
Abstract
Tibial plateau fractures are multiple fracture patterns associated with soft-tissue injuries. Among which, the combined existence of posterolateral tibial plateau depression fracture with anterior cruciate ligament (ACL) rupture has been reported rarely. Meanwhile, surgical method for the treatment of depression fracture is fairly complex. The aim of this article is to show a case series of this unusual injury pattern and the therapy of posterolateral tibial plateau depression fracture accompanying ACL rupture. In our treatment, arthroscopy assisted reduction of depression fracture and ACL reconstruction reduces surgical trauma and leads to good functional recovery. We also review the current literature.
Keywords
Introduction
Posterolateral tibial plateau depression fracture is a special fracture type of tibial plateau fracture, which occupies about 1% of all fractures. 1 Open reduction and internal fixation with the use of cancellous grafting is a typical methodology for the treatment of this depression fracture. 2 However, as a result of the posterolateral ligament complex, the anatomical restriction of the fibula head, and the anterior tibial artery, this surgical method for the treatment of the depression fracture is fairly complex. In addition, almost all of the tibial plateau fractures are relevant to soft-tissue structure injuries, such as ligaments, meniscus, tendons, and other soft-tissues. Gardner et al. convey that 99% presented evidence of soft-tissue injuries in knee periphery through a study of 103 tibial plateau fractures. 3 Among all soft-tissue injuries, anterior cruciate ligament (ACL) rupture is frequently related to posterolateral tibial plateau fracture, which seems to be caused by a multiplanar, valgus-shift loading pattern. 3,4 In particular, the combined existence of posterolateral tibial plateau depression fracture with ACL rupture has been reported rarely. Only a small number of cases with Segond fracture and ACL injury have been printed with an extra osseous injury to the tibial plateau, Gerdy tubercle, or femoral condyle. 5 Stabilizing posterolateral tibial plateau depression fracture with ACL rupture through arthroscopy may have a tremendous influence on postoperative functional recovery and complications. Thus, the adequate treatment is important and challenging.
