
Abstract
Background:
In patients with valgus alignment and degenerative changes in the lateral compartment, both distal femoral osteotomy (DFO) and high tibial osteotomy (HTO) can be used to unload the lateral compartment. Prior studies have shown that in valgus knees, the tibial wear is posterior and DFO exerts the greatest effect in extension; however, its effect is decreased as flexion angle rises.
Hypothesis:
Medial closing-wedge (MCW) HTO would significantly decrease contact area, mean contact pressure (MCP), and peak contact pressure (PCP) in the lateral knee compartment through knee flexion to a greater extent compared with lateral opening-wedge (LOW) DFO.
Study Design:
Controlled laboratory study.
Methods:
MCWHTO and LOWDFO were performed, correcting a mean of 8° of valgus alignment, in 10 cadaveric knees using plate fixation. Tibiofemoral contact pressure of the medial and lateral compartments was measured in 0°, 30°, 60°, and 90° of knee flexion before and after osteotomy using thin electronic sensors and load applied through an Instron device. PCP, MCP, and contact area were measured for each condition.
Results:
The lateral MCP was significantly decreased in the HTO state compared with the native state in 30° (P = .015), 60° (P = .0199), and 90° (P < .0001) of flexion. The lateral MCP was also significantly decreased in the HTO state when compared with the DFO state in 60° (P = .0093) and 90° of flexion (P < .0001). After DFO, the lateral MCP returned to that of the native state in 60° (P > .999) and 90° (P > .999) of flexion. The lateral PCP decreased for all test states in all degrees of flexion; the HTO state was significantly decreased when compared with the native state in 60° (P < .0001) and 90° (P < .0001).
Conclusion:
With varus corrections of 8°, MCWHTO was more effective at unloading the lateral compartment than LOWDFO. This effect was significant as the knee flexion angle increased. This study should be considered as one aspect of the surgical decision-making process.
Clinical Relevance:
In patients with mild to moderate valgus deformity without hypoplastic lateral femoral condyle and without significant joint line obliquity, MCWHTO may improve offloading of the lateral compartment in flexion.
Periarticular knee osteotomies have long been an established treatment for various pathologies in patients with coronal plane malalignment.3,4,17,18,26 Interest has increased in using these procedures in the setting of cartilage restoration and meniscal transplant procedures to optimize the biomechanical environment of the recipient knee during these surgeries. Neutral mechanical alignment is an important factor in the success of these operations, and interest has increased in using osteotomies to achieve this goal.9,11,26 In patients with valgus malalignment and a preserved medial compartment, a lateral opening-wedge (LOW) distal femoral osteotomy (DFO) or a medial closing-wedge (MCW) high tibial osteotomy (HTO) is considered for realignment.
Although DFOs have long been considered the standard for treatment of valgus with lateral compartment disease, these techniques preferentially affect joint contact forces in full extension with less effect at greater knee flexion angles and no effect at 90° or beyond.3,4,25 Quirno et al 20 biomechanically tested the ability of LOWDFO to unload the lateral compartment when a 10° valgus force was applied. 18 The authors found that when the knee was in full extension, a 10° correction was able to reliably unload the lateral compartment. Recently, Wylie et al 25 further explored the effect of LOWDFO on cadaveric knee models in varying stages of knee flexion and found that the osteotomy was able to unload the lateral compartment, with the greatest unloading effect in full knee extension. Additionally, Wylie et al found that LOWDFO more effectively decreased contact pressure in the more anterior aspects of the femoral articular cartilage. The current literature has shown that lateral compartment pathology preferentially affects the posterior joint during deeper knee flexion angles, as demonstrated in lateral compartment arthritis and after partial lateral meniscectomy.8,21
In contrast to LOWDFO, the MCWHTO may provide an advantage of altering joint biomechanics in both flexion and extension. 4 As the knee is brought to higher angles of flexion, the unloading benefit of LOWDFO is reduced, given that the correction is in the coronal plane only. MCWHTO offers the benefit of effectively lowering the medial joint line without affecting the anteroposterior diameter of the femoral condyles and preserving the flexion arc.1,4 Currently, no study is available in the literature that directly compares the biomechanical effects on the lateral knee compartment after LOWDFO versus MCWHTO. A comparison between these techniques would aid in the surgical decision-making process when assessing the expansive list of considerations at play.
