
Abstract
Background:
The long head of the biceps tendon (LHBT) is a well-known source of pain in the shoulder, especially in active patients.
Purpose:
To evaluate the outcomes and return-to-sports rate after all-arthroscopic suprapectoral tenodesis of the LHBT using a small knotless anchor.
Study Design:
Case series; Level of evidence, 4.
Methods:
In this retrospective study, 27 patients—who underwent all-arthroscopic tenodesis of the LHBT using a 2.7-mm knotless polyether ether ketone anchor—were evaluated. Sports activities, the return-to-sports rate, and other sports-related parameters (eg, pain during sports, level of sports) were examined. Sports-related data, the Constant score with isometric force (at 90° of abduction in the scapular plane), the American Shoulder and Elbow Surgeons (ASES) score, the Simple Shoulder Test (SST) score, the visual analog scale (VAS) score for satisfaction, range of motion, and the presence of a Popeye deformity were assessed at a mean follow-up of 15.3 ± 8.7 months. The data were initially analyzed using descriptive statistics.
Results:
The postoperative ASES, Constant, and SST scores were 81.61, 85.74 and 8.85, respectively. Of the 27 patients, 4 patients (14.8%) showed a Popeye deformity. Preoperatively, 25 patients (92.6%) participated regularly in some type of sports activity. All 25 patients (100.0%) were able to return to sports activities after surgery. 24 (96.0%) returned to the same level preoperatively, with 88.0% (22/25) within 6 months. Patient satisfaction with the outcome was high (VAS score: 2.15 ± 2.78). Neither bicipital groove pain nor cramping was reported. There were no signs of osteolytic bone around the anchor or a fracture of the humeral bone.
Conclusion:
Our clinical results after using a 2.7-mm knotless anchor for LHBT tenodesis as well as the return-to-sports rate were satisfying. Using an anchor this size can lower the risk of cortical bone damage and therefore the risk of fractures of the humeral head while still enabling patients to perform at a high level.
The long head of the biceps tendon (LHBT) is well known as a source of pain, especially for anterior shoulder pain. It is often combined with a tear of the rotator cuff. Other abnormalities of the biceps tendon such as pulley lesions with instability or subluxations, superior labral anterior to posterior lesions, and tenosynovitis can lead to pain.2,6,7,10,11,28,32
There are many different ways to address an abnormality of the LHBT. A recent systematic review and meta-analysis including 25 studies reported no evidence of whether LHBT tenodesis is superior to LHBT tenotomy in terms of strength, shoulder pain, and shoulder function. 17 The authors reported an odds ratio of 0.32 for the risk of developing a Popeye deformity when performing tenotomy of the LHBT, and they found that cramping pain in the biceps muscle was more common in the tenotomy group than in the tenodesis group. 17 Another meta-analysis from Anil et al 3 showed that different tenodesis procedures of the LHBT (arthroscopic intracuff tenodesis, arthroscopic subpectoral tenodesis, and open subpectoral tenodesis) resulted in better functional outcome scores and fewer Popeye deformities than simple tenotomy. The authors also mentioned that patients with arthroscopic intracuff tenodesis had more bicipital groove pain. 3
Nevertheless, there is a risk of harm to the neurovascular structures while performing subpectoral tenodesis, especially if a deep dissection is performed and the short head of the biceps tendon is retracted.21,25,29 Considering that tenodesis should preserve the normal length-tension relationship of the LHBT and provide better functional results, as well as less cosmetic problems, some studies recommend tenodesis, particularly for athletic and younger patients.3,9,10,26
The purpose of this study was to evaluate the clinical results and return-to-sports rate after suprapectoral tenodesis of the LHBT using a 2.7-mm knotless polyether ether ketone (PEEK) anchor (Microraptor Knotless; Smith+Nephew). We hypothesized that the knotless anchor would reduce the risk of bicipital groove pain and that this technique would be safe for patients.
Methods
Study Patients
This retrospective study included patients who underwent arthroscopic repair of the LHBT with the 2.7-mm Microraptor Knotless suture anchor. The study protocol received approval from the local ethics commission, and all included patients gave informed consent to participate in the study. Patients with a lack of documentation, those who were younger than 18 years old, and those who did not give their informed consent were excluded. A total of 27 patients (10 female, 17 male) were included.
