
Abstract
Background:
Recent studies have reported conflicting results as to whether isolated medial patellofemoral ligament reconstruction (MPFLr) leads to decreased patellar height.
Purpose:
To investigate if patellar stabilization surgery not intended to address patella alta influences patellar height.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A multicenter retrospective chart review was conducted, and patients who underwent MPFLr, medializing tibial tuberosity osteotomy (TTO), and/or trochleoplasty between 2016 and 2020 were included. The Caton-Deschamps index (CDI) was calculated from radiographs obtained preoperatively, 2 weeks postoperatively, and 3 months postoperatively. The preoperative CDI value was compared with the 2-week postoperative and 3-month postoperative values according to stabilization procedure (isolated MPFLr, isolated TTO, MPFLr + TTO, MPFLr + trochleoplasty, and MPFLr + trochleoplasty + TTO) using the paired t test. Analyses of the 1-bundle versus 2-bundle MPFLr technique and the presence of lateral retinacular release or lateral retinacular lengthening were conducted on the isolated MPFLr and combined MPFLr + TTO cohorts.
Results:
A total of 356 knees were included. Statistically significant pre- to postoperative decreases in CDI were seen in all stabilization procedures analyzed (P≤ .017 for all). Within the isolated MPFLr cohort, this significant decrease was seen at 2 weeks postoperatively with the 2-bundle technique (ΔCDI = −0.09; P < .001) but not with the 1-bundle technique (ΔCDI = −0.01; P = .621).
Conclusion:
The different surgical techniques analyzed in the current study affected patellar height, even when a distalizing TTO was not performed. The decrease was dependent on surgical technique, with a 2-bundle MPFLr leading to a statistically significant decrease and a 1-bundle MPFLr effecting no change.
Patellar instability has an incidence of 5.8 cases per 100,000 people, with the highest rates occurring in the young, active population.12,19,20 These dislocations can cause substantial morbidity due to cartilaginous injury, fracture, pain, decreased functionality, and patellofemoral arthritis.1,12,14,19,23,26,34 First-time dislocations are typically treated nonoperatively.12,17,29 After a second dislocation, recurrence rates are >50%,1,12 and stabilization surgery is typically considered. 39 The best choice of surgical procedure has traditionally depended on a variety of anatomic factors and is the subject of controversy. 39
The medial patellofemoral ligament (MPFL) is the most important medial restraint of the patella from 0° to 30° of flexion.4,7,18 More than 90% of lateral dislocations involve disruption of the MPFL. 33 Therefore, MPFL reconstruction (MPFLr) is typically performed for recurrent instability. 35 This procedure can be performed with a 1-bundle or 2-bundle technique, meaning the graft is secured to the patella at 1 or 2 points, respectively.
The lateral retinaculum contributes about 10% of the lateral stability of the patella. 3 When the retinaculum is abnormally tight, patellar maltracking can occur. 13 This is treated surgically with either a lateral retinacular release (LRR) or lateral retinacular lengthening (LRL).
