
Abstract
Background:
The rate of concomitant meniscal procedures performed in conjunction with anterior cruciate ligament (ACL) reconstruction is increasing. Few studies have examined these procedures in high-risk pediatric cohorts.
Hypotheses:
That (1) the rates of meniscal repair compared with meniscectomy would increase throughout the study period and (2) patient-related factors would be able to predict the type of meniscal operation, which would differ according to age.
Study Design:
Cohort study (prevalence); Level of evidence, 2.
Methods:
Natural language processing was used to extract clinical variables from notes of patients who underwent ACL reconstruction between 2000 and 2020 at a single institution. Patients were stratified to pediatric (5-13 years) and adolescent (14-19 years) cohorts. Linear regression was used to evaluate changes in the prevalence of concomitant meniscal surgery during the study period. Logistic regression was used to determine predictors of the need for and type of meniscal procedure.
Results:
Of 4729 patients (mean age, 16 ± 2 years; 54.7% female) identified, 2458 patients (52%) underwent concomitant meniscal procedures (55% repair rate). The prevalence of lateral meniscal (LM) procedures increased in both pediatric and adolescent cohorts, whereas the prevalence of medial meniscal (MM) repair increased in the adolescent cohort (P = .02). In the adolescent cohort, older age was predictive of concomitant medial meniscectomy (P = .031). In the pediatric cohort, female sex was predictive of concomitant MM surgery and of undergoing lateral meniscectomy versus repair (P≤ .029). Female sex was associated with decreased odds of concomitant LM surgery in both cohorts (P≤ .018). Revision ACLR was predictive of concomitant MM surgery and of meniscectomy (medial and lateral) in the adolescent cohort (P < .001). Higher body mass index was associated with increased odds of undergoing medial meniscectomy versus repair in the pediatric cohort (P = .03).
Conclusion:
More than half of the young patients who underwent ACLR had meniscal pathology warranting surgical intervention. The prevalence of MM repair compared with meniscectomy in adolescents increased throughout the study period. Patients who underwent revision ACLR were more likely to undergo concomitant meniscal surgeries, which were more often meniscectomy. Female sex had mixed effects in both the pediatric and adolescent cohorts.
The knee is one of the most commonly injured joints in athletes, and roughly 20% of these injuries involve the anterior cruciate ligament (ACL).11,21 A well-documented increase has been seen in the incidence of pediatric ACL injury and ACL reconstruction (ACLR), which is outpacing most general pediatric orthopaedic procedures and adult ACLR.3,5,13,39,42 Prompt intervention in skeletally immature patients is recommended to minimize the risk of developing further pathologic changes in the joint, including chondral and meniscal injury, which are well-established risk factors for osteoarthritis.1,14,23,25,28 ACLR in this cohort has been shown to expedite return to sports and other activities and reliably address knee instability.15,17
Isolated injury to the ACL is less common, 43 and associations with concomitant injury to the menisci have been well established, particularly in younger patient cohorts.4,12,19,29,31,41 In addition to the increasing rates of pediatric ACL injury, the rates of concomitant meniscal surgeries have been likewise increasing.4,12 Compared with adults, pediatric patients tend to have better outcomes after meniscal repair, which have been attributed to enhanced vascularity and healing potential.10,20 Accordingly, a growing trend of increasing rates of pediatric meniscal repair over meniscectomy has emerged.4,29,42 Although the risk factors for concomitant meniscal injury in adult ACL injuries have been well studied, such investigations are sparse in pediatric and adolescent cohorts.7,36 A recent single-center study performed by Perkins et al 32 revealed that increasing age and body mass index (BMI) were independent risk factors for concomitant meniscal injury in a pediatric cohort. Conversely, a recent analysis of American Board of Orthopaedic Surgery candidate data concluded that age was not associated with concomitant meniscal surgery in pediatric patients. 12 Such discrepancies underscore the paucity of literature regarding pediatric risk factors for meniscal injury and treatment in association with ACLR and how these compare to those in adult populations.