Surgical Procedure
All patients underwent surgery performed by a single experienced senior surgeon (P.H.) at a single institution. Follow-up was performed by another experienced shoulder surgeon (M.B.), who was not part of the initial operating team. Surgery was executed with patients placed in the beach-chair position with an interscalene block and under general anesthesia.
A standard posterior portal and standard anterior portal were placed. Then, a 4-mm scope at 30° was inserted through the posterior portal and an arthroscopic hook through the ventral one. Afterward, diagnostic arthroscopic surgery was performed to check for abnormalities, and each abnormality was photodocumented. Through the anterior portal, the LHBT was fixed intra-articularly about 2 cm distal to its origin. Minitape (Smith+Nephew) and Firstpass or Firstpass Mini (Smith+Nephew) were used with the double lasso-loop technique as described by Lafosse et al.18,19
The biceps tendon was cut with a radiofrequency ablation probe (Werewolf; Smith+Nephew) (Figure 1). The interval of the rotator cuff was opened carefully with a scalpel, and the bicipital groove was lightly decorticated with an arthroscopic bur. Next, the tape was pulled out of the lateral portal, and the 2 ends of the tape were passed through the eyelet of the Microraptor Knotless anchor using a suture threader. The appropriate drill guide and obturator were inserted high in the bicipital groove. After removing the obturator, the recommended drill was used to prepare the insertion site (Figure 2).

After fixation via the lasso-loop technique, the long head of the biceps tendon was cut with a radiofrequency ablation probe.

Insertion of the drill guide to prepare the bicipital groove for the anchor.
Next, the drill and the drill guide were removed, and the loaded suture anchor was inserted in the operative cannula. Tension was applied to the suture, and a mallet was used to tap the inserter handle until the laser mark was flush with the cortical bone (Figure 3). The knob was rotated clockwise until a minimum of 5 clicks was recognized to deploy the anchor. Then, we removed the inserter by pulling it straight back and cut the excess suture.

(A) Insertion of the anchor and tensioning of the suture. (B) Final insertion of the anchor until the laser mark was flush with the cortical bone.
Postoperative Protocol
If patients only underwent biceps tenodesis, no shoulder arm support was required. Only restricted weightbearing in elbow flexion was mandatory for 6 weeks after surgery. Patients were allowed to begin finger, hand, wrist, and elbow mobilization immediately after surgery. If repair was performed because of a concomitant injury (such as repair of the labral complex or the rotator cuff), patients had to wear a shoulder arm support without a pillow for 4 to 6 weeks postoperatively with a specific rehabilitation protocol. For most surgical procedures, only passive mobilization was permitted within a painless range of motion for 4 to 6 weeks, followed by active-assisted mobilization with ongoing increasing weight.
Functional Outcome Measures
To evaluate the clinical outcomes, different patient-reported outcome measures were used. They included the Constant score, the American Shoulder and Elbow Surgeons (ASES) score, and the Simple Shoulder Test (SST). In addition, isometric force was measured at 90° of abduction in the scapular plane using an IDO isometer (Innovative Design Orthopaedics, Redditch, UK). Patient satisfaction with surgery was measured at the final follow-up using a visual analog scale (VAS) from 0 to 10, with 0 indicating very satisfied.
Patients who participated regularly in sports completed a questionnaire on engagement in sports and recreational activities (eg, sports activities, frequency, sports level, time to return to sports, shoulder pain/fear during sports, and satisfaction with surgery) both preoperatively and postoperatively. Shoulder pain and fear during sports were measured using a VAS from 0 to 10, with 0 indicating best outcomes. We defined amateur sports as activities in which the participants engaged widely or completely without remuneration.
Radiographic Data
Radiographs in the anteroposterior/axial view were obtained in all patients preoperatively, immediately postoperatively, and at the final follow-up. All radiographs were evaluated by 2 clinicians independently. One was an orthopaedic surgeon (M.B.), who did not perform surgery. The other one was an external radiologist not involved in the study.