In our study, we presented a case series of a special injury type of posterolateral tibial plateau depression fracture associated with ACL rupture and medial collateral ligament (MCL) injury which was treated with arthroscopy assisted reduction of depression fracture and ACL reconstruction. A review of the current literature being related to this injury type is also included.
Case presentation and surgical management
Three cases of posterolateral tibial plateau depression fracture associated with ACL rupture were treated by arthroscopy in our hospital between 2015 and 2017.
Case 1
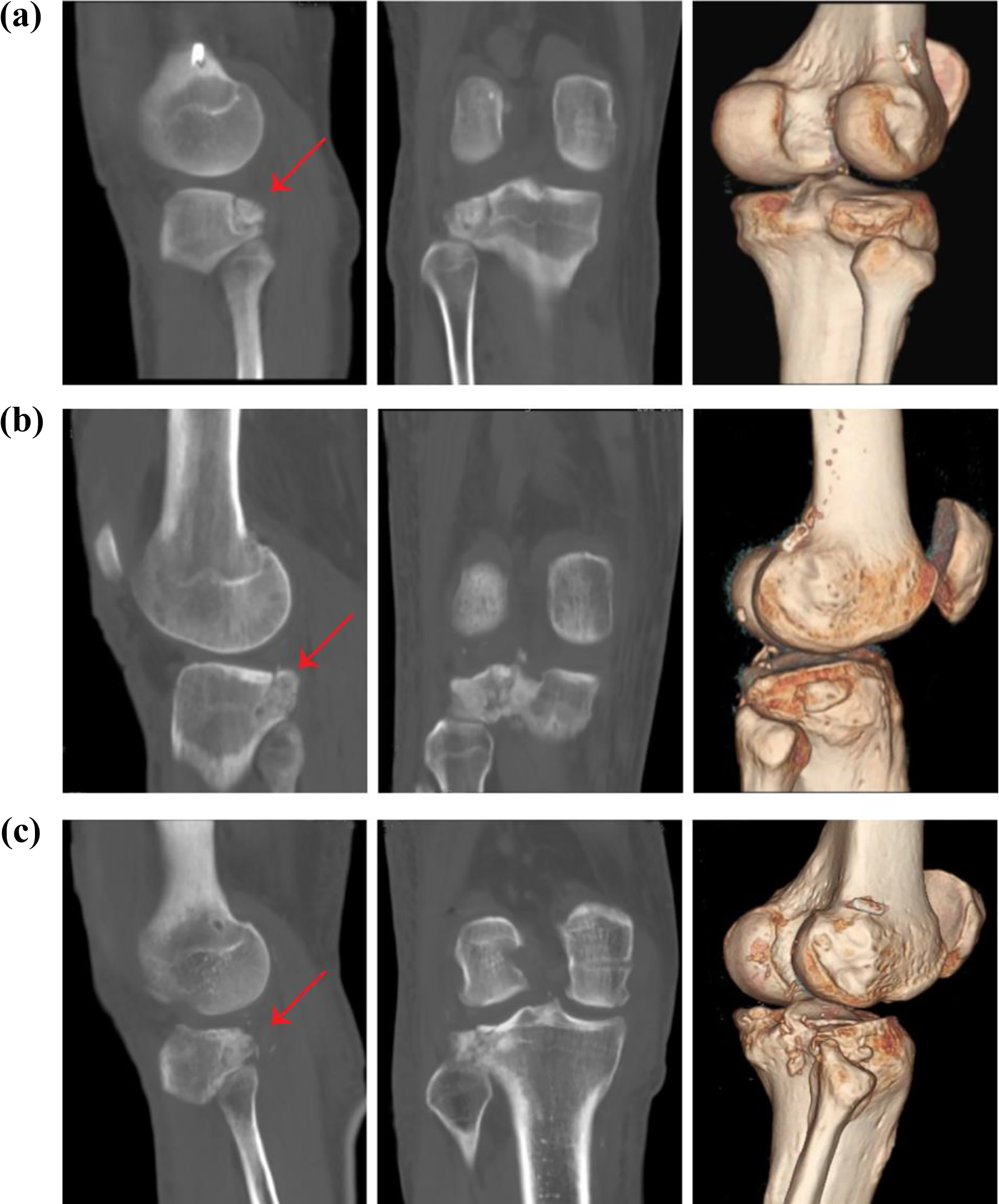
A 29-year-old man sustained a car accident during December 2015. He was admitted in our hospital with pain, swelling, and reduced functional capacity of the right knee. Physical examination: mild swelling of the right knee, anterior drawer test (+), and Bohler’s sign (+). It was not clear whether the fracture existed in the Plain radiographs (Figure 1(a)), while computerized tomography (CT) scan (Figure 2(a)) showed a clear compression fracture of the posterolateral tibial plateau. Magnetic resonance imaging (MRI) was performed to accomplish the examinations because of the doubt of soft-tissue injuries. The MRI clearly showed that the ACL was torn (Figure 3(a)).
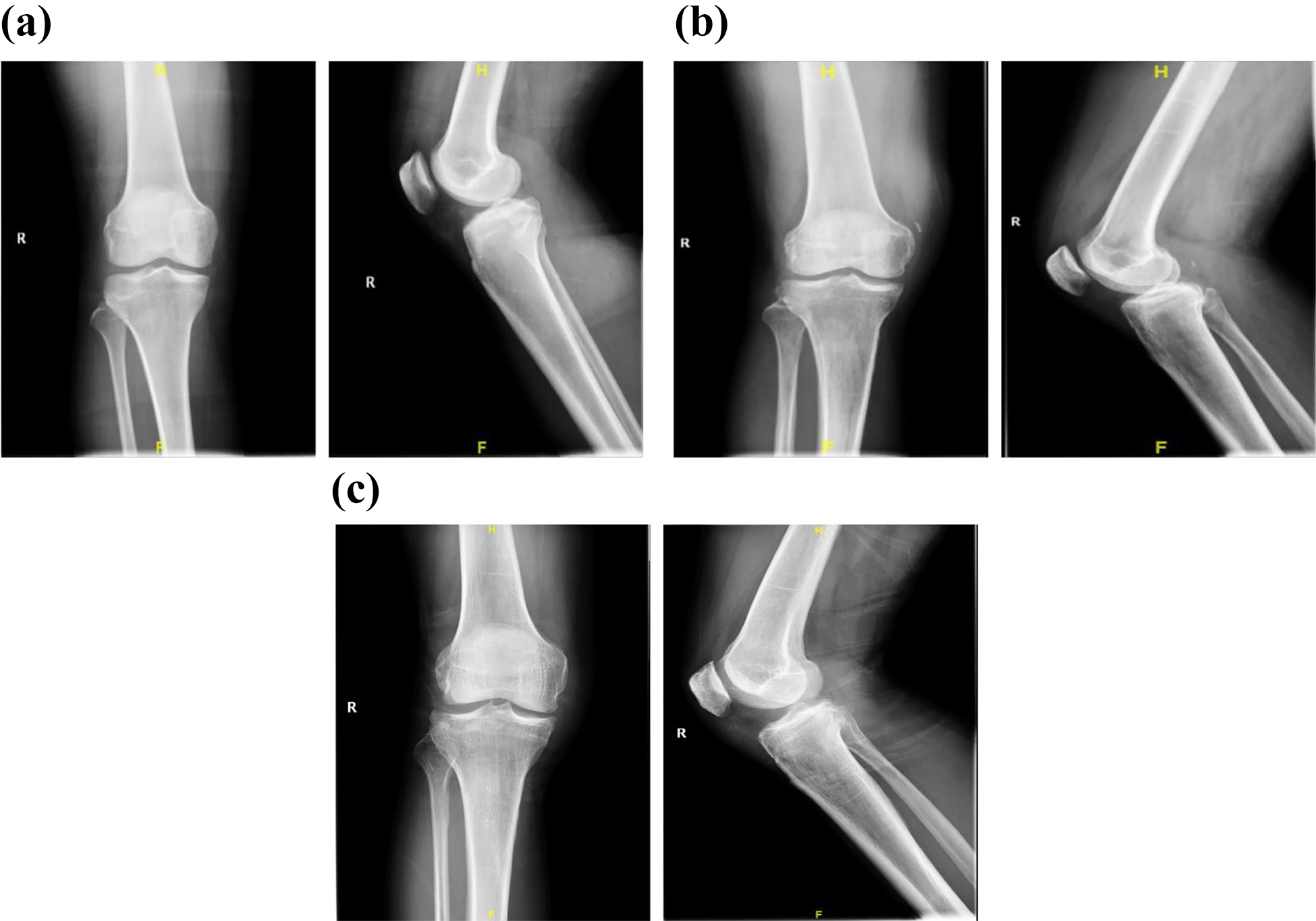
Plain radiographs of the three cases.

CT-scan images of the three cases, red arrow means fracture.

MRI findings, with torn ACL in all cases, red arrow means torn ACL. MRI: magnetic resonance imaging; ACL: anterior cruciate ligament.
Case 2
A 58-year-old man fell down from the Electric Vehicle during March 2015. He was transferred to our hospital with pain and functional restriction in the right knee. Physical examination: swelling of the right knee, anterior drawer test (+), and Bohler’s sign (+). Plain radiographs (Figure 1(b)) and CT-scan (Figure 2(b)) showed a compression fracture of the posterolateral tibial plateau. The MRI scan revealed a compression fracture of the posterolateral tibial plateau and showed the ACL was torn (Figure 3(b)).
Case 3
A 56-year-old man fell down from a tree during March 2016. He was admitted in our hospital with pain, swelling, and reduced functional capacity of the right knee. Physical examination: swelling of the right knee, anterior drawer test (+), and Bohler’s sign (+). It was difficult to recognize the fracture from the Plain radiographs (Figure 1(c)), whereas CT-scan (Figure 2(c)) presented a compression fracture of the posterolateral tibial plateau. Fibula head was intact. The MRI scan revealed that the ACL was torn (Figure 3(c)).