Patella alta is a risk factor for patellar instability, as the patella engages the trochlear groove later in knee flexion. This condition can be quantified with a variety of measures, one of which is the Caton-Deschamps index (CDI). CDI is defined as A/B, where A is the distance from the anterior angle of the tibial plateau to the most inferior aspect of the patellar articular surface and B is the length of the patellar articular surface (Figure 1). A value of >1.2 is indicative of patella alta.2,27 Current literature recommends a distalizing tibial tubercle osteotomy (TTO) to decrease patellar height in the setting of recurrent instability and alta with a CDI >1.4.2,10,27,39 However, distalizing osteotomy is not benign, as it is associated with complications including tibial fracture, nonunion, and painful hardware. 22
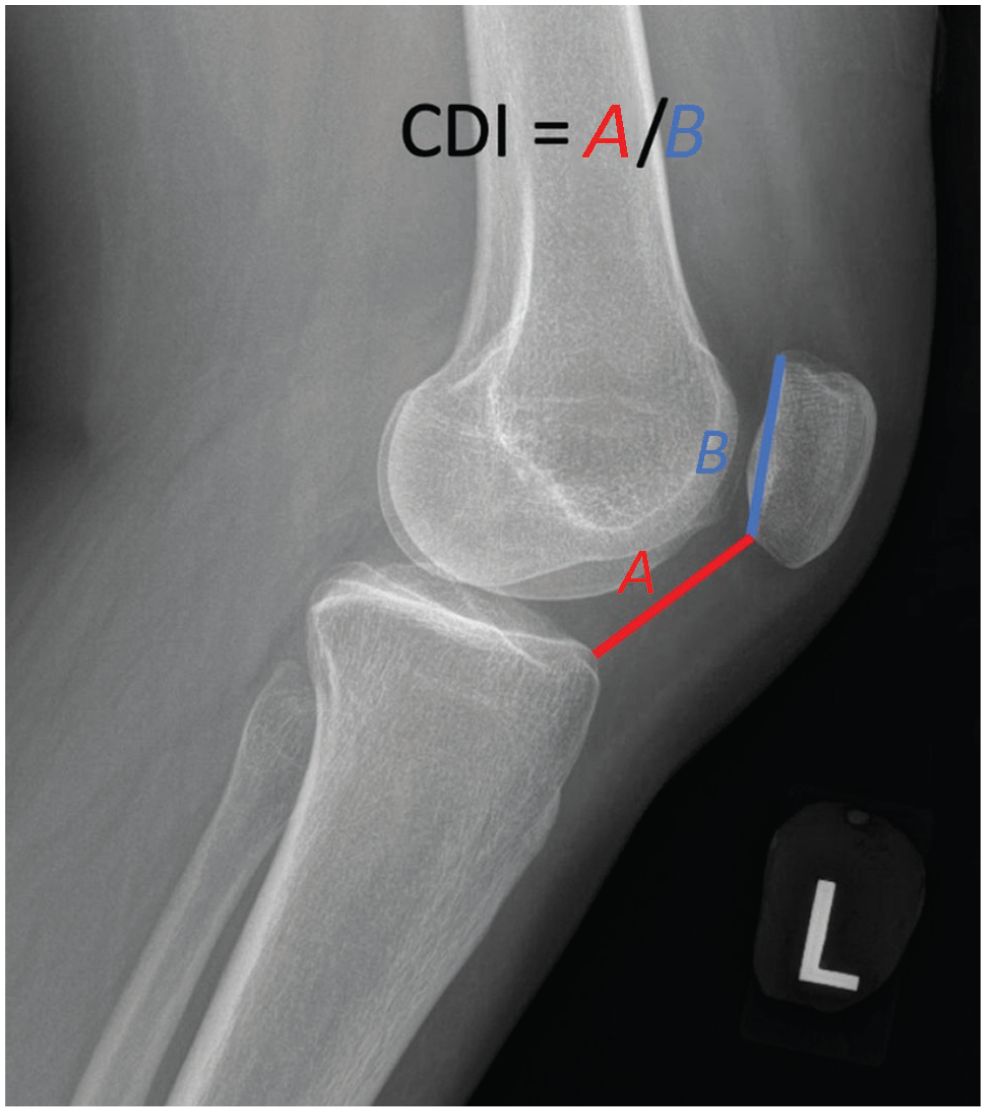
Figure demonstrating the Caton-Deschamps index (CDI), where A is the distance from the inferior patellar articular surface to the anterior and superior tibial plateau, and B is the length of the patellar articular surface.