The purpose of this study was to evaluate and compare trends in the prevalence of concomitant meniscal procedures in pediatric and adolescent patients undergoing ACLR and evaluate associated risk factors for concomitant meniscal surgery as well as meniscectomy versus meniscal repair. Such data may inform more evidence-based and patient-centered treatment algorithms in these common injury patterns. We hypothesized that the rates of meniscal repair compared with meniscectomy would increase between 2000 and 2020. Additionally, we hypothesized different patient-related factors would be predictive of the type of meniscal operation performed in pediatric versus adolescent patients.
Methods
Participants
After obtaining institutional review board approval, we used a custom natural language processing (NLP) pipeline 37 to identify all patients who underwent ACLR at our institution between January 1, 2000, and December 31, 2020, and we extracted pertinent clinical and operative data from the available unstructured electronic clinical notes to develop an institutional ACLR registry. Details of the NLP pipeline used along with model performance metrics and validation have been previously published.37,38 Briefly, we developed with an NLP model to identify ACL surgical cases from operative notes (accuracy, 1.00; sensitivity, 0.99; specificity, 1.00). 38 We then extracted relevant injury and surgical details from the operative notes of the identified patients using NLP (accuracy, 0.98 ± 0.01; sensitivity, 0.97 ± 0.03; specificity, 0.98 ± 0.02). 37
Age, sex, height, weight, BMI, race, and insurance status were retrieved from the structured medical record. Mechanism of injury (ie, contact vs noncontact), ipsilateral ACL injury history, and sports participation were extracted from preoperative notes using NLP. Laterality and concomitant operations, including meniscal repair and meniscectomy, were extracted from the operative reports using NLP. Patients were grouped by age, with the pediatric cohort made up of patients between 5 and 13 years of age and the adolescent cohort between 14 and 19 years, to characterize the effects of puberty and the transition toward skeletal maturity on the risk of concomitant surgery.16,22 Patients were also compared based on their participation in high-risk sports according to the classification proposed by Moksnes et al, 27 who adapted the original system developed by Hefti et al. 18 With this system, level 1 activities include frequent jumping, cutting, and pivoting (eg, soccer, basketball); level 2 activities involve lateral movements with less pivoting (eg, racket sports, gymnastics); and level 3 activities include primarily straight-ahead activities without jumping or pivoting (eg, running, weightlifting). 26
All surgeries were performed by 1 of 8 sports medicine fellowship–trained orthopaedic specialists, 4 of whom also completed general pediatric orthopaedic surgery fellowships. Surgical technique varied by surgeon and was based on a variety of patient-based criteria, but these criteria were not consistent among the surgeons.
Statistical Analysis
Demographic characteristics were summarized by standard descriptive summaries (ie, means and standard deviations for continuous variables such as age, percentages for categorical variables such as sex). Linear regression was used to evaluate changes in prevalence of concomitant medial and lateral meniscal procedures during the study period as well as the percentage of those procedures that were meniscal repairs. Separate models were developed for the pediatric and adolescent cohorts, yielding 8 linear regression models. The slopes of the linear regression models (betas) were used to estimate the change in prevalence per year. The linear regression models were developed using GraphPad Prism 8 (GraphPad Software).
Subsequently, logistic regression was used to evaluate potential predictors of meniscal procedure. Separate models were developed for (1) concomitant medial meniscal procedure, (2) concomitant medial meniscectomy, (3) concomitant lateral meniscal procedure, and (4) concomitant lateral meniscectomy for the 2 cohorts, again yielding 8 unique models. The models used to predict meniscectomy were created using only data from the cohort undergoing any meniscal procedure to isolate predictors of meniscectomy versus repair. Male sex, primary ACLR, level 1 sports participation, private insurance, White race, noncontact injury, and left knee injury were used as baselines for comparison and thus do not have an associated odds ratio (aOR). The logistic regression models were developed using RStudio (RStudio, Inc). Statistical significance was set at P < .05.