In all cases, the MCLs were also injured. The surgical steps were as follows.
The operations were performed with the patients in a dorsal position in the absence of a tourniquet. The antibiotic (Cefazolin) was administered in all patients for prophylaxis. Considering that the compression fracture position was at the most posterior area of the lateral plateau, and open reduction of the articular surface was difficult, we carried out surgery with closed reduction through a minimal incision arthroscopically. The first step was fracture reduction under arthroscopy. ACL reconstruction locator is positioned at the posterolateral tibial plateau collapse (Figure 4). The Kirschner needle was drilled from the medial lower edge of the tibial plateau, the bone tunnel was made with an 8 mm in diameter drill, and the top rod was drilled into the position from the tibial medial margin where the compression fracture is situated to reset the collapse of joint surfaces. After reduction of the articular surface was confirmed by arthroscopy, cancellous allograft bone was implanted into the bone tunnel to compensate the bone defect. The fracture reduction was good and no further support and fixation was used (Figures 5 and 6). Structures such as the fibular nerve (common peroneal nerve or lateral popliteal nerve) and the popliteus tendon were carefully preserved in this procedure. After fracture reduction, the complete rupture of the ACL was found by arthroscopy. Next step was the reconstruction of the ACL. A standard anatomical single bundle ACL reconstruction procedure was used for these patients with autologous hamstring tendon under arthroscopy. Finally, MCL was repaired.

Anterior cruciate ligament reconstruction locator (black arrow) is positioned at the posterolateral tibial plateau collapse (red arrow).

Radiological outcome after surgery.
CT-scan outcome after surgery, red arrow means the fracture which is fixed.
After operation, a long leg brace was applied for initial immobilization in the next day. Subsequently, the knees of the patients were put through the continuous passive motion machine as tolerable. They commenced non-weight bearing walking with the help of crutches. The knee brace, which has a goniometer, was worn for flexion and extension exercises. All patients were discharged from hospital on the fifth–sixth postoperative day with good recovery. There were no postoperative complications.