An excessively lateralized tibial tuberosity creates a lateral force vector through the extensor mechanism that predisposes to instability. One way to quantify tuberosity position is tibial tuberosity–trochlear groove (TT-TG) distance, which is the distance between a line bisecting the tibial tuberosity and another bisecting the trochlear groove sulcus.8,36 A TT-TG distance of >15 to 20 mm is associated with instability.6,31 An excessively lateralized tuberosity can be treated surgically with a medializing TTO.15,16,38
Trochlear dysplasia causing an abnormally shallow or convex groove can predispose to instability. It has been reported that 85% of knees with recurrent instability have some degree of trochlear dysplasia. 6 This can be treated by deepening trochleoplasty, or surgical reshaping of the trochlear groove. Indications are not well established but include a TT-TG of >10 mm and a J-sign 5 and radiographs demonstrating prominent trochlear convexity as evidenced by the trochlear floor crossing anterior to the lateral femoral condyle.6,9
There is controversy in the literature as to whether isolated MPFLr can lead to decreased patellar height. Some prior studies have shown a postoperative decrease in patellar height.11,24,25 However, another study showed no difference in patellar height indices. 32 Prior studies examined only isolated MPFLr and did not analyze the impact of osteotomy or LRR/LRL.
The purpose of the current study was to evaluate the effect of patellar instability surgery, including MPFLr, medializing TTO, and trochleoplasty, on patellar height. Our goal was to provide information that would help during preoperative planning to determine whether concomitant distalizing osteotomy will be necessary. We hypothesized that patellar stabilization procedures that were not performed to address patella alta would decrease patellar height.
Methods
A retrospective review was performed to identify all patients who underwent MPFLr, medializing TTO, and/or trochleoplasty performed by the attending surgeons at 4 institutions (A.J.C., M.J.T., D.R.D., L.D.F.) between 2016 and 2020. Institutional review board (IRB) approval to retrospectively collect patient data and review radiographs was obtained at all 4 institutions. To qualify for the study, patients had to have undergone MPFLr, medializing TTO, and/or trochleoplasty for patellar instability. All patients who underwent the aforementioned procedures were considered for inclusion. Patients were excluded for missing radiographs, for insufficient lateral radiograph quality, and if pre- or postoperative data were missing. Inividual patient informed consent was waived by each institution’s IRB.
Lateral knee radiographs were used to calculate the CDI. A sufficient lateral radiograph was defined as one with the knee in 15° to 65° of flexion and with <8 mm of overhang of the femoral condyles (Figure 2). These criteria were chosen by the senior authors (M.J.T., L.D.F., D.R.D., A.J.C.) as acceptable parameters, as there is no agreed-upon definition of an acceptable lateral radiograph. Patients with radiographs that fell outside these parameters were excluded.

Radiograph of a patient who was excluded from the study because the postoperative radiograph did not meet inclusion criteria due to excessive condylar overlap.
Surgical Procedures
Patients were indicated for surgery by each institution's attending surgeon. Surgical technique varied by attending surgeon. MPFLr was conducted using a 1- or 2-bundle technique depending on surgeon preference. The femoral tunnel was placed at the Schöttle point and the patellar tunnels were placed to create an isometric graft. Reconstructions were performed with allograft or autograft hamstring tendons based on surgeon preference (Figure 3). Each surgeon performed medializing TTO by creating a shingle around the tibial tuberosity and greensticking the fragment at its distal attachment. To preserve vascular supply, complete release of the shingle was avoided by all surgeons. Patients undergoing distalizing osteotomies were excluded from the study.

(A) Single-bundle MPFLr technique using a single transverse socket. (B) Two-bundle MPFLr technique utilizing 2 suture anchors. (C) Two-strand MPFLr technique with horizontal tunnels and gracilis autograft. Reconstruction technique varied by surgeon preference. MPFLr, medial patellofemoral ligament reconstruction.
Data Collection
Data collection, including radiographic analysis, was performed by a senior orthopaedic resident (postgraduate year 4 or 5) or fellowship-level trainee at each institution (R.T.K., G.A., S.Y., M.S.F.). Patient and surgical technique data were collected (age at time of surgery, surgeon, surgical procedure performed, TTO translation distance, 1- or 2-bundle MPFLr technique, and whether an LRR or LRL was performed). The CDI on preoperative, 2 week–postoperative, and 3 month–postoperative radiographs were also evaluated. Per surgeons’ protocols, patients who underwent isolated MPFLr had only 2 week–postoperative radiographs, as there was no need to assess osteotomy healing. The surgeon reviewing the images could not be blinded to the procedure given the presence of hardware and drill tunnels visible on postoperative radiographs. Interobserver agreement could not be calculated because of cross-institution IRB restrictions, but this radiographic measurement technique has been previously shown to have high interobserver reliability.37,40
The primary outcome of our study was the change between the preoperative and postoperative CDI (ΔCDI) of the different patellar instability procedures. An exploratory analysis was also performed in order to examine differences between the 1-bundle and 2-bundle MPFLr techniques, the presence of LRR/LRL, and the amount of TTO translation during medialization.
