
Abstract
Background:
Rates of anterior cruciate ligament (ACL) reconstruction among pediatric and adolescent patients are increasing. Limited knowledge exists about population-level rates of concomitant meniscal surgery in this age group.
Purpose/Hypothesis:
This study sought to examine trends in concomitant meniscal procedures and describe short-term complications in pediatric and adolescent patients undergoing ACL reconstruction. We hypothesized that overall meniscal surgery rates are increasing and that the likelihood of performing meniscal repair or meniscectomy is associated with patient- and surgeon-specific factors.
Study Design:
Cross-sectional study.
Methods:
We queried ACL procedures in patients younger than 19 years reported by American Board of Orthopaedic Surgery (ABOS) part II examination candidates from 2000 to 2016. Regression models examined associations between patient and surgeon characteristics, year of surgery, follow-up time, meniscal procedure type, and number and type of complications.
Results:
A total of 9766 cases were identified. Females represented 46% (n = 4468) of included cases. Mean patient age was 16.1 years (SD, 1.62 years; range, 0-18 years). The rate of concomitant ACL-meniscal procedures increased from the years 2000 to 2016 (49%-60%; P = .005). Surgeons with sports medicine (+7.0%) or pediatric orthopaedic fellowship (+6.6%) training had a higher likelihood of reporting a concomitant ACL-meniscal procedure (P = .003 and .006, respectively). Sports medicine–trained surgeons were more likely to perform meniscal repair compared with meniscectomy (+3.0%; P = .016). Younger patient age was associated with increased likelihood of undergoing meniscal repair compared with meniscectomy. Overall reported complication rate was 12.8%. Notable reported complications included infection (1.61%), arthrofibrosis (1.14%), and deep venous thrombosis or pulmonary embolism (0.11%). Sports medicine and pediatric orthopaedic fellowship training was associated with higher rates of reporting postoperative stiffness and/or arthrofibrosis.
Conclusion:
Among ABOS part II candidates, concomitant ACL-meniscal surgery has become more common than isolated ACL procedures. Procedures involving sports medicine fellowship–trained surgeons and younger patients were associated with increased rates of meniscal repair compared with meniscectomy. Pediatric orthopaedic and sports medicine training was associated with a greater likelihood of being involved in a concomitant ACL-meniscal procedure of any kind, and surgeons with such training also reported a higher incidence of postoperative stiffness and/or arthrofibrosis in patients.
Anterior cruciate ligament (ACL) tears are an increasingly common injury in young patients. 5,37,38 Concomitant meniscal injury is highly prevalent, with one-third to two-thirds of patients with ACL tears presenting with an associated meniscal tear. 15,18,28 Among patients with ACL tears, many risk factors have been identified for the presence of an associated meniscal tear, including patient age, sex, and time from initial injury. 4,9,10,14,21,28,31,34 Although past studies have helped elucidate the risk factors associated with concomitant ACL-meniscal injury, the optimal treatment strategy for meniscal injury in the setting of ACL reconstruction remains somewhat controversial, 28 as studies have demonstrated acceptable outcomes for both observation 6,22,30,32 and meniscal repair. 39,40 Prior studies also highlight rates of failed meniscal repair in young patients. 17,23,33 Despite the range of treatment options for meniscal tears in the setting of ACL reconstruction, limited population-level research is available that describe the general treatment trends and complications for combined ACL-meniscal procedures compared with isolated ACL procedures in pediatric patients.
The purposes of this study were to (1) examine ACL reconstruction procedures and concomitant meniscal surgeries reported by American Board of Orthopaedic Surgery (ABOS) part II candidates during their board collection period, (2) examine the rate of concomitant meniscal procedures performed in this setting over time, (3) examine the association between surgeon training and patient demographics with performance of concomitant meniscal procedure, and (4) describe the incidence and type of reported complications in these patients.
Methods
This study queried deidentified ACL procedures (Current Procedural Terminology [CPT] code 29888) in patients younger than 19 years reported by ABOS part II examination candidates from 2000 to 2016. From this group of cases, the following information was tabulated: patient age, patient sex, fellowship training of the surgeon, number and type of reported postoperative complications, follow-up duration, year of surgery, and whether 1 or more concomitant meniscal procedures were completed.