Discussion
ACL and MCL injury in association with a compression fracture of the posterolateral tibial plateau is, as far as we know, a rare pattern with very few cases recorded in the documents. The cases reported involving small peripheral compression fracture of the anteromedial tibial border along with cruciate ligament injuries, of which the posterior cruciate ligament (PCL) injury is the most common one. 6 –8 In 2001, Chiba et al. showed 12 cases of this injury type, which was the largest series so far. 9 They considered that a minor fracture compression of the anteromedial tibial plateau implies an accompanying PCL injury. The Segond fracture is the proximal lateral tibial avulsion fracture along with the ACL injury. The incidence of the Segond’s fracture in the ACL tears is about 9–12%. 10,11 In addition, it indicates the tear of the lateral collateral ligament or the iliotibial tract capsular fibers. 12,13 The mechanism of such type of injury is that knee is flexed along with the tibial internal rotation and forced varus on the middle portion of the lateral capsule middle portion. 14 The collision between the lateral femoral condyle and the posterolateral tibial plateau leads to these trivial chip fractures during the knee-joint damage. 15,16 Injuries to the ACL and PCL are sometimes connected with the Segond fracture. The combined osteochondral fracture of the posterolateral tibial plateau and Segond fracture with ACL injury in a skeletally immature patient was reported by Tei et al. 17 In the view of those injuries, the injury mechanism might be the impact of the lateral femoral condyle and the posterior aspect of the lateral tibia due to the anomalous internal rotation. Two cases were reported by Jiang et al, which showed the similar injury pattern described by us: ACL rupture combined with a posterolateral tibial plateau fracture. 18 In their opinion, the possible injury mechanism was a violent internal tibial rotation/anterior tibial translation without any valgus or varus knee force mechanism. In our patients, the knees experienced flexion and internal rotation during the accident. The underlying mechanism of our patients was the internal rotation of tibial plateau in conjunction with anterior tibial shifting in noncontact ACL injury. The collision between the posterolateral tibial plateau and the lateral femoral condyle was possibly hard but focused which caused the compression fracture to appear. We believed that the posterolateral tibial plateau depression fracture was hit by the femoral condyle when the knee flexion and internal rotation of the tibial occurred. Moreover, ACL and MCL injury could be as a result of the vigorous internal rotation of the tibial or anterior tibial shifting with the knees in a forced valgus mechanism. Based on our findings and according to the findings of other authors, we thought that a small compression fracture of posterolateral tibial plateau strongly suggests an accompanying ACL and MCL injury.
On the part of tibial plateau fractures, clinicians still pay close attention to its fixation and functional results. 19 –21 Among these fractures, depression fractures are known as one of the most complicated to administer. It is well-known that open reduction and internal fixation with the use of autologous cancellous grafting is the traditional methodology for the treatment of depression tibial plateau fractures. 2 Jiang et al. used the posterolateral approach to expose the fracture zone with lag screws for stability, and the ACL reconstruction was done before the open reduction of the depression tibial plateau fracture. 18 In our cases, the tibial plateau fractures were an actual collapse of the articular surface at the posterolateral zone of tibial plateau. In our treatment, this type of fracture mainly has three injuries: the ACL rupture, MCL injury, and a posterolateral tibial plateau depression fracture. So, we reconstructed these structures. The fracture could be seen by arthroscopy, and ACL rupture was found. The posterolateral tibial plateau depression fracture was reduced, which restored the congruity of the joint. Then, ACL was reconstructed assisted with arthroscopy. Finally, MCL was repaired. In this approach, the fibular nerve and the popliteus tendon were not exposed and were carefully protected. Meanwhile, screws were not needed. In our opinion, arthroscopy has its distinctive function in these cases to assist in observation and reduction of the joint surface. In addition, with the help of arthroscopy, the treatment of tibial plateau fractures permits speedy convalescence, low complications rate, and short hospital stay. 22 Treatment of suitable tibial plateau fractures assisted with arthroscopy can reduce surgical trauma and lead to good functional recovery. This method is worth expanding to the therapy of other kinds of fractures in other regions. Also, open reduction and internal fixation combined with arthroscopy will show very promising results.
In conclusion, it is a very promising method where the minimal invasive technique using arthroscopy is applied in the surgical treatment of posterolateral tibial plateau depression fracture accompanying soft-tissue injuries. In future, we will do further study for the evaluation, long follow-up, and clinical application of this approach for the treatment of this type injury.
Footnotes
Authors’ contribution
Zhangfu Wang and Binbin Zheng contributed equally to this article and they were designated as co-first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partly sustained by appropriation from Public Technology Research Program of Zhejiang Province (LGF18H060011 and LGF19H060004), Zhejiang Medical Science and Technology Plan (2020KY347) and by the Science and Technology Planning Program of Taizhou City (1702KY04).