Statistical Analysis
Data set diagnostics included review of skewness and kurtosis for the CDI measurement. All met assumption of a normal distribution. We used dependent (paired) samples t test to compare the preoperative CDI values with the 2 week–postoperative (isolated-MPFLr cohort) and 3 month–postoperative (all other cohorts) values. Analyses of the 1- versus 2-bundle techniques and the presence of LRR/LRL were conducted on the isolated MPFLr and combined MPFLr + TTO cohorts using the independent-samples t test. Change scores, which provide a summary measure of the mean change in a variable between 2 time points, were used to compare preoperative and postoperative CDI values. The correlation between TTO medialization and patellar height measures was determined for the isolated-TTO cohort, in order to minimize confounding variables including additional surgeries. The Pearson product-moment correlation coefficient (r) was used for bivariate associations. For all comparisons, differences were considered statistically significant at P≤ .05. Statistical analyses were performed with IBM SPSS Statistics for Windows, Version 28.0 (IBM Corp), 2021 release.
Results
A total of 356 knees were included, with a mean age of 24.0 years (range, 10-62 years). The procedures included were as follows: 128 patients underwent isolated MPFLr, 71 patients underwent isolated TTO, 107 underwent MPFLr with TTO, 32 underwent MPFLr with trochleoplasty, and 18 patients underwent MPFLr with TTO and trochleoplasty. No patient underwent isolated trochleoplasty or TTO and trochleoplasty without MPFLr.