Results
Between January 2000 and December 2020, there were 4729 ACLRs identified by the NLP pipeline. The mean age of patients at the time of surgery was 15.6 years (range, 5.3-19.9 years), and the sample included 2586 (54.7%) female patients. A total of 2459 patients (52.0%) underwent at least 1 concomitant meniscal operation. Of the total concomitant meniscal procedures, 1656 (54.6%) were meniscal repairs; 309 (6.5%) of the identified operations were revision ACLR procedures (Table 1). Data regarding graft use are presented in Table 2.
Cohort Characteristics a
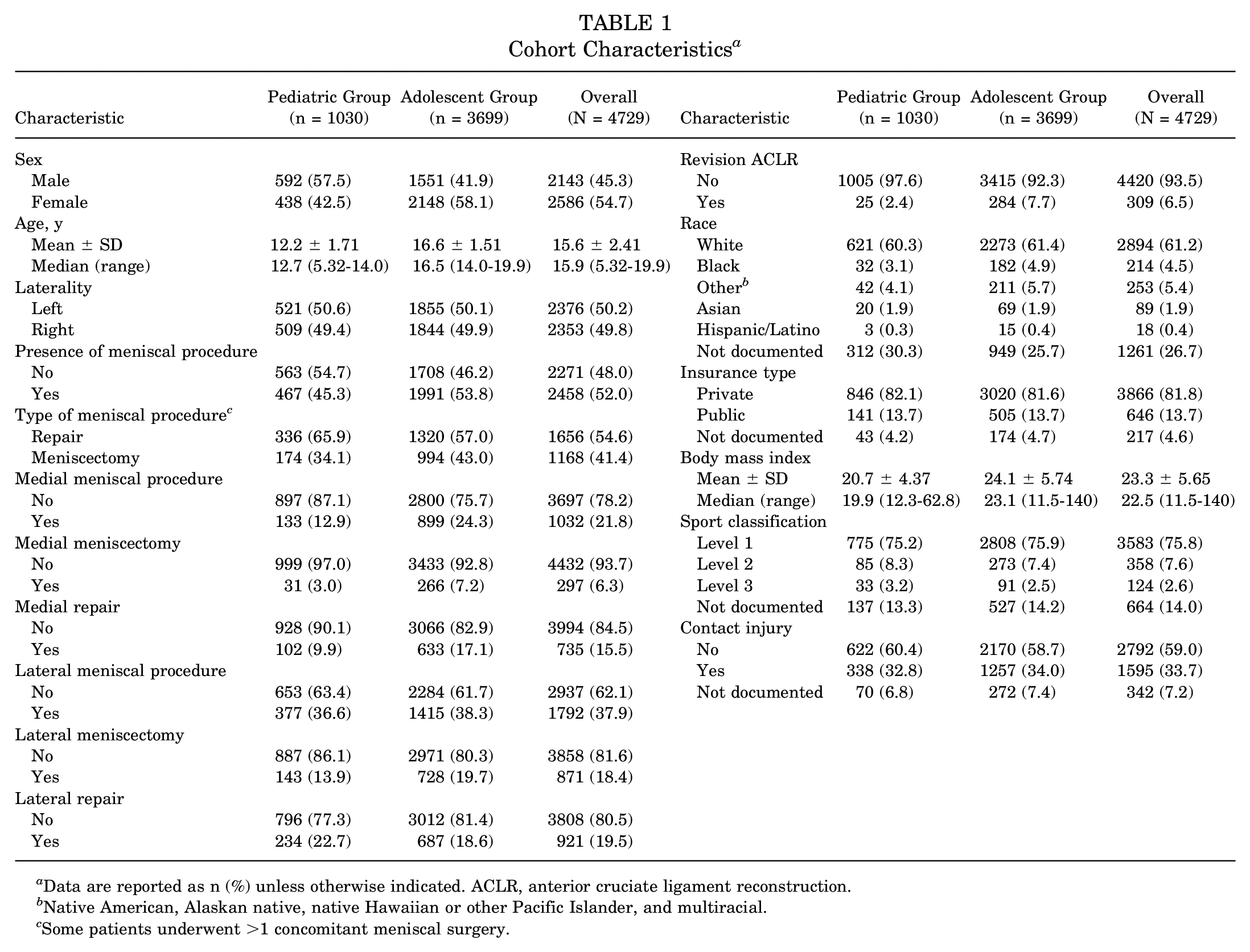
Data are reported as n (%) unless otherwise indicated. ACLR, anterior cruciate ligament reconstruction.
