
Abstract
Background:
Low back pain (LBP) is a common condition that can affect athletes of all ages. The risk factors for LBP onset and worsening associated with the lacrosse shooting motion are not yet known.
Purpose:
To identify training and biomechanical factors associated with preexisting LBP and development of LBP over 6 months in youth, high school, and collegiate lacrosse players.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 128 lacrosse players were enrolled in this study between January 2016 and January 2019. Player characteristics, lacrosse experience, and participation in other sports were self-reported. At baseline and 2-, 4-, and 6-month follow-ups, the players self-rated the presence and severity of LBP using a numeric pain rating scale (0-10 points). Participants were grouped according to LBP symptoms: no LBP at any time point (n = 102), preexisting LBP (n = 17), or developed LBP within the 6-month period (n = 9). The lacrosse shooting motion was captured via 3-dimensional motion analysis, and kinematic and kinetic variables were recorded. A Low Back Stress Index was used to estimate lumbar stress as a function of pelvic acceleration at the time of maximum lateral trunk lean during the shot. Univariate analyses of covariance and logistic regression models were used to address study aims.
Results:
Compared with the no-LBP group, the preexisting LBP group demonstrated 13.9% to 22.9% lower maximum angular velocities at the pelvis, trunk, and shoulders in the transverse plane (P < .05), 19.3% less collective pelvis-shoulder rotation in the transverse plane (P = .015), and 4.5% more knee flexion excursion (P = .063). The developed-LBP group produced 2.3% to 11.1% higher angular velocities in the pelvis, trunk, and shoulder and generated maximum pelvic acceleration values 36% to 42% higher than the remaining groups (P < .05 for both). Mean Low Back Stress Index values were not statistically significant among the groups (no LBP: 12,504 ± 13,076 deg2/s2; preexisting LBP: 8808 ± 10,174 deg2/s2; developed LBP: 19,389 ± 13,590 deg2/s2; P = .157).
Conclusion:
Preexisting LBP was associated with significantly restricted motion of the pelvis, trunk, and shoulders during a lacrosse shot. Excessive pelvic acceleration may be related to the development of LBP in lacrosse players.
Low back pain (LBP) is one of the most common musculoskeletal issues in the United States. The lifetime prevalence of LBP in the general adult population is estimated at 85% to 90%. 23 In the athletic population, LBP occurs in approximately 10% to 15% of young athletes and up to 30% in athletes with developed musculoskeletal systems. 10 A concerning trend is that pain episodes recur in young athletes with overuse-related back injuries at a rate of 26% to 33%. 4
Lacrosse is a complex sport involving high-velocity rotation movements about the spine. Epidemiological lacrosse studies have found that acute injuries commonly occur in the sport, but chronic musculoskeletal injuries can also develop.16,27 Back/trunk pain has been reported in 2.8% to 14.2% of youth, high school, and collegiate-level lacrosse players.12,16 A key movement in this sport is the overhead throw, which is used for passing, clearing, and shooting to score. The overhead motion and variations of this motion are repeated in high volumes during practice, drills, scrimmage, and shooting practice.
From our observations of youth through collegiate teams, we estimate the volume of shooting/throwing during different preparatory sessions to range from 40 to >70 depending on player age and field position. Like other throwing or swinging motions that produce fast ball speed,2,29 a fast lacrosse shot is produced through a generation of high angular velocities of body segments along the kinetic chain and optimal transfer of that energy from the foot plant to ball release.17,30 Several factors can affect torque development at joints or the timing of the mechanics, including the presence of musculoskeletal pain. The lumbar spine and associated musculature transfer energy from the lower to the upper body via sequential rotations of the pelvis, trunk, and shoulders.26,28,30 During a lacrosse shot, these same body segments are involved with the acceleration and deceleration of the upper body and arms while using a long lever arm to release the ball. If the resultant repetitive forces acting on the body are not dissipated through appropriate movement technique and sequencing, the low back torsional loads increase and pain can follow.20,32
From an injury prevention perspective, chronic issues may be mitigated if the mechanisms underlying the pain are better understood. Concerning back pain, we previously characterized biomechanics of the shooting motion among high school and collegiate lacrosse players with chronic LBP. 28 In this small study, we detected rotation restrictions in the trunk and shoulder and slower ball speeds during the shooting motion compared with players with no LBP. 28 A limitation of our previous study was that it could not be determined whether specific risk factors of lacrosse playing experience or mechanical shooting features were related to the onset of pain, or if LBP modified the biomechanics. Potential playing experience factors related to LBP include lack of participation in other sports, all-year play (specialization), and player position with different shooting volumes (offense vs defense). Midfielders and attack are most often the shooting positions on the field, and LBP may develop over time due to repetitive, high-velocity mechanical stresses at the spine.28,29 A lack of participation in sports other than lacrosse may hinder the optimization of movement coordination and dynamic strengthening of the musculature supporting the spine. 13 Concerning biomechanical technique, LBP in other high-speed rotational sports (eg, golf) is characterized by high trunk rotation, lateral trunk bending, and restricted shoulder-to-pelvis crossover during the backswing or crank back. 6 Additional evidence is needed to better understand which features of playing experience and biomechanical technique are present among lacrosse players with current LBP and those who develop LBP over time. These findings will inform injury prevention strategies and provide insight into the impact of LBP on shooting performance.