Surgical technique influenced the change observed in CDI (Table 1). Specifically, when looking at isolated MPFLr, a statistically significant decrease at 2 weeks postoperatively was seen in the 2-bundle cohort (ΔCDI = −0.09 [95% CI, −0.14 to −0.04]; P < .001) but not in the 1-bundle cohort (ΔCDI = −0.01 [95% CI, −0.14 to 0.12]; P = .621). This pattern was also seen in the MPFLr + TTO cohort: at 3 months postoperatively, the 2-bundle cohort (ΔCDI = −0.12 [95% CI, −0.18 to −0.06]; P < .001) had a significant decrease that was not observed in the 1-bundle cohort (ΔCDI = −0.02 [95% CI, −0.12 to 0.08]; P = .300). Change scores decreased whether or not an LRR/LRL was performed in either the isolated-MPFLr or the MPFLr + TTO cohorts (Table 1).
Comparison of Pre- and Postoperative CDI for All Analyzed Cohorts a
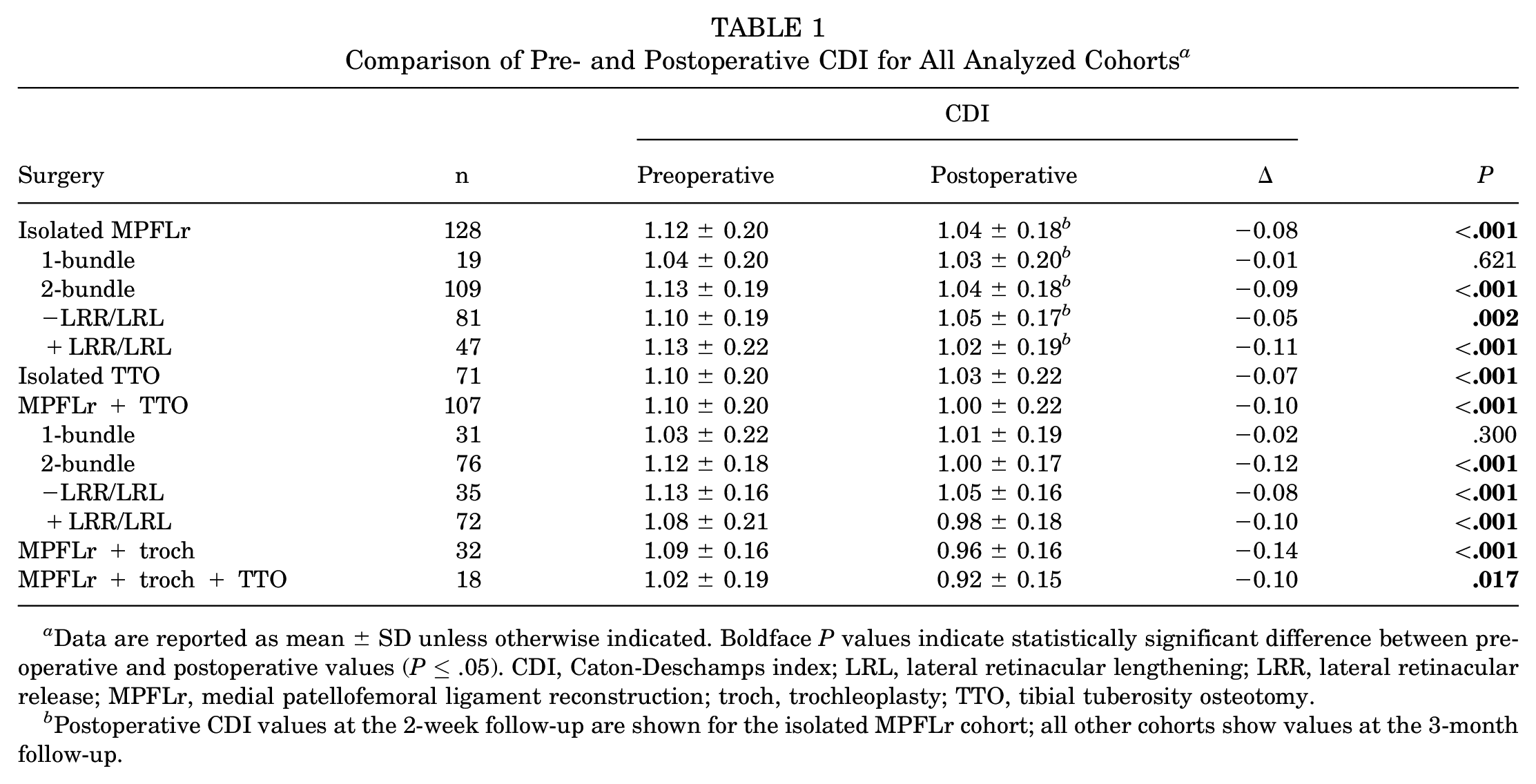
Data are reported as mean ± SD unless otherwise indicated. Boldface P values indicate statistically significant difference between preoperative and postoperative values (P≤ .05). CDI, Caton-Deschamps index; LRL, lateral retinacular lengthening; LRR, lateral retinacular release; MPFLr, medial patellofemoral ligament reconstruction; troch, trochleoplasty; TTO, tibial tuberosity osteotomy.
Postoperative CDI values at the 2-week follow-up are shown for the isolated MPFLr cohort; all other cohorts show values at the 3-month follow-up.
When a medializing TTO was performed, the shingle was medialized between 10 and 15 mm. The results of the correlation analysis indicated that there was no significant association between the amount of medialization and change in CDI (Table 2).
Correlation Between Amount of Medialization and Changes in CDI for Patients Who Underwent Isolated Medializing TTO (n = 63 Patients) a

A total of 8 patients who had 3-month follow-up radiographs but lacked 2-week follow-up radiographs were excluded from this analysis. CDI, Caton-Deschamps index; TTO, tibial tuberosity osteotomy.