The purpose of this study was to directly compare how LOWDFO and MCWHTO affect tibiofemoral joint pressure and joint contact area and to evaluate how the compartment pressures and contact area change as the knee is brought into higher flexion angles. We hypothesized that MCWHTO would significantly decrease contact area, mean contact pressure (MCP), and peak contact pressure (PCP) in the lateral knee compartment through knee flexion to a greater extent than a similar LOWDFO. We also hypothesized that as flexion angle increased, the unloading benefit of LOWDFO would be lost and the compartment pressure and contact area would return to near-native state.
Methods
Power Analysis
Ten cadaveric specimens were needed to have 80% power to detect a difference in MCP of 0.1 MPa. Calculations were based on data from 2 prior DFO biomechanical studies where 2-way analyses of variance for each condition in 3 treatment groups with 6 samples per group resulted in a power of 83%.20,25
Specimen Preparation
The specimens used were donated to a tissue bank for medical research and then purchased by our institution. All specimens were left-side, fresh-frozen, human cadaveric knees (mean age, 53.3 years; range, 39-64 years) and were stored at –20°C and thawed overnight before testing. The specimens each contained 15 cm of distal femur and 15 cm of proximal tibia and were dissected down to the joint capsule with removal of the skin, subcutaneous tissue, patella, patellar tendon, and fat pad. The use of cadaveric specimens does not require institutional review board approval at our institution.
The specimens were individually evaluated to confirm no degenerative changes and to confirm integrity of medial meniscus, lateral meniscus, and cruciate ligaments and the absence of significant anatomic variants (hypoplastic lateral femoral condyle, significant joint line obliquity, significant varus or valgus malalignment). Specimen criteria included age 18 to 65 years, no osteoarthritis, no cancer to bone, and no previous surgeries or other joint pathology.
Surgical Osteotomy Technique
With the femur and tibia still in the native state, a Synthes Tomofix lateral DFO plate and a Synthes Tomofix medial HTO plate (DePuy Synthes) were secured to the lateral femur and distal tibia, respectively. The plates were then removed and the osteotomies performed (Figure 1).

Radiographic images of osteotomy states mounted to the loading fixture. Both osteotomies were performed on the same specimen to ensure a repeated-measures study design. Shown are the opening wedge distal femoral osteotomy (DFO) (left), the native state (center), and the closing wedge high tibial osteotomy (HTO) (right).
The opening-wedge DFO was performed using an 18-mm oscillating saw blade (Stryker) and a 1-inch osteotome. The osteotome was introduced approximately 2 to 3 fingerbreadths proximal to the lateral epicondyle following a trajectory aimed just proximal to the medial epicondyle, with preservation of the medial femoral hinge. The 8° varus correction was then completed and secured with the Synthes Tomofix lateral DFO plate (Figure 1).
The closing-wedge HTO was then performed using the same 18-mm oscillating saw blade and 1-inch osteotome. The instrument was introduced approximately 3 to 4 fingerbreadths distal to the medial tibial plateau and followed a trajectory aimed toward the tip of the proximal fibula. A subsequent 8° varus correction was then completed and secured with a Synthes Tomofix medial HTO plate. The distal tibia was then embedded in poly(methyl methacrylate) (Fricke Dental).
Radiographic Assessment
Fluoroscopy was used on each specimen in the native state, HTO state, and DFO state to calculate the medial proximal tibial angle (MPTA) as well as the anatomic lateral distal femoral angle (aLDFA) (Figure 2). The MPTA was calculated by measuring the angle between a line going through the midshaft of the tibia and a line tangential to the proximal tibia articular surface. 15 The aLDFA was created between a line going through the midshaft of the distal femur and centered in the femoral canal and a line tangential to the articular surface of the femur. 15 Radiographs were obtained only in the 0° of flexion position, and measurements were reported as means and standard deviations.