There were 2 purposes to this study. First, we sought to determine differences in lacrosse shooting biomechanics among players with preexisting LBP and those who developed LBP over 6 months. We hypothesized that high pelvic and trunk rotational velocities and acceleration would contribute to the development of LBP and that players with existing LBP would have restricted pelvic and trunk rotational excursions and slower maximum angular velocities of the pelvis and trunk compared with those without LBP and those who develop LBP. Second, we sought to determine the associations between LBP, player characteristics, and lacrosse playing experience. We hypothesized that (1) those playing in field positions with high shooting volumes (midfield or attack) would have higher odds of having preexisting LBP and developing LBP than those playing in positions that shoot less (defense) and (2) players involved in other sports than lacrosse would have a lower risk of LBP than players involved only in lacrosse.
Methods
Study Design and Participants
Data were merged from 2 previously unpublished cohort studies of lacrosse players. Our institutional review board approved the protocols for these studies. Parental consent/child assent for youth and high school players and informed consent for participants aged ≥18 years were obtained after the study details and potential risks were reviewed. A total of 128 lacrosse players (mean age, 16.4 ± 3.0 years; height, 169.0 ± 13.0 cm; weight, 64.1 ± 15.0 kg) with any level of lacrosse experience were recruited using study flyers, online notices, and word of mouth. The study enrollment period was January 2016 to January 2019. The number of participants was chosen to allow stratification of the results based on age, sex, and player position (attack, midfield, or defense) for statistical analysis; a large number is necessary for meaningful analysis. The inclusion criteria for the studies were male and female players between 10 and 21 years of age who played lacrosse in organized school/university teams. Criteria for exclusion were individuals aged <10 or >21 years and those currently being treated for an acute injury (eg, new sprain, strain, fracture, or concussion).
Outcome Measures
Participant Characteristics and Playing Experience
Age was self-reported. Height and weight were obtained using a medical-grade stadiometer. Players self-reported other sports besides lacrosse (if any) in which they participated during the previous year. A multisport athlete was defined as playing ≥2 sports in the past year. A study-specific survey was developed to determine key information about the lacrosse playing experience of each participant. Questions were administered electronically using REDCap. 11 The survey included questions relating to years of play, current weekly frequency of lacrosse practice sessions or games, and the number of seasons played per year (single season, 2 seasons, or all-year play). Positions were categorized into midfield, attack, defense, and >1 position. Players also reported whether they had changed positions during the past year.
Pain Severity
The self-reported occurrence of any lower body musculoskeletal pain was rated using an 11-point numeric pain rating scale (0 = no pain, 10 = worst imaginable pain). Participants were asked to rate their average pain over the previous week separately at the lumbar spine, hips, knees, ankles, and feet. The lumbar spine was the primary pain site studied and discussed in this study. The numeric pain rating scale is a valid, reliable, and responsive outcome measure with established minimal clinically important difference values. 24 Pain scores were collected at baseline and 2, 4, and 6 months after baseline through follow-up telephone calls. Pain scores were collected in these intervals to capture any players who experienced early pain or pain onset with seasonal changes in training volume, as has been shown to occur in baseball players and runners.18,19
Participants with no LBP at any time point were considered the no-LBP group, those who reported LBP at baseline were included in the preexisting LBP group, and those who reported no LBP at baseline and subsequently reported LBP at any follow-up time point were designated as the developed-LBP group.