The following fellowships were tabulated: adult reconstruction, foot and ankle, hand and upper extremity, oncology, pediatric orthopaedics, shoulder and elbow, spine, sports medicine, trauma, “other,” and general orthopaedics. General orthopaedics was defined as any case record in which the reporting physician listed no fellowship (“other” was counted as a fellowship).
A meniscal procedure was defined as either a meniscal repair or a meniscectomy. A procedure was defined as a meniscectomy if labeled as CPT code 29880 or 29881. A procedure was defined as a meniscal repair if labeled as CPT code 29882 or 29883.
In addition to tabulating infections, deep venous thrombosis and/or pulmonary embolism (DVT-PE), and arthrofibrosis complications separately, we created 3 major groups of complications: (1) all reported complications, (2) surgery-related complications, and (3) anesthesia and/or medical complications excluding infections. Some of these groups included the same complications. For example, DVT-PE was deemed to qualify as “surgery-related complication (orthopaedic, vascular/coagulopathic, wound-related complications)” and “medical complication.”
Statistical Analysis
When analyzing trends in meniscal procedure type over time, we used Spearman rho statistics to test for correlations between a target year and a given procedure type (expressed as a percentage of total ACL-meniscal cases in a target year or total ACL cases in a target year). When analyzing variables associated with choice of meniscal procedure, we used naïve univariable and multivariable linear probability regression analyses. Unless otherwise specified, the term independent association, when used to describe meniscal procedure choices, refers to effects found after adjustment for differences in patient sex, patient age, and surgeon fellowship. When used to describe complications, the term independent refers to effects found after adjustment for differences in patient sex, patient age, follow-up time, whether a patient underwent concomitant meniscal surgery, and surgeon fellowship (see Appendix).
All analyses used robust standard errors and were conducted through use of Stata 15 (StataCorp LLC). Throughout all aspects of this study, statistical significance was defined as P < .05.
Results
ACL Reconstruction Procedures and Concomitant Meniscal Surgeries Reported
Our query identified 9766 ACL procedures; 46% of patients were female (n = 4468). The average age of all patients was 16.1 years (SD, 1.62 years; range, 0-18 years). Of the 9766 total ACL procedures, 53% involved 1 or more concomitant meniscal procedures (n = 5129): 22% involved meniscal repair without meniscectomy (n = 2129); 26% involved meniscectomy without meniscal repair (n = 2518); and 5% involved both meniscal repair and meniscectomy (n = 482). The mean postoperative follow-up time was 9.2 weeks (SD, 6.77 weeks; range, 0-57 weeks).
Of the patients who underwent an ACL procedure with either meniscal repair or meniscectomy (but not both meniscal repair and meniscectomy) (n = 4647 patients), 42.3% were females (n = 1967 females), and the average age was 16.1 years.
Rate of Concomitant Meniscal Procedures Performed Over Time
Trends in concomitant ACL-meniscal surgery by year and surgery type are shown in Figures 1 and 2. A statistically significant negative correlation was found between the number of isolated ACL procedures (expressed as a proportion of the total number of ACL procedures in a given year) and the year in which the ACL procedures were totaled (Spearman rho, –0.88; P < .0001). This suggests that the percentage of isolated ACL procedures decreased over time. A statistically significant positive correlation was found between the number of concomitant ACL-meniscal procedures (expressed as a proportion of the total number of ACL procedures in a given year) and the year in which the ACL procedures were totaled (Spearman rho, 0.88; P < .0001). This suggests that the percentage of concomitant ACL-meniscal procedures increased over time. A statistically significant positive correlation was found between the number of concomitant ACL–meniscal repair procedures (expressed as a proportion of the total number of concomitant ACL-meniscal procedures in a given year) and the year in which the concomitant ACL-meniscal procedures were totaled (Spearman rho, 0.95; P < .0001). This suggests that the percentage of concomitant ACL–meniscal repair procedures increased over time. A statistically significant negative correlation was found between the number of concomitant ACL-meniscectomy procedures (expressed as a proportion of the total number of concomitant ACL-meniscal procedures in a given year) and the year in which the concomitant ACL-meniscal procedures were totaled (Spearman rho, –0.96; P < .0001). This suggests that the percentage of concomitant ACL-meniscectomy procedures decreased over time.