Radiographic assessment of osteotomy states: anatomic lateral distal femoral angle (aLDFA) and medial proximal tibial angle (MPTA).
Mechanical Testing
Equilibrated electronic pressure sensors (K-scan Model 4000, 1500 psi; Tekscan Inc) were installed under the meniscus in the lateral and medial compartments, and the anterior and posterior ends of the sensors were sutured and tethered to screws anchored to the tibia to ensure consistent placement of the sensors during all trials and to ensure reproducibility of pressure measurements (Figure 3). The pressure-mapping sensors were calibrated by performing manufacturer-defined calibrations at 20% of the expected maximum pressure and 80% of the expected maximum pressure. At each loading value, cork (3-mm thickness) cylinder with a contacting surface area of 314 mm2 and capped with a layer of silicone 30 was applied to the pressure sensor, and a power calibration was performed per the manufacturer's specifications. The sensors allowed the measurement of pressures from 0.1 to 172 MPa with an accuracy of 0.1 MPa. The sensor model is 0.1 mm thick and comprises 2 measuring fields, each with an area of 33 × 22 mm and a spatial resolution of 0.1 mm.
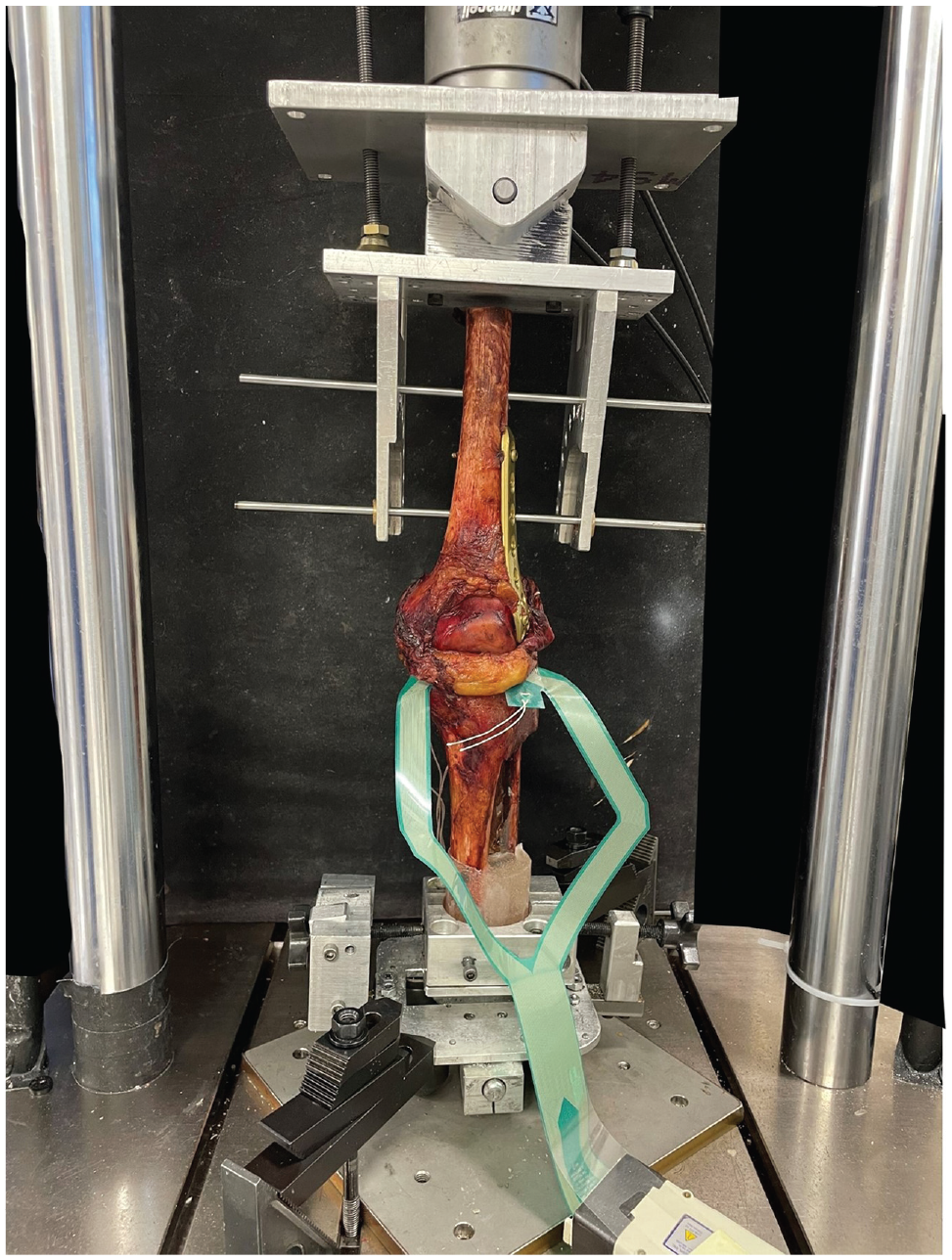
Mechanical setup with Tekscan pressure sensors installed submeniscally.
Each specimen received 2 osteotomies, an HTO and a DFO, and both osteotomy states were tested on the same specimen. The order of each osteotomy state was randomized via a custom MATLAB (Version R2021a; The MathWorks) script. If DFO was selected to be tested first, the femoral plate would be secured with the femur in the osteotomy-corrected position, whereas the tibial plate would be secured so that the tibia returned to the native state. If the HTO state was selected first, the tibia would be secured to the plate in the osteotomy-corrected position, whereas the femoral plate would be secured with the femur in the native state; if the native state was selected first, both the tibial and femoral plate would be secured to the femur and tibia in the native state. To ensure that contact mechanics were not affected when transitioning a specimen from the native state (ie, anatomic alignment and position with both the tibial and femoral plate secured in place) to a varus-producing osteotomy or from a varus osteotomy state back to the native state, the compartment pressures and contact area to the medial and lateral compartment were assessed before any plate fixation and compared those results to the native state both before and after an osteotomy had been performed (Figure 4).