Motion Analysis
The lacrosse shooting motion with the dominant arm was captured using a high-speed, 12-camera optical motion-capture system (Motion Analysis Corp). The details of this technique and the determination of body segment calculations we developed have been previously published. 25 Motion data were captured at 200 Hz. Reflective markers were applied to the following anatomic landmarks: right scapula (offset), acromion processes, lateral epicondyles of the elbow, midway between the ulnar and radial styloid processes, third metacarpals, posterior superior iliac spines, anterior superior iliac spines, greater trochanters, lateral femoral epicondyles, lateral malleoli, heels, and the halluces. Markers and reflective tape were also placed on the stick end of the crosse and the crosse shaft. Only reflective tape was used on a lacrosse ball with the standard National Operating Committee on Standards for Athletic Equipment stamp. Figure 1 shows the computer model view in Cortex software (Motion Analysis Corp).
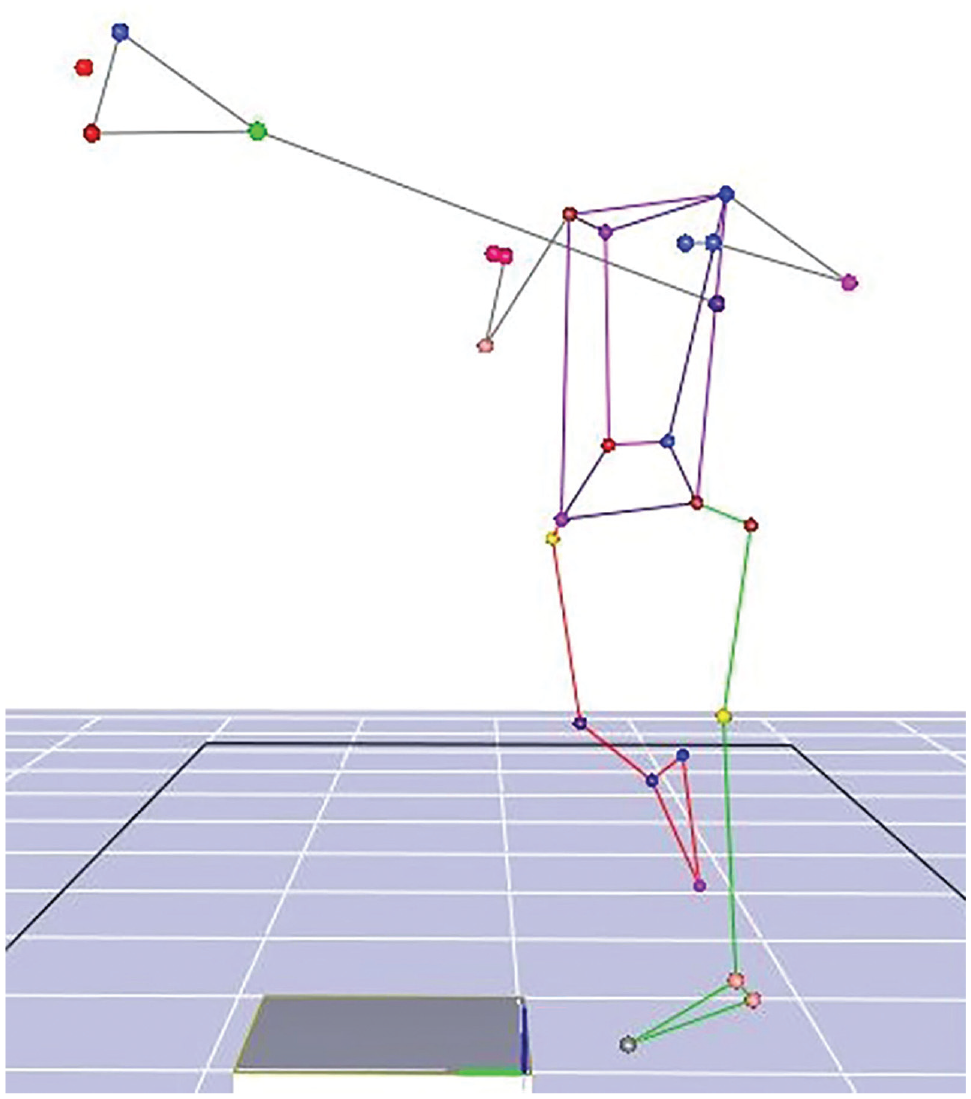
Still image of 3-dimensional computer model of lacrosse player after ball release during a shot.