Statistical Analysis
The data were initially analyzed using descriptive statistics (mean ± SD or absolute value and percentage). For continuous data, only parameter-free testing (Mann-Whitney U test or Wilcoxon signed-rank test) was used because of the small sample size and the presence of outliers. The chi-square test was used for categorical data. All reported tests were 2-tailed. P values ≤.05 were considered statistically significant. All statistical analyses were performed with SPSS Statistics (Version 28.0; IBM) and R (Version 4.3.2; The R-Foundation for Statistical Computing).
Results
The mean follow-up of the 27 patients was 15.3 ± 8.7 months. The mean age was 54.2 ± 8.2 years, and the mean body mass index was 27.2 ± 4.0 kg/m2. Overall, 18 shoulders were affected on the right side and 9 on the left side (1 patient was treated on both sides). The dominant shoulder was the right shoulder for most of the patients (n = 22 [81.5%]), which was determined by asking them. Patients’ characteristics are shown in Table 1.
Patient Characteristics a

Data are reported as mean ± SD or n (%).
Concomitant procedures were performed in 88.9% of the patients, as seen in Table 2. Most of them were subacromial decompression procedures (70.4%). Rotator cuff repair was necessary in 40.7% of patients. The most affected tendon was the supraspinatus; in some patients, there was more than 1 tendon affected. Of the 27 patients, 4 patients showed a Popeye sign. Most Popeye signs (3/4 [75.0%]) were diagnosed in male patients. At the final follow-up, none of the patients reported muscle cramping or local pain in the bicipital groove.
Concomitant Procedures and Popeye Sign a

Data are reported as n (%).
Clinical Outcome Scores
Figure 4 shows the outcome scores that were collected. The mean ASES score was 81.61 ± 14.36, the mean Constant score was 85.74 ± 14.45, and the mean SST score was 8.85 ± 2.66. For the ASES and Constant scores, there were no significant differences between male and female patients, although male patients tended to have higher scores than their female counterparts (ASES: 85.41 ± 12.12 vs 75.16 ± 16.17, respectively [P = .073]; Constant: 89.82 ± 7.44 vs 78.80 ± 20.49, respectively [P = .054]). There was a significant sex-related difference in the SST score of 2.15 (9.65 ± 1.83 [male]vs 7.50 ± 3.34 [female]; P = .040). With a mean VAS satisfaction score of 2.15 ± 2.78 (0-2 = very satisfied, 3-4 = satisfied), the patients in our study were mostly very satisfied or satisfied with the postoperative result.
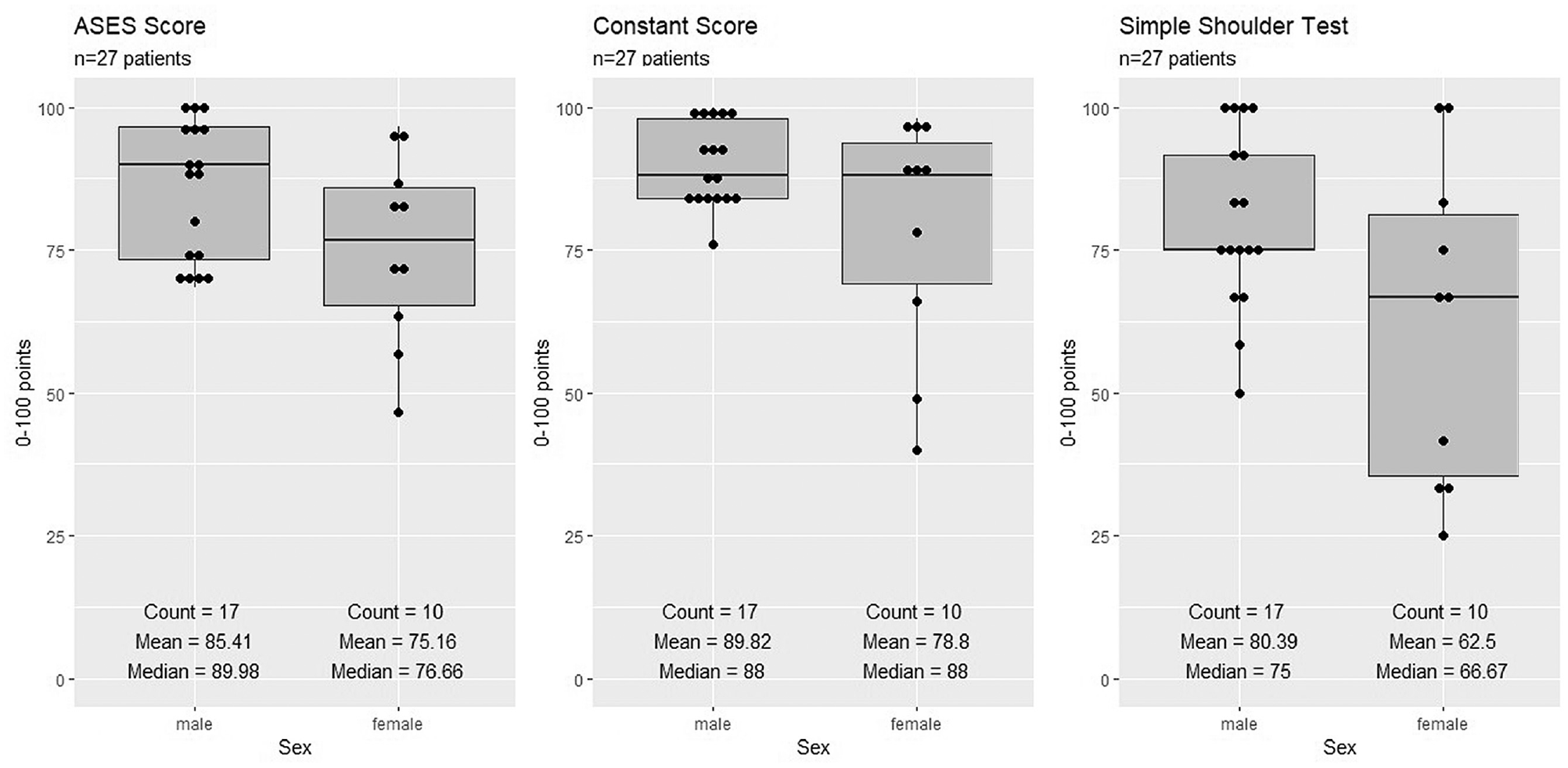