Diagrams of mechanical testing setup and specimen alignment for (A) native alignment, (B) HTO alignment, and (C) DFO alignment. aLDFA, anatomic lateral distal femoral angle; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; MPTA, medial proximal tibial angle.
The specimen was initialized to its first osteotomy state and rigidly fixed in a custom apparatus mounted to a biaxial materials testing machine (Instron Electropuls 10000). The femur was secured to the upper fixture simulating a fixed hip joint, with the ability to abduct and adduct only, by sliding 2 stainless steel rods through the proximal femur. The upper fixture, fixed to the end effector of the materials testing machine, enabled the specimen to rotate freely in the coronal plane and allowed the specimen's flexion angle to be changed. The potted tibia was fixed to the lower fixture that enabled the tibia to rotate freely in the coronal plane and translate freely in the anterior-posterior direction. The specimen was initially positioned in 0° of flexion and loaded to 300 N of compression at a rate of 20 N/s. The final load was held for 10 seconds, a snapshot of the contact pressure map was recorded, and then the specimen was unloaded to 20 N of compression. This loading protocol was repeated for a total of 2 trials per testing condition at 0°, 30°, 60°, and 90° of flexion. After the specimen had been tested at all flexion angles, the osteotomy was switched to the other osteotomy state (from DFO to HTO or from HTO to DFO), and the testing protocol was repeated (Figure 4).
Statistical Analysis
The 2 trials of the contact pressure maps were exported for each specimen at each osteotomy state at each flexion angle and analyzed using a custom MATLAB script. Three primary outcomes were computed for the lateral and medial compartments: MCP (mean of all nonzero Tekscan cells), PCP (mean of the highest 20% of pressure sensels), and contact area. The results of the 2 trials were averaged for each test.