After a 5-minute warm-up of throwing the ball at a target, participants performed overhead shots with their dominant arm within the camera capture volume area. Participants used their personal crosses that they would typically use for their primary playing position (ie, longer pole for defense). The dominant arm was defined as the arm the participant used to write. The overhead shot was selected because it is a fundamental skill of the sport and is easily replicated by players; comprises a relatively high volume of the high-speed, rotational movement performed; and is translatable to passing and defensive clearing. Overhead shooting (and slight variations of the shot) and related throwing motion are a common part of warm-up, drills, and scrimmage play. Players were provided a set of standardized instructions to naturally approach the target and release the ball with as much speed and accuracy as possible without compromising form for speed. Accuracy was defined as the ability of the ball to hit a simulated lacrosse goal target (1.82 × 1.82 m). The trial was excluded from analysis if the ball did not land in the goal target. The data from 3 trials were averaged to determine the typical shooting motion characteristics.
Specific kinematic events were expressed as a percentage of the shot cycle using available software (MATLAB; MathWorks Inc). Stride length was determined by the distance between the midfoot segment and the midfoot of the lead foot at foot contact; this value was then adjusted by height. The software was used to calculate angular velocities of the pelvis, trunk, and shoulder at key shot cycle events (lead foot contact [0%], ball release [100%], and follow-through [>100%]) and the relative orientation of the pelvis, trunk, and knee (sagittal); pelvis (sagittal and transverse); trunk (sagittal and frontal); and shoulder (transverse) joint angles at foot contact and ball release. There were 3 key phases of the lacrosse shot used for this analysis:
•Phase 1: Crank-back. In the wind-up phase, the shooting shoulder abducted and the trunk turned away from the target as the lead foot made contact with the ground in preparation for acceleration. Shoulder-to-pelvis motion involves the trailing shoulder crossing over the pelvis away from the target (back separation).
•Phase 2: Acceleration. This phase consists of increasing angular velocities of the body segments (pelvis, trunk, and upper arm about the shoulder) and crosse to prepare for the ball's release toward the target.
•Phase 3: Follow-through. In this phase, the shoulder crosses again over the pelvis (forward separation), and the body segments decelerate.
Concerning the determination of the kinematic variables, the maximum angular velocities of the pelvis, trunk, shoulders, and crosse were identified in the shot cycle. The joint excursions for the knee, pelvis, trunk, and shoulders in each of the 3 planes of motion were calculated as the difference between the maximum and minimum angular position values achieved from 0% to 100% of the shot cycle. The anterior and lateral lean of the trunk in the sagittal and frontal planes were determined from the difference in the maximum and minimum angular positions from 50% of the shot cycle to the end of the follow-through. The total rotation excursion of the pelvis-trunk was calculated from the summation of the absolute value of the crank-back and follow-through of the back and forward shoulder-to-pelvis separation angles.
Low Back Stress Index
We expanded what was known about combined trunk motion and trunk tilt angle in high-speed rotation motions such as those of a golf swing to better understand the risks of LBP in lacrosse players. 3 Using the previously published concept of the crunch index in golf as a guide (instantaneous product of lateral bending angle and trunk rotation velocity), we modeled our Low Back Stress Index score here to also include variables that represent the stresses that are applied to the lumbar region during a lacrosse shot. 21 The foundation for our index incorporated 2 distinct features of movement: (1) magnitude of maximum lateral trunk tilt and (2) maximum pelvic acceleration overall and at the time of maximum lateral trunk tilt. The Low Back Stress Index was calculated as follows:

Statistical Analysis
Descriptive statistics (means, standard deviations, and frequencies) were obtained to characterize the 3 study groups (no LBP, preexisting LBP, and developed LBP). The normality of the data was confirmed before analysis. To address our first study aim, univariate analyses of variance were used to determine whether differences existed between the 3 groups according to training volume and frequency, kinematic parameters (stride, joint angles, joint excursions, acceleration, angular velocities, relative time to achieve peak velocities, and Low Back Stress Index), and ball speed. Covariates included age, sex, and body mass index. Chi-square analyses were used to compare the frequency distribution for noncontinuous variables (sex, race, multisport athlete, youth or collegiate play level, seasons of play, position, and position change) between the 3 study groups.