Native American, Alaskan native, native Hawaiian or other Pacific Islander, and multiracial.
Some patients underwent >1 concomitant meniscal surgery.
Graft Use During the Study Period (2000-2020) a

Data are reported as n (%). ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone.
20-Year Trends in Concomitant Meniscal Surgeries
The results from the linear regression models are seen in Table 3. No changes were found in the overall prevalence of concomitant medial meniscal procedures at the time of ACLR in either cohort (R2 < 0.08; P > .2). Among adolescent patients undergoing medial meniscal procedures, a 1.0% annual increase in medial meniscal repair procedures was seen (R2 = 0.25; P = .02), but no change in the prevalence of medial meniscal repair procedures was found in the pediatric cohort (R2 = 0.06; P = .3).
Changes in Meniscal Procedure Patterns, 2000-2020 a

Boldface P values indicate statistical significance (P < .05).
An annual increase of 0.6% to 1.2% in concomitant lateral meniscal procedures was found in the pediatric (R2 = 0.21; P = .038) and adolescent (R2 = 0.71; P < .0001) patients who underwent ACLR throughout the study period (Table 3). Among these patients who underwent a concomitant lateral meniscal procedure, no changes were observed in the proportion of patients who underwent meniscal repair in either cohort (R2 < 0.14; P > .09).
Predictors of Medial Meniscal Surgery
The aOR and 95% CI for potential predictors of concomitant medial meniscal surgery are presented in Table 4. In the pediatric cohort, only female sex (aOR = 1.93; P = .006) was associated with increased odds of undergoing a concomitant medial meniscal procedure. No patient factors were associated with decreased odds of requiring a concomitant medial meniscal procedure.
Predictors of Concomitant Medial Meniscal Procedures in the Pediatric and Adolescent Cohorts a

Boldface P values indicate statistical significance (P < .05). Dashes indicate there were insufficient data to calculate the aOR. ACLR, anterior cruciate ligament reconstruction; aOR, associated odds ratio.
In the adolescent cohort, revision ACLR (aOR = 2.68; P < .001), public insurance (aOR = 1.44; P = .006), and Asian ethnicity (aOR = 1.79; P = .043) were significant risk factors for undergoing a concomitant medial meniscal procedure. In contrast, adolescent patients who sustained a contact injury were less likely to receive a concomitant medial meniscal procedure (aOR = 0.80; P = .018) (Table 4).
Predictors of Medial Meniscectomy
The aOR and 95% CI for predictors of medial meniscectomy in the subgroup of patients who underwent concomitant medial meniscal procedures are presented in Table 5. In the pediatric group, only higher BMI (aOR = 1.33; P = .03) was associated with increased odds of undergoing meniscectomy versus repair. No patient factors were found to be associated with decreased odds of undergoing meniscectomy.
Predictors of Concomitant Medial Meniscectomy in the Pediatric and Adolescent Cohorts Who Underwent Medial Meniscal Procedures at the Time of ACLR a

Boldface P values indicate statistical significance (P < .05). Dashes indicate there were insufficient data to calculate the aOR. ACLR, anterior cruciate ligament reconstruction; aOR, associated odds ratio.
