patterns of Other Ligaments | ACL Injury Patterns | |||||||
|---|---|---|---|---|---|---|---|---|
| No Injury (n = 19) | Partial In-Substance Tear (n = 23) | Complete In-Substance Tear (n = 28) | Avulsion Fracture (n = 43) | |||||
| Incidence | P | Incidence | P | Incidence | P | Incidence | P | |
| PCL | ||||||||
| Partial in-substance tear | 0 (0.0) | >.99 | 0 (0.0) | >.99 | 0 (0.0) | >.99 | 1 (2.3) | .14 |
| Complete in-substance tear | 0 (0.0) | — | 0 (0.0) | — | 0 (0.0) | — | 0 (0.0) | — |
| Avulsion fracture | 0 (0.0) | >.99 | 0 (0.0) | >.99 | 0 (0.0) | >.99 | 1 (2.3) | .14 |
| MCL | ||||||||
| Partial in-substance tear | 0 (0.0) | .21 | 2 (8.7) | >.99 | 6 (21.4) | .07 | 4 (9.3) | >.99 |
| Complete in-substance tear | 0 (0.0) | .59 | 0 (0.0) | .58 | 3 (10.7) | .10 | 2 (4.7) | >.99 |
| Avulsion fracture | 0 (0.0) | >.99 | 0 (0.0) | >.99 | 0 (0.0) | >.99 | 1 (2.3) | .38 |
| LCL | ||||||||
| Partial in-substance tear | 1 (5.3) | .46 | 3 (13.0) | >.99 | 4 (14.3) | .75 | 6 (14.0) | .77 |
| Complete in-substance tear | 0 (0.0) | — | 0 (0.0) | — | 0 (0.0) | — | 0 (0.0) | — |
| Avulsion fracture | 0 (0.0) | — | 0 (0.0) | — | 0 (0.0) | — | 0 (0.0) | — |
Data are reported as n (%). P values have not been adjusted for multiple comparisons. Dashes indicate not applicable. ACL, anterior cruciate ligament; LCL, lateral collateral ligament; MCL, medial collateral ligament; PCL posterior cruciate ligament.
Final revision submitted September 9, 2023; accepted September 18, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Ethics Committee of Shanghai Sixth People's Hospital (reference No. 2023-033).