To address our second aim, logistic regression models were developed to predict preexisting LBP and the development of LBP. Sex, age, and variables related to playing experience (field position [offense or defense], played other sports besides lacrosse [yes or no], and all-year lacrosse play [yes or no]) were entered into the models, and the comparator group was players with no LBP at any time during the study. Odds ratios (ORs) and 95% confidence intervals were obtained. A priori alpha levels were established at .05 for all statistical tests. IBM SPSS statistics software Version 26.0 (IBM Corp) was used for statistical analyses.
Results
Participant Characteristics
Of the 128 study participants, 102 had no LBP at any time point, 17 were found to have preexisting LBP, and 9 developed LBP during the 6-month follow-up. Table 1 summarizes the demographics and sport involvement characteristics of the participants overall and according to group. Participants with preexisting LBP at baseline were older than those with no LBP and who developed LBP (P = .019).
Baseline Characteristics of the Participants Overall and According to Study Group a
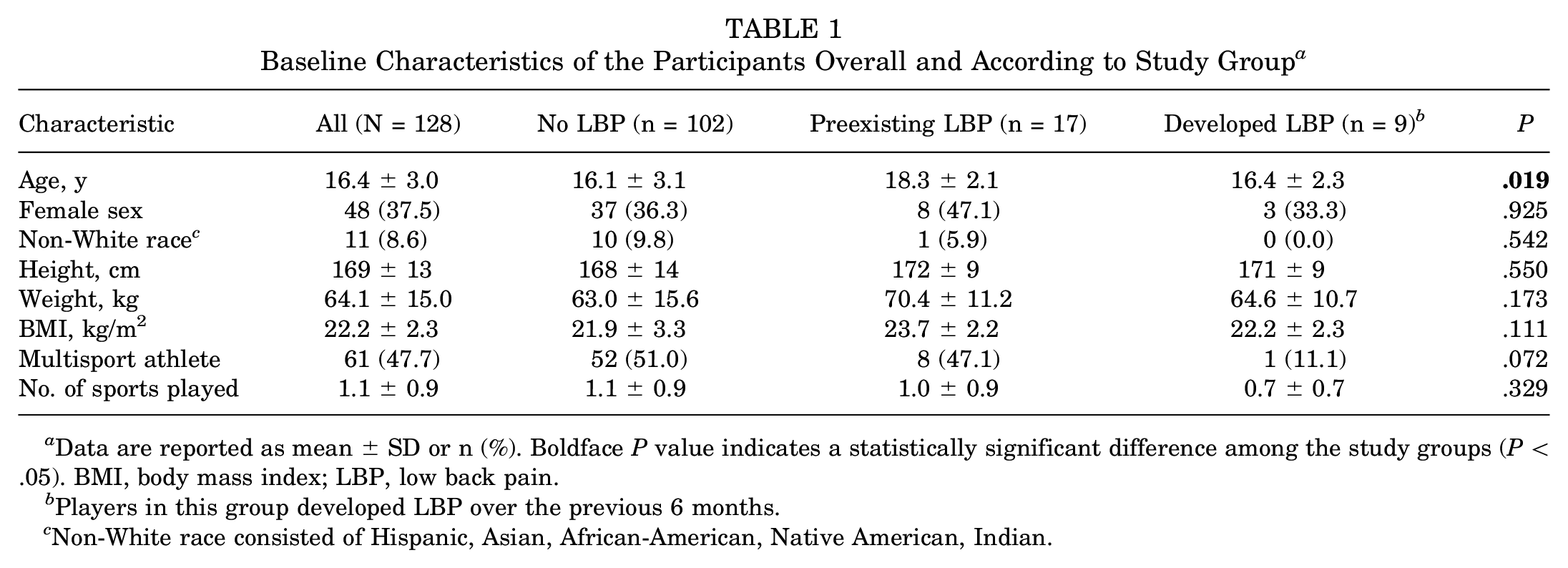
Data are reported as mean ± SD or n (%). Boldface P value indicates a statistically significant difference among the study groups (P < .05). BMI, body mass index; LBP, low back pain.