Trends in total isolated anterior cruciate ligament (ACL) vs total concomitant ACL-meniscal surgery, by year of procedure. The y-axis represents the target case type expressed as a proportion of the total number of ACL procedures completed in a given year.

Trends in type of concomitant meniscal surgery, by year of procedure. The y-axis represents the target case type expressed as a proportion of the total number of concomitant anterior cruciate ligament (ACL)-meniscal procedures completed in a given year.
Association Between Surgeon Training and Patient Demographics With Performance of Concomitant Meniscal Procedure
All results reported below are adjusted for differences in patient age and patient sex.
Pediatric Orthopaedic Fellowship
Pediatric orthopaedic fellowship–trained surgeons had a statistically significant higher rate (+6.6%) of reporting a concomitant ACL-meniscal surgery of any kind (meniscal repair, meniscectomy, or both) compared with an isolated ACL procedure (P = .006). Among patients receiving concomitant ACL-meniscal surgery (with either meniscal repair or meniscectomy, but not both), pediatric orthopaedic fellowship training was not associated with a higher or lower probability of performing meniscal repair (vs meniscectomy) (P = .762).
Sports Medicine Fellowship
Sports medicine fellowship–trained surgeons had a statistically significant higher rate (+7.0%) of reporting a concomitant ACL-meniscal surgery of any kind (meniscal repair, meniscectomy, or both) compared with an isolated ACL procedure (P = .003). Sports medicine fellowship–trained surgeons also had a statistically significant higher rate (+3.0%) of reporting a concomitant ACL-meniscal surgery with both meniscectomy and meniscal repair (P = .016). Among patients receiving concomitant ACL-meniscal surgery (with either meniscal repair or meniscectomy, but not both), sports medicine fellowship–trained surgeons had a statistically significant higher rate (+11.2%) of reporting a meniscal repair instead of a meniscectomy (P = .002).
General Orthopaedic Training
General orthopaedic training was not statistically significantly associated with ACL-meniscal surgery of any kind (meniscal repair, meniscectomy, or both) compared with an isolated ACL procedure (P = .422).
Was Patient Age Associated With Certain Procedures?
Figure 3 shows the frequency of concomitant ACL-meniscal surgery (meniscal repair, meniscectomy, or both) versus isolated ACL surgeries by patient age. Age was not statistically significantly associated with a patient’s likelihood of receiving concomitant ACL-meniscal surgery (meniscal repair, meniscectomy, or both) (P = .107). These results held after adjustment for differences in patient sex (P = .452) and after adjustment for differences in both patient sex and surgeon fellowship training (P = .146).

Distribution of concomitant meniscal surgery, by age.
Among patients who underwent concomitant ACL-meniscal surgery (with either meniscal repair or meniscectomy, but not both), older age was negatively associated with a patient’s likelihood of undergoing meniscal repair (vs meniscectomy) (Figure 4). For each increased year of age, a patient had a statistically significant lower probability (–2.2%) of receiving concomitant ACL–meniscal repair surgery (P < .01). This finding held after adjustment for differences in both patient sex and surgeon fellowship training: For each increased year of age, a patient had a statistically significant lower probability (–1.9%) of undergoing meniscal repair (as opposed to meniscectomy) (P < .01). In this analysis, patients younger than 12 years were excluded because of the relatively low numbers in the data set (<30 ACL procedures per age group in those ≤11 years old). These low numbers are consistent with other investigations’ reported rates of ACL injury in pediatric patients. 3,5

Trends for anterior cruciate ligament (ACL)-meniscal repair vs ACL-meniscectomy, by age in patients 12 years or older.
Incidence and Type of Reported Complications in Patients
Table 1 shows the number of complications (tabulated from all reported complications) for the entire cohort. Only complications with higher than 1.0% reported rate are shown. Surgery-related complications were reported in 11.08% of cases and, of these, infection and stiffness-arthrofibrosis were the most common (1.61% and 1.14%, respectively).