Clinical outcome scores for the American Shoulder and Elbow Surgeons (ASES) score, Constant score, and Simple Shoulder Test (SST) according to patient sex.
A total of 24 patients (88.9%) reached forward flexion and abduction over 151°. Additionally, 25 of the patients (92.6%) were able to position their arm up to the top of the head or higher. Internal rotation to reach the 12th vertebra or higher was possible in 25 patients (92.6%). The operated shoulder showed a mean isometric force of 7.49 ± 3.21 kg at 90° of abduction in the scapular plane. Male patients were able to apply more force than female patients (8.26 ± 2.45 vs 6.19 ± 4.00 kg, respectively; P = .106).
Sports Participation
Preoperatively, 25 patients (92.6%) participated regularly in some type of sports activity. Most (22/25 [88.0%]) played sports at an amateur level. Only 3 patients (12%) played sports professionally. One former professional athlete who was unable to participate in his sport after his injury was able to return to his sport at a professional level after surgery. In the amateur group, 3 patients had to stop their sports activities after their injury, but all of them were able to return at the amateur level postoperatively. Another one of the professional athletes had to change to the amateur level after surgery and could not return to a professional level. This patient was 1 of 4 with additional symptomatic acromioclavicular joint arthrosis who underwent concomitant acromioclavicular joint resection.
All 25 patients (100.0%) were able to return to sports activities after surgery, and 24 (96.0%) returned to the same level preoperatively. However, not all of them participated in the same sport postoperatively as they did before surgery, as seen in Figure 5. In total, patients mentioned thirteen different sport activities which they performed preoperatively. This results in 96 different sport activities peformed by 25 patients (as each performed 1 or more). Whereas, postoperatively only 16 different sport activities (16.7%) could no longer be performed, 80 (83.3%) could still be performed. Patients had to stop their preoperative sport because of various reasons (pain during sports, fear of reinjury, insufficient range of motion). Regarding timing, 15 patients (60.0%) returned to sports between 1 and 3 months postoperatively, and 7 patients (28.0%) returned between 4 and 6 months postoperatively. Only 2 patients (8.0%) needed more than half a year (7-12 months) to return to sports. One patient could not remember exactly when he returned to sports.