Players in this group developed LBP over the previous 6 months. c Non-White race consisted of Hispanic, Asian, African-American, Native American, Indian.
Playing Experience
Table 2 shows the playing experience of the participants. Overall, players participated for a mean of 6.3 ± 3.1 years and were currently engaging in between 3 and 5 lacrosse sessions per week. More than 93% of participants reported playing at least 2 seasons annually or all-year play. Midfield was the most commonly played position, and goalie was the least commonly played position. Fewer than one-fourth of the participants changed their position in the last year. No significant differences were found between the 3 study groups in years of lacrosse play, number of lacrosse sessions per week, or seasons played.
Lacrosse Playing Experience of the Participants Overall and According to Study Group a

Data are reported as mean ± SD or n (%). LBP, low back pain.
Biomechanics of the Lacrosse Shot
Key kinematics generated during the lacrosse shot motion are shown in Table 3. No differences were detected in stride length; shoulder-to-pelvis separation; or joint angles of the knee flexion, pelvic and trunk flexion anterior tilt, pelvic orientation toward the target, or shoulder abduction by ball release. However, several joint excursions differed among the groups. Participants with preexisting LBP and developed LBP produced more knee flexion excursion (P = .063). Players with preexisting LBP demonstrated less pelvis and shoulder rotation (alone and combined rotational motion) in the transverse plane than players with no LBP, whereas the players who developed LBP produced more rotation at the pelvis and shoulder (P < .05 for all).
Key Kinematic Variables During a Lacrosse Shot According to Study Group a

Data are reported as mean ± SD (95% CI). Boldface P values indicate a statistically significant difference among the study groups (P < .05). BR, ball release; FC, foot contact; LBP, low back pain.
Negative values denote lead shoulder motions away from the target.
Angular Velocities, Pelvic Acceleration, and Low Back Stress Index
Ball speed, maximum angular velocities and accelerations in the transverse plane, and temporal patterns of maximum segmental angular velocities are provided in Table 4. Maximum angular velocities for the pelvis, trunk, and shoulders were lowest in the preexisting LBP group and highest in the developed-LBP group (P < .05 for all). The developed-LBP group produced the highest maximum pelvic acceleration values overall and at the time point of maximum lateral trunk lean of all groups (P < .05 for both). Figure 2 shows the Low Back Stress Index scores. Despite different pelvic acceleration patterns by LBP group, the differences in mean Low Back Stress Index among the groups did not reach statistical significance (no LBP: 12,504 ± 13,076 deg2/s2; preexisting LBP: 8808 ± 10,174 deg2/s2; and developed LBP: 19,389 ± 13,590 deg2/s2; P = .157).
Ball Speed, Maximum Angular Velocities and Accelerations in the Transverse Plane, and Temporal Patterns of Maximum Segmental Angular Velocities a

Data are reported as mean ± SD (95% CI). Boldface P values indicate a statistically significant difference among the study groups (P < .05). LBP, low back pain; Max, maximum.
Expressed as a percentage of the lacrosse shot cycle, where 0% = lead foot contact with the ground and 100% = ball release.

Box-and-whisker plot of Low Back Stress Index values during a lacrosse shot among players with no low back pain (LBP), with preexisting LBP, and who developed LBP. The horizontal line represents the median, the x represents the mean, the top and bottom of the box represent the interquartile range, and the whiskers represent the range. Max, maximum; Min, minimum; Q1, quartile.
Results of Logistic Regression Analysis
Table 5 provides the ORs for preexisting LBP or development of LBP compared with no LBP at any time among the study participants. Older age increased the risk for preexisting LBP (OR, 1.32; 95% CI, 1.06-1.64; P = .012). For the development of LBP over 6 months, being a multisport athlete significantly reduced the risk (OR, 0.06; 95% CI, 0.006-0.56; P = .014), while playing lacrosse all year increased the risk by >7-fold (OR, 7.31; 95% CI, 1.44-37.2; P = .017).
Odds Ratios for Preexisting LBP and Developing LBP Among Lacrosse Players a

The comparator group was players with no LBP at any time during the study. Boldface P values indicate statistical significance (P < .05). LBP, low back pain; OR, odds ratio.