Discussion
The results of our multicenter study demonstrated that patellar stabilization surgery led to unintentional decreases in the CDI, except in patients undergoing isolated 1-bundle MPFLr. This decrease was influenced by MPFLr surgical technique, with a statistically significant decrease in preoperative to 2-week postoperative CDI in the 2-bundle cohort (ΔCDI = −0.09 [95% CI, −0.14 to −0.04]; P < .001) but not the 1-bundle cohort (ΔCDI = −0.01 [95% CI, −0.14 to 0.12]; P = .621). Neither concomitant lateral retinacular release, lateral retinacular lengthening, nor TTO affected patellar height.
Other studies have analyzed patellar height after patellar stabilization surgery not intended to lower the patella. Luceri et al 24 studied skeletally mature patients with mild patella alta (CDI between 1.20 and 1.40) undergoing isolated MPFLr using a 2-bundle technique. In 95 knees (89 patients) with a mean age of 25.0 years, a significant reduction in CDI was observed postoperatively (Δ = −0.19; P < .00001) at a mean follow-up of 18.4 months. In their series, there was a moderate correlation between the severity of the patella alta and the observed reduction in CDI. Based on these data, the authors concluded that distalization procedures are not indicated in cases of patellar instability and a CDI between 1.20 and 1.40. 24 The specific description of the surgical technique and, in particular, the position of the patellar tunnel were not reported.
Lykissas et al 25 examined adolescent patients undergoing MPFLr using a 1-bundle technique. In 38 knees with a mean age of 14.2 years, a significant reduction in CDI was seen postoperatively (Δ = −0.14; P < .001) at a mean follow-up of 6 months. This cohort was compared with a group of patients undergoing surgery for osteochondritis dissecans. In the osteochondritis dissecans group there was no significant decrease in CDI. The authors concluded that isolated MPFLr decreases patellar height in adolescent patients. 25
Fabricant et al 11 also studied an adolescent population undergoing MPFLr with a 2-bundle technique. In 27 knees with a mean age of 14.9 years, CDI decreased by −0.22 (P < .001) at a mean follow-up of 3 months. 11 Similar to Lykissas et al, 25 the authors concluded that MPFLr in adolescents decreases patellar height.
However, not all studies investigating the effect of MPFLr on patellar height have shown a decrease in patellar height. Roessler et al 32 examined an adult population also undergoing MPFLr with a 2-bundle technique. In a study of 32 knees with a mean age of 29.7 years, no statistically significant difference in CDI was observed. This study also examined Insall proximal realignment, which also did not affect CDI. 32 The authors concluded that MPFLr does not affect patella alta.
The decrease in CDI in our cohort was seen with 2-bundle, but not 1-bundle, MPFLr technique, a difference that may be related to graft attachment position at the patella. The tension of the MPFL graft is anisometric. More proximal patellar MPFL graft insertions demonstrate more isometric behavior than distal insertions. 21 It is unclear at this time whether attachment site affects CDI postoperatively.
The effect of LRR/LRL on patellar height has not been established in patellofemoral stabilization surgery. Murayama et al 28 examined the effect of LRR during opening wedge high tibial osteotomy (OWHTO). In their cohort of 37 knees, OWHTO with LRR led to no change in CDI, while isolated OWHTO led to a decrease in patellar height, suggesting that LRR may increase patellar height. 28 In our cohort, CDI decreased whether or not LRR/LRL was performed.
Nondistalizing TTO has been shown to alter patellar contact pressures and decrease the Q-angle. 30 However, the effects on patellar height have not been definitively established. Our data demonstrated no correlation between the amount of TTO shingle medial translation and patellar height change. The range of shingle translation was also small (10-15 mm), so it is possible that the measurements made from plain radiographs were not sensitive enough to detect a true difference.
Strengths and Limitations
This study has several strengths. It examines patellar stabilization procedures other than MPFLr, giving surgeons valuable information on the effects of MPFLr, medializing TTO, and trochleoplasty performed either in isolation or together. In addition, the multicenter nature of our study allowed us to examine potential factors that influence the observed decrease in patellar height. Namely, we were able to demonstrate the effects of additional operations (medializing TTO and trochleoplasty), 1- versus 2-bundle surgical technique, LRR/LRL, and medial translation of the shingle during TTO on patellar height. Finally, it is the largest patient cohort published to date, with 356 knees.