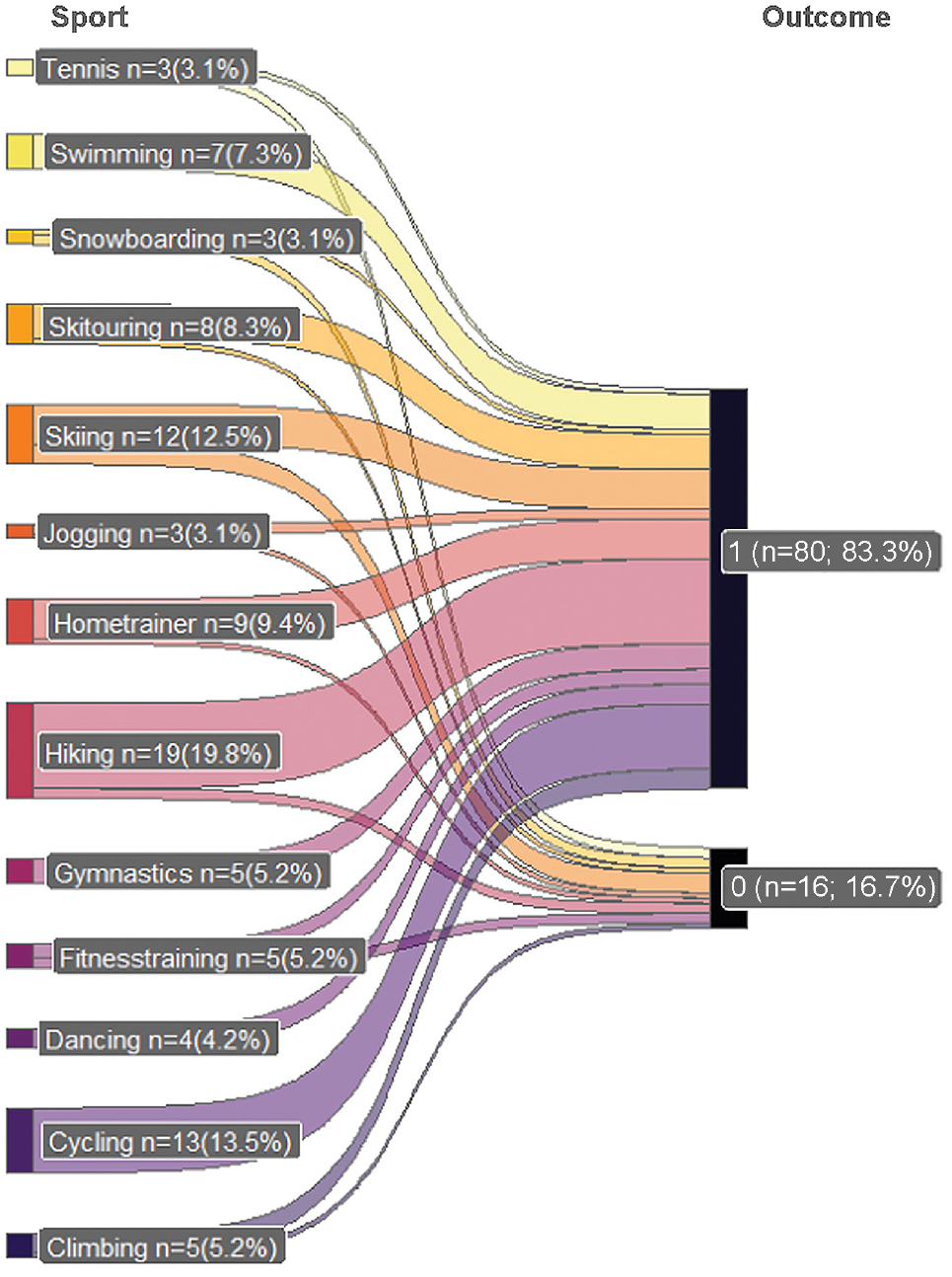
Type of sports activities preoperatively versus postoperatively. 1 = returned to sports; 0 = stopped playing sports.