Discussion
The major findings from this investigation were that compared with the no-LBP group, (1) the preexisting LBP group demonstrated 13.9% to 22.9% lower maximum angular velocities at the pelvis, trunk, and shoulders in the transverse plane (P < .05); produced 19.3% lower collective pelvis-shoulder rotation in the transverse plane (P = .015); and produced 4.5% more knee flexion excursion (P = .063). The developed-LBP group produced 2.3% to 11.1% higher pelvis, trunk, and shoulder angular velocities (P < .05) and generated maximum pelvic acceleration values 36% to 42% higher than the remaining groups (P < .05). Mean Low Back Stress Index values were not statistically different among the groups (P = .157). Older players had a greater risk of preexisting LBP (OR, 1.32; P = .012), while year-round lacrosse play increased the risk for the development of back pain (OR, 7.31; P = .017). Playing other sports appeared protective against the onset of back pain during the follow-up (OR, 0.06; P = .014).
Based on previous work, 28 we hypothesized that players with preexisting LBP would have restricted pelvic and trunk rotational excursions with lower segmental angular velocities than those without LBP. This hypothesis was confirmed. In contrast to earlier work, ball velocity was not statistically different whether pain was present or not. Lacrosse players develop fast ball speeds by transferring energy along the kinetic chain from the lower body to ball release.17,30 It is likely that players with back pain use compensatory strategies distally in the kinetic chain to maintain high ball speed, such as more activation of the muscles in the arm, forearm, and hand to produce a wrist flexion snap motion. Our findings are in agreement with those of other studies showing deficits in pelvis transverse range of motion and pelvic angular velocity among the general population with LBP 22 and golfers with back pain. 6 Lastly, we hypothesized that players with greater peak pelvic rotational velocity and acceleration would develop LBP. This hypothesis can be partially supported as those participants who developed LBP during our study had 36% and 42% faster pelvic accelerations than those who did not have LBP and those who had preexisting LBP, respectively. In interpreting our findings, we recognize that as players mature, strength, shooting velocities, and forces acting on the body increase. The stresses may accumulate to contribute to pain, especially as lacrosse players specialize in the sport. Players with pain were older, and age was a risk factor for LBP. Among players who developed LBP, the high mechanical stresses related to shooting may have accumulated over the 6-month follow-up to contribute to new pain onset.
A unique aspect of this study was the calculation of a Low Back Stress Index. A previous research group developed a “crunch factor” for golfers 3 ; however, subsequent evidence has shown that this calculation has been largely inconclusive in detecting the impact of unilateral loading at the low back and lumbar spine during rotational sporting activity. 8 Our approach modified this published technique and considers the stress at the low back as an interaction of maximum lateral trunk tilt before ball release and pelvic acceleration at the time of maximum lateral trunk tilt. We suggest that this time point functionally represents one of the shot motion's highest rotational and shear stress aspects. The mean Low Back Stress Index scores among the groups did not reach statistical significance, likely given the considerable variance. Nevertheless, compared with the players with no LBP, mean scores were 55% greater in the developed-LBP group and 30% lower in the preexisting LBP group. In addition, the maximum acceleration of the pelvis as it rotated about the vertical axis was 36% faster in players who developed pain and 4% lower in players with preexisting pain. Acceleration has been previously shown to be a common mechanism of LBP, including disk herniations and soft tissue damage. 9 An important point to consider in lacrosse is the variation in a shooting motion during actual game play, which could potentially increase the stress on the low back as players maneuver around other players for a shot or shoot from far distances. Players may adopt a more lateral lean when shooting sidearm or underhand, depending on the situation and player style. Although we did not directly capture this as part of this study, there is the possibility that players with a history of LBP habitually use more lateral bending on the field with normal shooting volume, which can potentially affect the stresses at the low back and back pain symptoms. Additional field research in both game and practice situations and comparison of the effects of shooting variations on LBP are needed to systematically address this question of habitual shooting style on symptoms and motion.
We initially hypothesized that field positions that commonly shoot high volumes during play (midfield or attack) would have higher odds of reporting and developing LBP than positions that shoot less (e.g. defense, long stick midfield, or goalie). We were unable to support this hypothesis. Second, we predicted that players currently participating in sports additional to lacrosse throughout the year would have a lower prevalence of LBP and LBP development than players participating only in lacrosse. Participants who only played lacrosse had a nearly 7-fold increase in odds of developing LBP. These findings emphasize the need to encourage lacrosse athletes to participate in various activities involving different movement patterns and skill sets and training strategies that improve dynamic stability and core rotational strength.