Shapiro-Wilk tests were used to verify normal distribution of contact area, MCP, and PCP data. At a significance level of α = .05, 2-tailed analyses of variance were applied to check for significant differences in lateral and medial contact area, MCP, and PCP between native, HTO, and DFO groups at each flexion angle (R version 4.1.2; R Core Team, 2021). Tukey post hoc tests were applied to make pairwise comparisons between means of native, HTO, and DFO groups at each flexion angle.
Results
We found no difference in force or contact area between the presurgical specimen and the native state (P = .863) after the osteotomies had been performed.
Radiographic Analysis
Radiographic analysis showed a mean aLDFA of 83.9°± 2.02° before correction. After an 8° varus-producing LOWDFO, the mean aLDFA was 89.8°± 2.21°. Before correction, the mean MPTA was 80.6°± 1.43°, and after an 8° varus-producing MCWHTO, the mean MPTA was 85.6°± 1.82°. The opening-wedge angle of osteotomy was a mean of 7.93°± 2.21°, whereas the closing-wedge angle of osteotomy was 7.58°± 1.02°.
Mean Compartment Pressure
In the medial compartment, MCP in the DFO state was not significantly different from MCP in the native state at all flexion angles. MCP in the HTO state was significantly higher than MCP in the native state and in the DFO state at 60° (native, P < .0001; DFO, P = .015) and 90° (native, P < .0001; DFO, P = .044) of flexion (Figure 5). At 0° and 30° of flexion, MCP in the HTO state was not significantly different from MCP in the native state or the DFO state.

Mean (A) medial compartment and (B) lateral compartment pressure at each flexion angle for the native state (blue), high tibial osteotomy (HTO) state (red), and distal femoral osteotomy (DFO) state (yellow). Error bars indicate standard deviations. For each flexion angle, P values comparing differences between states are reported.
In the lateral compartment, MCP in the DFO state was not significantly different from MCP in the native state at all flexion angles. MCP in the HTO state was significantly lower than MCP in the native state at 30° (P = .015). MCP in the HTO state was significantly lower than MCP in the native state and in the DFO state at 60° (native, P = .020; DFO, P = .009) and 90° (native, P < .0001; DFO, P < .0001) of flexion (Figure 5). At full extension, MCP in the HTO state was not significantly different from MCP in the native state or the DFO state. At 30° of flexion, MCP in the HTO state was not significantly different from MCP in the DFO state.
Peak Compartment Pressure
In the medial compartment, PCP in the DFO state was not significantly different from PCP in the native state or the HTO state at all flexion angles. PCP in the HTO state was significantly higher than PCP in the native state at 90° of flexion (P = .030) (Figure 6). At 0°, 30°, and 60° of flexion, PCP in the HTO state was not significantly different from PCP in the native state.

Peak (A) medial compartment and (B) lateral compartment pressure at each flexion angle for the native state (blue), high tibial osteotomy (HTO) state (red), and distal femoral osteotomy (DFO) state (yellow). Error bars indicate standard deviations. For each flexion angle, P values comparing differences between states are reported.
In the lateral compartment, PCP in the DFO state was not significantly different from MCP in the native state at all flexion angles. PCP in the HTO state was significantly lower than MCP in the native state at 60° (P < .001) and 90° (P < .001) of flexion (Figure 6). PCP in the HTO state was significantly lower than MCP in the DFO state at 60° of flexion only (P = .007). At 0° and 30° of flexion, PCP in the HTO state was not significantly different from PCP in the native state or the DFO state.
Contact Area
In the medial compartment, contact area in the DFO state was not significantly different from contact area in the native state at all flexion angles. Contact area in the HTO state was significantly higher than contact area in the native state and the DFO state at 30° (native, P < .0001; DFO, P < .0001), 60° (native, P < .0001; DFO, P < .0001), and 90° (native, P = .043; DFO, P = .028) of flexion (Figure 7). At full extension, contact area in the HTO state was not significantly different from contact area in the native state or the DFO state.