In the adolescent group, older age (aOR = 1.15; P = .031) and revision ACLR (aOR = 3.76; P < .001) were associated with increased odds of undergoing medial meniscectomy versus repair. Notably, the odds of undergoing medial meniscectomy (vs repair) decreased 7% each year throughout the study period (aOR = 0.93; P = .002) (Table 5).
Predictors of Lateral Meniscal Surgery
The aOR and 95% CI for predictors of concomitant lateral meniscal procedures are presented in Table 6. No significant predictors of undergoing a concomitant lateral meniscal procedure were found in the pediatric cohort. Of note, female pediatric patients had decreased odds of undergoing a lateral meniscal procedure (aOR = 0.68; P = .018) compared with their male counterparts.
Predictors of Concomitant Lateral Meniscal Procedures in the Pediatric and Adolescent Cohorts a

Boldface P values indicate statistical significance (P < .05). Dashes indicate there were insufficient data to calculate the aOR. ACLR, anterior cruciate ligament reconstruction; aOR, associated odds ratio.
In the adolescent population, later year of surgery (aOR = 1.04; P < .001), heavier weight (aOR = 1.02; P = .016), and right knee laterality (aOR = 1.22; P = .012) were significant risk factors for undergoing a concomitant lateral meniscal procedure. Female sex (aOR = 0.66; P < .001), increased height (aOR = 0.98; P = .047), and level 3 sports participation (aOR = 0.51; P = .011) were associated with lower odds of requiring a lateral meniscal procedure (Table 6).
Predictors of Lateral Meniscectomy
The aOR and 95% CI for predictors of lateral meniscectomy in the subgroup of patients who underwent lateral meniscal procedures are presented in Table 7. In the pediatric group, only female sex (aOR = 1.82; P = .029) was a significant predictor of lateral meniscectomy versus lateral meniscal repair. Patients with public insurance (aOR = 0.42; P = .045) had lower odds of undergoing lateral meniscectomy versus repair.
Predictors of Concomitant Lateral Meniscectomy in the Pediatric and Adolescent Cohorts Who Underwent Lateral Meniscal Procedures at the Time of ACLR a

Boldface P values indicate statistical significance (P < .05). Dashes indicate there were insufficient data to calculate the aOR. ACLR, anterior cruciate ligament reconstruction; aOR, associated odds ratio.
In the adolescent group, only revision ACLR (aOR = 2.30; P < .001) was a significant predictor of undergoing lateral meniscectomy versus repair. Additionally, right knees were less likely to undergo meniscectomy versus repair (aOR = 0.78; P = .04) (Table 7).
Discussion
The results of this longitudinal single-center study showed that 52% of young patients who underwent ACLR between 2000 and 2020 were found to have meniscal pathology warranting surgical intervention. Lateral meniscal procedures were more common than medial meniscal procedures (38% vs 22%). Analysis of changes in prevalence over time showed that the prevalence of concomitant medial meniscal procedures did not change over the study period. Notably, a significant increase was found in the proportion of patients who underwent concomitant lateral meniscal procedures in both cohorts (range, 0.58%-1.2% annually), potentially related to the high intensity of youth and adolescent sports participation and competition over time leading to more substantial, higher energy injuries. We noted a 1% annual increase in the percentage of adolescent patients undergoing medial meniscal repair (vs meniscectomy) but no increase in the proportion of patients undergoing lateral meniscal repair in either cohort. In the adolescent cohort, revision ACLR was more consistently associated with the need for concomitant meniscal procedures, particularly meniscectomy, when compared with primary ACLR. Interestingly, female sex and higher levels of sports participation both had mixed effects on the rates of meniscectomy versus repair. Of note, BMI was a significant risk factor only for undergoing medial meniscectomy (versus repair), and this was observed only in the pediatric cohort.