Shoulder pain during sports as measured by the VAS was reduced significantly after surgery (3.78 ± 2.95 [preoperatively] vs 2.70 ± 2.64 [postoperatively]; P = .013). Nonsignificant improvements after surgery were also seen in the VAS score for shoulder pain after sports (2.96 ± 2.73 [preoperatively] vs 2.38 ± 2.87 [postoperatively]; P = .442) and for subjective fear during sports (0 = feel totally safe, 10 = feel totally unsafe) (3.27 ± 3.06 [preoperatively] vs 2.32 ± 2.84 [postoperatively]; P = .285).
The top 5 sports disciplines in which the patients participated before and after surgery are shown in Table 3. Male and female patients participated in the same top 5 sports. In both groups, most of the patients had to quit skiing or hiking after surgery. Patients participated in a mean of 4.00 ± 2.43 different sports before surgery. This decreased to 3.44 ± 2.14 sports postoperatively (P = .060). More sports were played preoperatively than postoperatively for both female (3.80 ± 1.81 vs 3.00 ± 1.56, respectively; P = .071) and male (4.12 ± 2.78 vs 3.71 ± 2.42, respectively; P = .347) patients. Furthermore, women participated in fewer sports disciplines after surgery than men (3.00 ± 1.56 vs 3.71 ± 2.42, respectively; P = .428).
Participation in Top 5 Sports Disciplines by Sex

Change in percentage from preoperatively to postoperatively.
Younger patients (age <60 years) participated more often in different sports activities preoperatively compared to older patients (age ≥60 years) (4.17 ± 2.81 vs 3.67 ± 1.50, respectively; P = .374). Moreover, younger patients returned to fewer sports disciplines than those who were older (–0.89 ± 1.57 vs 0.11 ± 0.93, respectively; P = .173). Patients who had to change their sports habits most frequently mentioned fear or pain during sports and reduced range of motion in the shoulder as reasons.
Overall, most of the patients played sports fewer than 4 times per week, as seen in Figure 6. Of the patients who engaged in sports actively (≥4 d/wk), a greater percentage were older both preoperatively (age <60 vs ≥60 years: 19% vs 22%, respectively) and postoperatively (age <60 vs ≥60 years: 6% vs 11%, respectively). When comparing the length of each sports session, more male patients were found to play longer (>60 min/session) than female patients (69% vs 63%, respectively).

Number of days per week that patients played sports preoperatively and postoperatively.
Radiographic Results
No signs of osteolytic bone around the anchor were seen on postoperative radiographs. The anchor was found to be still in position with good osseous integration. Furthermore, no fracture or bony defect was detected radiographically.
Discussion
In the current study, we evaluated outcomes after suprapectoral tenodesis of the LHBT using a 2.7-mm knotless PEEK anchor and found that 100% of patients who participated in sports regularly were able to return to sport. Moreover, 96.0% were able to return to sports at the same level as before surgery. 83.3% of the preoperative sport activities were also be performed postoperatively. We also showed that return to sports was possible for older patients (age ≥60 years). None of the study patients had to undergo a reoperation.
Compared to the studies in a 2022 systematic review by Sandler et al, 30 our results are quite promising. Sandler et al 30 reported a combined return-to-sports rate of 63% to 85% after tenodesis of the LHBT. Most of our study patients who participated in sports did so at the amateur level (88.0%), and considering that an increasing number of people play amateur-level sports and have higher expectations concerning the operative outcome, we can inform our patients that they have a good chance of returning to the same preoperative level of sports after surgery. Hiking and skiing were the sports that most of the patients had to stop. For both sports, all patients used poles, which we think generates pain or problems. Overall, however, patients reported a high level of satisfaction with the postoperative result (mean VAS satisfaction score: 2.15 ± 2.78).