(A) Medial and (B) lateral compartment contact area at each flexion angle for the native state (blue), high tibial osteotomy (HTO) state (red), and distal femoral osteotomy (DFO) state (yellow). Error bars indicate standard deviations. For each flexion angle, P values comparing differences between states are reported.
In the lateral compartment, contact area in the DFO state was significantly lower than contact area in the native state at 30° of flexion only (P = .046) (Figure 7). At all other flexion angles, contact area in the DFO state was not significantly different from contact area in the native state. Contact area in the HTO state was not significantly different from contact area in the DFO state at all flexion angles. Contact area in the HTO state was significantly lower than contact area in the native state at 30° (P = .043) and 90° (P = .027) of flexion (Figure 7). At 0° and 60° of flexion, contact area in the HTO state was not significantly different from contact area in the native state.
Discussion
The main finding of this biomechanical study was that MCWHTO was able to unload the lateral compartment more effectively compared with LOWDFO. This effect was amplified at higher degrees of flexion. Additionally, we found that both the lateral compartment contact pressure and medial compartment contact area returned to near-native states in higher flexion angles. We found no differences in lateral compartment pressure and contact area after varus-producing HTO and DFO in full extension. Although a prior study have reported a joint line obliquity of up to 10° to be acceptable, 2 other biomechanical studies have shown that even 4° of medial joint line obliquity can lead to significant elevations in pressure to the lateral compartment and significant medial translation of the distal femur.1,5,24 Increased forces in the lateral compartment were also found in our study.
From a historical perspective, both LOWDFO and MCWHTO have been used for >50 years in the treatment of valgus malalignment and lateral compartment overload. 23 Much of the initial research in this area did not directly compare osteotomy techniques and unreliably recorded joint line obliquity and/or presence of lateral condyle hypoplasia.5,12,13,20 In 1969, Jackson et al 12 described that HTO was a safe and reliable treatment option for osteoarthritis of the knee. A few years later, Shoji and Insall 22 reported that the results of a varus-producing HTO were inferior to those of a valgus-producing osteotomy and that knees undergoing a varus HTO with obliquity >15° did poorly. In 1973, Coventry 5 stated that a distal femoral varus-producing osteotomy was preferable to a varus-producing HTO when the valgus deformity exceeded 12° and when joint line obliquity exceeded 10°. In 1985, Maquet 14 reported that for patients undergoing surgery for valgus malalignment, a supracondylar osteotomy of the femur was unquestionably much better than a tibial osteotomy. This statement was based on his own outcomes in addition to the perception that tibial osteotomies result in a large amount of force on the medial portion of the lateral tibial plateau, whereas femoral osteotomies result in a completely even distribution of forces. 13
More recently, we have gained a better understanding of patient selection and surgical technique as they relate to periarticular osteotomies for valgus malalignment. Finkelstein et al 7 performed a survivorship analysis evaluating varus-producing DFO and found a 10-year survivorship of 64%. Additionally, Healy et al 10 and McDermott et al 16 found favorable results after distal femoral varus osteotomy for valgus deformity and reported improvement in pain.
Although relatively limited long-term clinical outcomes after MCWHTO have been reported, they overall demonstrate positive results. Chambat et al 3 reported a series of 47 patients with 10-year follow-up who underwent MCWHTO for valgus malalignment. The authors reported that 72% of patients reported “good” to “very good” results at 10 years. 3 Chambat et al concluded that the ideal correction is to about neutral, joint line obliquity must be <10° of valgus, and younger patients with mild arthritis had better outcomes. Coventry 6 reported on 31 patients after MCWHTO. The author reported that at a mean follow-up of 9.4 years, 77% of patients had no pain or mild pain, 19% of patients had moderate pain, and 1 patient had severe pain. Six knees required conversion to total knee arthroplasty at a mean of 9.8 years after osteotomy. Puddu et al 19 reported on 6 cases with excellent improvement of pain and functional capabilities.