The findings of the current study are similar to those of Mercurio et al, 24 who accessed the Pediatric Health Information System database and found 14,398 patients aged <18 years between 2015 and 2019 in whom a 1.24-fold increase in concomitant meniscal procedures for patients who underwent ACLR was detected as well as a 0.82-fold change in the number of meniscectomies compared with repair. Unlike the current study, the investigation by Mercurio et al did not stratify meniscal procedures by compartment (medial vs lateral). Similarly, in an IBM MarketScan database study, Block et al 4 reported a 15% increase in the use of repair compared with meniscectomy between 2006 and 2018. Finally, in a study including pediatric patients undergoing ACL reconstruction, Cruz et al 12 observed a significant positive correlation between year and rate of concomitant meniscal procedures (compared with isolated ACLR) and a significant negative correlation between year and rate of concomitant meniscectomy (compared with repair). The overall body of emerging evidence suggests that a growing proportion of pediatric and adolescent patients are presenting for ACLR with more concomitant meniscal injuries, which are increasingly being treated with repair compared with meniscectomy. This trend is likely multifactorial, as some studies have found that younger patient age and a provider's sports medicine fellowship training are associated with increased likelihood that a patient will undergo repair compared with meniscectomy.12,44 Additionally, recent advances in meniscal repair techniques have allowed for more broad indications for repair,2,9 which are likely to be preferred in younger patients in attempts to optimize long-term joint health.
These findings suggest a mixed effect of sex as a risk factor for concomitant meniscal surgeries in both cohorts. Somewhat paradoxically, female sex was predictive of medial meniscal procedures in the pediatric cohort but protective from lateral meniscal procedures in both the pediatric and adolescent cohorts. Nevertheless, these findings are similar to those of Jackson et al, 20 whose retrospective case series included 880 pediatric patients receiving meniscal surgery (45% of whom underwent concomitant ACL reconstructions). Jackson et al reported that boys were significantly more likely to have lateral meniscal tears and girls were significantly more likely to have medial meniscal tears. Other studies have reported that male patients had higher odds of undergoing concomitant meniscal procedures4,24; however, the authors of those studies did not analyze the rates of medial versus lateral meniscal procedures separately. These sex-based differences between the 2 cohorts, specific to the tibial compartment, make future investigations of pediatric and adolescent patients particularly important.
Recent studies have highlighted that pediatric and adolescent patients who undergo revision ACLR have worse outcomes than those who undergo primary ACLR.8,30 Ouillette et al 30 found that adolescent patients who underwent revision ACLR had more meniscal and cartilage damage, worse functional outcomes, and higher graft failure rates than patients who underwent their first ACLR. At the time of revision surgery, patients were also significantly more likely to have meniscal injury than patients undergoing primary ACLR. In a similar pediatric and adolescent study, Christino et al 8 also reported an increased incidence of meniscal and chondral damage in the patients’ revision ACLR compared with their primary ACLR. The findings of the current study are similar, in that adolescent patients undergoing revision ACLR were more likely to require concomitant medial meniscal surgery and that medial and lateral meniscal procedures were more likely to be meniscectomy. In the current study, the increased articular damage at the time of revision, and the need for meniscectomy as opposed to repair in the adolescent cohort, highlights the need for effective, evidence-based surgical intervention and rehabilitation at the time of initial injury to protect patients’ long-term joint health.
The current study included patient height, weight, and BMI as predictors to assess the relationship between body habitus and the need for concomitant meniscal surgeries. Of note, increased BMI was not a risk factor for undergoing meniscal procedures in either cohort, but it was a risk factor for medial meniscectomy in pediatric patients. Previous studies have shown conflicting results on the relationship between BMI and meniscal surgery in young patients, with stronger associations observed between increased BMI and medial meniscal injury.32,41 The current study also found that increased weight was predictive of concomitant lateral meniscal procedures and that increased height was associated with decreased odds of undergoing a concomitant lateral meniscal procedure in adolescent patients. The isolated effects of height and weight as variables on the risk of concomitant meniscal surgery are poorly characterized; however, Dumont et al 14 found that increased patient weight was associated with an increased rate of medial and lateral meniscal tears. The discrepancy between the findings of the current study and those of other studies, as well as the paucity of data including height and weight as predictors of injury or surgery, highlights the need for future studies to isolate what effect, if any, these variables have on the risk of concomitant meniscal surgery.