Limitations
The limitations of this study deserve comment. Although we followed lacrosse athletes prospectively, functional and kinematic measures were only collected at baseline. Moreover, a larger sample size of lacrosse players who developed LBP during follow-up would have improved study power and understanding of risk factors that may predispose lacrosse athletes to develop LBP. While the literature notes a high prevalence of LBP in athletes within the age range of our sample, onset of LBP over a 6-month period in this select group of athletes would not realistically mirror prevalence among larger cohorts.
In addition, there are differences in shot motions between male and female lacrosse players because of equipment design and game strategy. The crosse used by female lacrosse players has a shallow pocket to cradle the lacrosse ball, potentially forcing them to restrict their shot motions to prevent them from losing possession of the ball. 7 Moreover, because of rule restrictions and the helmets and protective pads used by female players, contact injuries are significantly reduced. The combination of male and female players in our analysis may have skewed our overall results, as injuries are sustained at different rates 15 and shots are performed at different velocities 31 according to sex. Although the prevalence of LBP in lacrosse players was not different between sexes, we still accounted for sex in our analyses.
Considerations for volume of lacrosse could be further investigated. Although we assessed years of lacrosse play and lacrosse sessions per week, we did not track weekly changes in lacrosse play (such as rapid ramping spikes in volume relative to the testing time point or tournament events). Accumulations of volume spikes are related to back pain onset in high-speed rotational sports. 14 Moreover, we did not include measures of ground-reaction forces produced by the lead foot, which could have provided additional compression forces to the shearing and rotational forces at the lumbar spine. Given our sample of varied ages, positions, and skill levels, the results have generalizability to the broader lacrosse population. Finally, we acknowledge that our Low Back Stress Index has not been validated or tested in isolation. While based on previous calculations in the golf population, we have not independently verified its value, and the purpose of its use in this paper is purely as an indicating variable. Future efforts should aim to test this index (1) on a population with relatively little performance variability (ie, established/elite players or growing/learning adolescent players but potentially not combined), (2) in specialized lacrosse athletes without other sport motion confounders, (3) in conjunction with shooting volume tracking, and (4) over longer periods of time as back symptoms and pain severity change.
Future Directions
Further research should aim to determine wrist, elbow, and shoulder kinematics in lacrosse players, as the utilization of these segments could explain areas where players might compensate for LBP or they may further influence LBP. Comparison of the effects of different shooting types (sidearm, overhead, and underhand) on LBP and back stress and documented volume of shots taken during weekly play is needed to support the proposed relationship studied here. Lastly, the next step is to focus on events and motions during the follow-through. A large portion of low back injuries in lacrosse have a muscle-tendon strain mechanism 5 ; this may relate to eccentric forces during the follow-through phase. In other overhead sports like pitching, the follow-through is the second most stressful phase of a throw because of its eccentric demand on the body. 1 Advancements in sports medicine may be next achieved through implementation of injury prevention programs and/or potential addition to exercise programs provided by USA Lacrosse online for the lacrosse community. Incorporation of dynamic strengthening, core stabilization, and endurance may help to mitigate the onset of back pain as players develop.
Conclusion
The study findings indicated that lacrosse players with existing LBP have slower peak pelvic, trunk, and shoulder angular velocities and greater knee flexion during a shot motion than players with no pain. Higher pelvic acceleration was a distinguishable risk factor in players who developed LBP. Lack of multisport participation contributed to the onset of LBP in lacrosse athletes. With further age stratification and analysis, data will likely reveal subgroups of players who may benefit from training and injury prevention programs. Those players who develop pain may consider improving strength and dynamic stability about the core, hips, upper back, and lower body to improve durability against LBP.
Footnotes
Final revision submitted August 29, 2023; accepted September 6, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research was received from a USA Lacrosse Sports Science and Safety Grant (PRO00008322) and the University of Florida Clinical and Translational Science Institute, which is supported in part by the National Institutes of Health (NIH) National Center for Advancing Translational Sciences under award No. UL1TR001427. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Florida (reference No. 94-2013 and IRB201602059).