In our cohort, 4 patients (14.8%) developed a Popeye deformity. The data in the literature are quite heterogeneous, and some studies have reported similar rates after tenodesis of the LHBT (11.4%-27.8%).1,12,22 We found that 3 of the 4 patients with this deformity were male. A randomized clinical trial with 114 patients showed that male patients had a 7 times greater chance of developing a Popeye deformity compared with female patients. 33
Even though we had no preoperative clinical outcome scores, our postoperative clinical outcome scores were quite satisfying compared to those in other studies. With a mean postoperative Constant score of 85.74 ± 14.45, we achieved higher results than other studies that also performed tenodesis high in the bicipital groove (72.8-76.1).5,8,12 Our results are promising compared with those of Boileau et al, 7 who reported a Constant score in the tenodesis group of 72.8 in patients with rotator cuff tears, because 40.7% of the patients in our cohort also underwent concomitant rotator cuff repair. The rotator cuff tears within the Boileau et al 7 cohort were described as irreparable, however, and the tears in our cohort could have been repaired primarily. With a mean ASES score of 81.61 and a mean SST score of 8.85, our patients fared better than in other comparable studies (ASES: 64.3-79.4; SST: 6.1-11.3).4,5,20,22,23 Because of our promising postoperative clinical results, we recommend repair of a concomitant rotator cuff tear (massive or not). This is in line with the literature in which even incomplete arthroscopic repair showed satisfactory clinical outcomes in massive rotator cuff tears. 14
Bicipital groove pain and cramping are well-known problems after surgical procedures of the LHBT. In 3 meta-analyses,3,17,24 it was reported that cramping pain of the muscle occurs more in patients with tenotomy; however, bicipital groove pain was seen more often in patients who had undergone tenodesis of the LHBT, especially those undergoing an intracuff procedure. None of the patients in our study cohort reported bicipital groove pain or cramping, although it should be considered that our sample size was small. Yet, we assume that knotless fixation prevents the occurrence of knot irritation, which can cause pain. Kongmalai 16 and Song and Williams 31 described their tenodesis techniques using 4.5-mm knotless anchors and confirmed the advantage of missing knot irritation as well. In our study, we were able to demonstrate that our technique with only a 2.7-mm knotless anchor could achieve excellence and comparable clinical results. Even though interference screws and suture anchors have shown equal biomechanical and clinical results, 27 Koch and Burks 15 reported that using an interference screw can lead to damage of the LHBT because of compression against the cortical bone. A recent systematic review with 74,394 patients showed a mean fracture rate of 1.0% ± 1.6% (in 669 patients) and a higher risk with open techniques and/or using interference screws. 13 In our study, none of the patients showed any sign of osteolytic bone around the anchor or a fracture of the humeral bone. Consequently, we assume that the small 2.7-mm anchor size reduced the risk of bone damage while performing tenodesis. Moreover, this technique can easily be applied. We also believe that another advantage of using a small anchor might be that in case of wrongly setting the first anchor, another small anchor can be inserted just beside it. This will not be as easy if bigger anchors are used.
Limitations
Our study had several limitations. First, the design of the study is a retrospective study, which has inherent limitations. Furthermore, the sample size is small with a short follow-up period. However, this also results from the fact that this anchor has not been used until more recently for LHBT tenodesis. Second, 3 of the 27 study patients were not able to appear in person for follow-up appointments. Thus, a self-reported Constant score was used, and patients were contacted via telephone to clarify open questions and guarantee a complete dataset. In these 3 patients, radiographs were only available at about 2 months postoperatively and not at the time of follow-up. Moreover, our clinical scores and questionnaire responses on sports activities were available only postoperatively, even though questions about preoperative sports habits were asked. Finally, there were no patients with isolated pulley or superior labral anterior to posterior lesions, which would result in biceps tenodesis only. Similar to most of the existing studies, most (88.9%) study patients underwent concomitant procedures, which may have biased the findings.
Conclusion
Tenodesis of the LHBT with a 2.7-mm knotless anchor resulted in good clinical outcomes with a high return-to-sports rate (100%), even with concomitant procedures. 96.0% were able to return to sports at the same level as before surgery. 83.3% of the preoperative sport activities were also performed postoperatively. Using an anchor this size can lower the risk of cortical bone damage and therefore the risk of fractures of the humeral head while still enabling patients to perform at a high level. Future studies with more patients and a longer follow-up are needed to support our results.
Footnotes
Final revision submitted August 27, 2023; accepted September 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The Department of Orthopedic and Trauma Surgery at Klinik Diakonissen Schladming has received honoraria from Smith+Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Medical University of Graz (ref No. 1102/2022).