We used NLP to retrospectively identify our cohort of study patients and extract pertinent operative details for analyses. NLP has been used for medical research in a number of specialties, including orthopaedic surgery, for cohort identification and variable extraction tasks using clinical documentation.6,33-35,40,45 These techniques have been shown to be more accurate than traditional approaches (eg, diagnostic or billing code–based searches) in identifying cohorts of interest. 38 Specifically, using NLP, we were able to identify 20% more ACL surgery cases compared with using Current Procedural Terminology billing codes alone. 38 The strengths of this approach include drastically reducing the time of manual chart review and potentially reducing the administrative and logistical costs of performing database research. Weaknesses of this approach include that multi-institutional collaboration would be required to establish the external validity of these models as well as error within the model itself. However, with an adequate sample size and appropriate amount of manual review, the effects of error within the model can be minimized.
Limitations
This study is not without limitations. This was a retrospective single-center study, which may be limited by selection bias and unclear generalizability. However, the large sample size of patients seeking care across a large region over a 20-year period helps ensure a representative young, athletic subpopulation. Additionally, only patients who underwent surgery for ACL injuries were included, potentially excluding those with nonsurgical management. Importantly, these effects are minimal because the goal of the study was to characterize concomitant surgical management. Finally, we did not have access to clinical data from outside visits for patients who underwent later revision ACLR at different institutions or presented as new patients to the study institution for revision, which may have affected some conclusions.
Conclusion
Analysis of 4729 ACLR procedures performed by 8 different surgeons between 2000 and 2020 at a large academic medical center and regional referral center revealed an increase in the prevalence of concomitant lateral meniscal procedures in pediatric and adolescent patients. An increase was noted in the proportion of adolescent patients receiving medial meniscal repair, compared with meniscectomy, throughout the study period. Several risk factors for undergoing concomitant meniscal procedures were detected but with some mixed findings based on age, sex, and knee compartment. Patients undergoing revision ACLR were more likely to require concomitant meniscal procedures, particularly meniscectomy.
Footnotes
Acknowledgements
The authors thank Dr Amir Kimia, Mr Assaf Landschaft, and Ms Lanna Feldman for assisting with this study.
Final revision submitted August 9, 2023; accepted September 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Children's Hospital Orthopaedic Surgery Foundation and Boston Children's Hospital Faculty Council. B.E.H. has received education payments from Arthrex, Kairos Surgical, and Pylant Medical; consulting fees from Imagen Technologies; and nonconsulting fees from Arthrex; he holds stock for Imagen Technologies. M.S.K. has received education payments from Kairos Surgical, consulting fees from OrthoPediatrics and Ossur, nonconsulting fees from Smith & Nephew, and royalties from OrthoPediatrics, Ossur, Elsevier, and Wolters Kluwer. D.E.K. has received education payments from Kairos Surgical and consulting fees from Miach Orthopaedics and DePuy Synthes. M.D.M. has received education payments from Kairos Surgical and royalties from Saunders/Mosby-Elsevier. Y-M.Y. has received consulting fees from OrthoPediatrics and Smith & Nephew. L.M. is an unpaid consultant for Carticel. M.M.M. has received consulting fees from Miach Orthopedics and royalties from Springer and owns stock from Miach Orthopedics. A.M.K. has received consulting fees from Miach Orthopaedics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Boston Children's Hospital (ref No. IRB-P00037878).