Reported Complications a
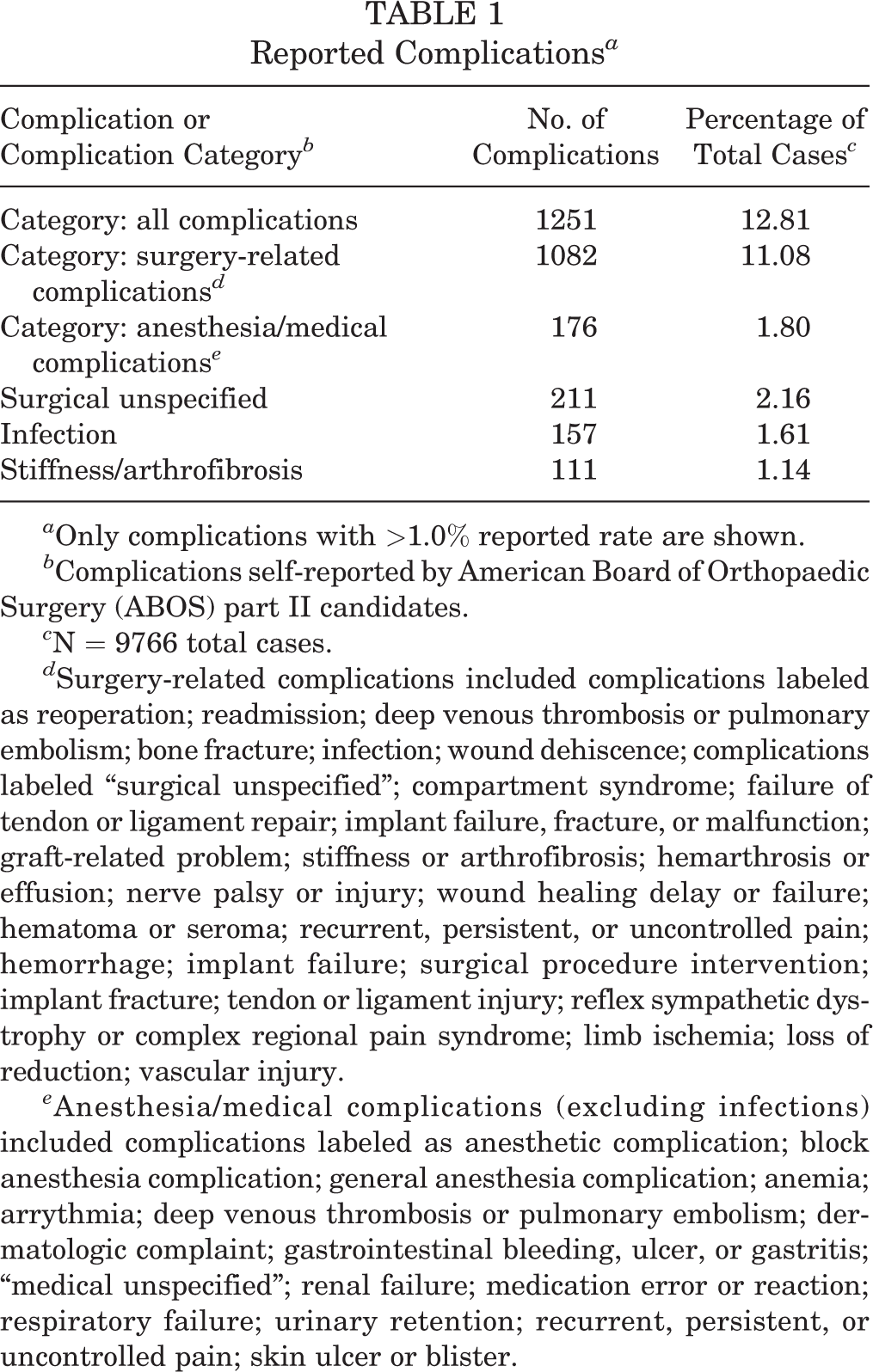
a Only complications with >1.0% reported rate are shown.
b Complications self-reported by American Board of Orthopaedic Surgery (ABOS) part II candidates.
c N = 9766 total cases.
d Surgery-related complications included complications labeled as reoperation; readmission; deep venous thrombosis or pulmonary embolism; bone fracture; infection; wound dehiscence; complications labeled “surgical unspecified”; compartment syndrome; failure of tendon or ligament repair; implant failure, fracture, or malfunction; graft-related problem; stiffness or arthrofibrosis; hemarthrosis or effusion; nerve palsy or injury; wound healing delay or failure; hematoma or seroma; recurrent, persistent, or uncontrolled pain; hemorrhage; implant failure; surgical procedure intervention; implant fracture; tendon or ligament injury; reflex sympathetic dystrophy or complex regional pain syndrome; limb ischemia; loss of reduction; vascular injury.
e Anesthesia/medical complications (excluding infections) included complications labeled as anesthetic complication; block anesthesia complication; general anesthesia complication; anemia; arrythmia; deep venous thrombosis or pulmonary embolism; dermatologic complaint; gastrointestinal bleeding, ulcer, or gastritis; “medical unspecified”; renal failure; medication error or reaction; respiratory failure; urinary retention; recurrent, persistent, or uncontrolled pain; skin ulcer or blister.