Although the results of the current study favor using MCWHTO over LOWDFO for the purpose of offloading the lateral compartment and decreasing lateral compartment contact area, these results should not be broadly applied to all patients with lateral compartment overload and valgus malalignment. Concern continues to exist for development of medial collateral ligament laxity after MCWHTO. Our study used an intended correction of 8°, which was an estimated amount of correction to return nonphysiologic valgus to physiologic valgus based our clinical experience and a prior study reporting favorable outcomes. 3 Although it would be reasonable to assume that larger corrections may result in even greater offloading potential and amplification of the results, we believed that knees requiring a greater amount of correction would have a higher likelihood of having additional anatomic variants (hypoplastic lateral femoral condyle, significant joint line obliquity, absence of medial collateral ligament or lateral meniscus) that were not controlled for in our current study. Moreover, our data showed that MCWHTO was able to reliably offload the lateral compartment and transfer this load to the medial compartment. Although this is often the intended consequence of using this osteotomy location, the act of transferring too much load to the medial compartment may unintentionally also transfer the accelerated wear to the medial compartment. Additionally, in the setting of a significantly elevated lateral distal femoral angle and in the setting of lateral femoral condyle hypoplasia, performing MCWHTO places the patient at high risk of increased joint line obliquity and medial subluxation or translation of the distal femur.
Limitations
The present study is not without its limitations. First, without complete hip, knee, and ankle joints, the specimen's mechanical axis was approximated. To address this limitation, the end effector of the materials testing machine was approximately aligned to the mechanical axis of the knee via a custom fixture that simulated the hip and ankle joints. Second, to ensure repeated-measures design of the study, the native state included all osteotomy cuts before testing, though complete native anatomic positioning was maintained. Third, the custom fixture that secured the specimen to the materials testing machine enabled movement and loading only within the coronal plane. Although the custom fixture that secured the specimen to the materials testing machine replicated the degrees of freedom in the ankle and hip within the coronal plane, it did not enable loading or movement in the other planes. We did not measure or account for the effects of bony alignment within other degrees of freedom. Fourth, muscle tension was not included in this cadaveric model. A fifth limitation was the unknown native anatomic axis of the specimen being tested. Although the tested specimens did not have excessive lateral compartment degenerative changes or extremes of malalignment, we believe that this study's design and the ability to individually assess and compare each specimen in varying osteotomy states provided an internal control that would allow a clinician to draw the reasonable conclusion that MCWHTO can better unload the lateral compartment as the knee is taken throughout knee flexion. The submeniscal placement of the Tekscan pressure sensors required that the anterior and posterior meniscotibial ligaments be cut. Although this windowing does not affect the tibiofemoral contact, local contact measurements may be affected by interference from surrounding tissue. Sixth, skin, subcutaneous tissue, and muscles were removed from the specimen, possibly affecting the forces at play.
Conclusion
This study demonstrated that MCWHTO was able to unload the lateral compartment more effectively compared with LOWDFO at higher flexion angles. This finding should be considered as one aspect of the surgical decision-making process, with precise deformity analysis being performed on a case-by-case basis. In patients with mild to moderate valgus deformity without hypoplastic lateral femoral condyle and without significant joint line obliquity, MCWHTO may improve offloading of the lateral compartment in flexion.
Footnotes
Final revision submitted July 17, 2023; accepted August 29, 2023.
Presented at the AOSSM Annual Meeting, Washington DC, July 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.L. has received grants from Arthrex; education payments from Arthrex, Impact Ortho, Smith & Nephew, and Southtech Orthopedics; and hospitality payments from Stryker. C.S. has received grants from DJO and education payments from Smith & Nephew and Medinc of Texas. M.F. has received grants from Arthrex and education payments from Arthrex and Smith & Nephew. A.V. has received education payments from Gemini Mountain Medical, consulting fees from Arthrex and Stryker, nonconsulting fees from Arthrex and Smith & Nephew, honoraria from Vericel, and hospitality payments from Bodycad. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.