Any study should also be viewed within the context of its limitations. Each surgeon in our study used either a 1- or a 2-bundle MPFLr technique, so we could not compare the 1- versus 2-bundle technique for each surgeon. Each surgeon also made an individual decision as to whether or not to perform an LRR/LRL. While all surgeons had patients who did or did not undergo LRR/LRL, it is possible indications varied across surgeons. Also, typical postoperative protocols for all 4 surgeons did not include imaging beyond 2 weeks after isolated MPFLr. Imaging beyond 2 weeks in the other cohorts was obtained to assess osteotomy healing and was therefore not needed for isolated MPFLr. Although limitations within our IRB approvals did not allow for images to be viewed across institutions, meaning that interobserver reliability could not be calculated, we have previously demonstrated high interobserver reproducibility with the radiographic measurement protocols utilized in this study. 37 Nonetheless, this is a potential source of error. As there is no published definition of a sufficient lateral radiograph, we developed one based on the expert opinion of the 4 attending surgeons in this study. However, we realize that this method could be either overly restrictive or inclusive.
Additionally, tunnel position could affect graft tensioning and potentially patellar height. While we considered evaluating tunnel position, because the postoperative radiograph was not always perfectly perpendicular to the tunnel, it was not possible to accurately determine its position. Moreover, the range of medialization during TTO was only 10 to 15 mm. It is possible that this range was not great enough to detect a change in CDI. As with any retrospective study, we were limited by the number of patients who met the inclusion criteria. It is possible that the sample size may have been too small to detect certain differences. We also had more patients in the 2-bundle cohort than the 1-bundle MPFLr cohort, which could have affected our ability to detect patellar height differences in the 1-bundle cohort. Finally, postoperative radiographs were obtained primarily to assess MPFLr tunnel position and TTO shingle healing, so there was not a high degree of scrutiny placed on obtaining perfect lateral radiographs to assess patellar height.
Nonetheless, we believe this study provides clinicians with valuable information that informs surgical decision making when treating patients with patellar instability. Patellar instability is multifactorial, and patella alta affects other anatomic risk factors such as lateralized tuberosity and trochlear dysplasia because greater degrees of knee flexion are required before the patella is engaged in the bony stability deep in the trochlear groove. Understanding how patellar height will change following patellar stabilizing procedures may influence decisions regarding the need for distalization of the tibial tuberosity. Further studies are needed to provide a biomechanical reason behind the different effects of 1- versus 2-bundle MPFLr on patellar height, as well as to further elucidate the clinical superiority of either technique.
Conclusion
The results of this study indicated that patellar instability surgery can affect patellar height, even when distalizing TTO or patellar tendon shortening are not performed. Surgeons can expect a decrease in CDI of 0.09 when a 2-bundle MPFLr is performed. Surgeons can factor this degree of shortening of the patellar height into decision-making regarding whether or how much to distalize the patella in the setting of patella alta. The amount of shingle translation during TTO did not affect patellar height, and a decrease was seen with or without LRR/LRL.
Footnotes
Acknowledgements
The authors acknowledge Christa Librizzi, MD, for contributions to the figures in this article. They also thank Denise Di Salvo, MS, Sandra Crump, MPH, and Rachel Box, MS, in the Editorial Services group of the Johns Hopkins Department of Orthopaedic Surgery, for editorial assistance.
Final revision submitted August 16, 2023; accepted September 8, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: G.A. has received education payments from Arthrex and Medical Device Business Services and hospitality payments from Exactech. M.S.F. has received education payments from Kairos Surgical. M.J.T. has received education payments from Kairos Surgical and Supreme Orthopedic Systems. L.D.F. has received hospitality payments from DJO. D.R.D. has received consulting fees from DePuy Synthes, Medical Device Business Services, and OsteoCentric Technologies and royalties from OsteoCentric Technologies and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Cleveland Clinic (ref No. 21-623), Johns Hopkins Medicine (ref No. IRB00266398), University of Virginia (ref No. 22690), and Massachusetts General Hospital.