After adjustment for differences in patient age, patient sex, follow-up duration, and whether a patient underwent concomitant ACL-meniscal surgery, pediatric orthopaedic fellowship training was associated with a statistically significant higher probability (+1.85%) of reporting a stiffness- and/or arthrofibrosis-related complication (P = .016). No increased risk of reporting other types of complications was found. When cases with stiffness-arthrofibrosis complications were excluded, and after adjustment for differences in patient age, patient sex, follow-up duration, and whether a patient underwent concomitant ACL-meniscal surgery of any kind, pediatric orthopaedic fellowship training was no longer statistically significantly associated with a higher or lower probability of reporting of a complication (P = .169).
Sports medicine fellowship training was also associated with a statistically significantly increased probability (+1.91%) of reporting a stiffness-arthrofibrosis complication (P = .008). As with pediatric orthopaedic fellowship training, sports medicine fellowship training was not statistically significantly associated with a higher or lower probability of reporting any other subset of complication. No other fellowship training was statistically significantly associated with a higher or lower probability of stiffness- and/or arthrofibrosis-related complications.
Discussion
In this study, we found that 53% of ACL procedures performed in patients younger than 19 years reported by ABOS part II candidates from 2000 to 2016 involved 1 or more concomitant meniscal procedures. This is higher than the 20% rate reported by Westermann et al 40 in a multicenter retrospective study of primary ACL reconstruction procedures from 2002 to 2004. When examining trends in concomitant ACL-meniscal surgery over time in the current study’s cohort, we found that the proportion of ACL procedures that involve concomitant meniscal surgery has increased (see Figure 1). This finding among ABOS part II candidates may reflect a wider trend of increasing rates of concomitant ACL-meniscal procedures in more recent years and is consistent with recent literature examining primary ACL reconstruction. 1,11,14,20,27,41
The meniscus is an important structure for maintenance of long-term knee health, and therefore, attempts to preserve the meniscus or minimize damage to it are important. 2,7,8,16,19,26,29 Decisions on how to optimally treat a meniscal tear in the setting of an ACL reconstruction are based on several factors including tear shape and location, tear chronicity, patient age and activity level, and perhaps even surgeon training. Wyatt et al 41 examined patients in whom a meniscal injury was diagnosed during primary ACL reconstruction. The authors found that among 5712 primary ACL reconstruction procedures, surgeon sports medicine fellowship training (in addition to younger patient age, lower patient body mass index, and higher surgeon and site case volume) was independently associated with increased likelihood of meniscal repair. When examining fellowship training, the results of the current study show that both pediatric orthopaedic training and sports medicine fellowship training were associated with an increased likelihood of concomitant ACL-meniscal procedures (repair or meniscectomy), whereas only sports medicine fellowship training was associated with an increased likelihood of repair. Tagliero et al, 36 evaluating pediatric and adolescent patients who underwent concomitant meniscal repair during ACL reconstruction, reported good long-term success rates (defined as failure-free survival) in 72% of patients. Our findings of a significant association between fellowship training and concomitant ACL-meniscal procedures may reflect a bias in surgeon training or may reflect the relatively young patient cohort examined (<19 years old), which may bias treating surgeons toward performing repair. In fact, when we analyzed age and procedure choice, patient age was not statistically significantly associated with a patient’s likelihood of undergoing concomitant ACL-meniscal surgery; however, of the patients undergoing ACL-meniscal surgery (involving either meniscal repair or meniscectomy, but not both), younger patients were more likely to undergo meniscal repair instead of meniscectomy (Figure 4).
Complications
When we analyzed fellowship training, pediatric orthopaedic training was independently associated with a higher likelihood of reporting stiffness- and/or arthrofibrosis-related complications. These results are consistent with other authors’ findings. Nwachukwu et al 24 retrospectively examined the rate of postoperative arthrofibrosis following ACL reconstruction in a cohort of children and adolescents (mean age, 15 years; range, 7-18 years). The authors reported an 8.3% prevalence of arthrofibrosis and found that female sex, age 16 to 18 years, patellar tendon autograft, and concomitant meniscal repair were risk factors for development of arthrofibrosis.
Regression analysis suggested that sports medicine fellowship training was also statistically significantly associated with a higher risk of stiffness- and/or arthrofibrosis-related complications. One contributing factor to the increased risk in stiffness-arthrofibrosis complications may be the association between sports medicine fellowship–trained surgeons and their increased likelihood of being involved in meniscal repairs over meniscectomies. Many postoperative physical therapy protocols differ between patients undergoing meniscal repair compared with meniscectomy or isolated ACL surgery, 25,35 which may be reflected by the increased rate of stiffness-arthrofibrosis. Unfortunately, because of the nature of the data, more detailed case-level characteristics that may have accounted for this finding—such as total surgical time, time from initial injury, or other indicators of case complexity—could not be examined.
It is reasonable to expect that pediatric orthopaedic and sports medicine–trained surgeons are more likely to treat higher complexity pediatric sports-related knee cases than surgeons of other subspecialty training (including general orthopaedic surgery). As a result, one may expect complication rates to be upwardly biased among pediatric orthopaedic and sports medicine–trained surgeons. This is supported by the fact that no other fellowship training demonstrated a statistically significant association with stiffness- and/or arthrofibrosis-related complications.
Limitations and Future Research
This study has several limitations. First, the data analyzed were queried from ABOS part II certification examination candidates and, as a result, are reliant on the self-reporting of examinees. Second, ABOS Part II examinations evaluate the work of orthopaedic surgeons who are relatively early in their practice, and the trends and complications reported by these surgeons represent a relatively small sample compared with orthopaedic surgeons in general. Third, the available ABOS data are missing major determinants of procedure indications and complication rates. For example, the data set used does not describe case complexity, meniscal tear patterns, idiosyncratic patient-related difficulties, or specific surgical techniques used. As a result, although the modeling in this study describes associations, it should not be used as a predictive model, nor should the associations be interpreted in a causal manner. Fourth, because the ABOS part II case collection period is restricted to 6 months, the follow-up periods for the reported cases are limited, and therefore true complication rates (particularly medium- and long-term complications) may be underestimated in this study. Longer term follow-up would be expected to produce higher complication and reoperation rates, as shown in prior studies. 12,13 However, we did adjust for follow-up time when examining complication rates in comparative statistical analyses.
Conclusion
This study examined 9766 ACL procedures reported by ABOS part II candidates from 2000 to 2016 and showed an increased rate of combined ACL-meniscal surgeries compared with isolated ACL surgeries in recent years. Pediatric orthopaedic and sports medicine fellowship–trained surgeons are more likely to perform concomitant ACL-meniscal surgery compared with other types of fellowship-trained or general orthopaedic surgeons. Stiffness- and/or arthrofibrosis-related complications are major contributors to short-term complication rates observed by surgeons who perform ACL-meniscal procedures.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.I.C. has received educational support from Arthrex. T.J.G. has received educational support from Arthrex and Liberty Surgical and research support from Allosource and Vericel. A.T.P. has received educational support from Sportstek, consulting fees from OrthoPediatrics, and hospitality payments from Smith & Nephew and has stock/stock options in Imagen. K.G.S. has received research support from Allosource, Sanofi-Aventis, and Vericel; consulting fees from HealthTrust; and hospitality payments from DePuy. J.J.B. has received educational support from Arthrex and research support from DJO. H.B.E. has received educational support from Pylant Medical and hospitality payments from Smith & Nephew and Synthes. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
Appendix
After tabulation, naïve univariable and multivariable regression analyses were conducted through use of Stata 15. Robust standard errors were used. Statistical significance was defined as P < .05. The specifications used are shown in Tables A3, A4, and A7-A11.
In each of these specifications, the dependent variables are shown in the first row of each table, and the regressors used are shown in the first column.
The general regression equation used for these regressions is as follows: