
Abstract
Background:
There has been little focus on concussions in youth lacrosse players in the United States.
Purpose:
To provide a descriptive analysis of the epidemiology and incidence of concussions in youth lacrosse and compare the results with well-documented analyses of concussions in youth American football.
Study Design:
Descriptive epidemiology study.
Methods:
Data on concussions in pediatric patients playing lacrosse from 2006 to 2019 were collected using the National Electronic Injury Surveillance System (NEISS). Weighted calculations and combined participation data obtained from membership in USA Lacrosse were used to estimate injury incidence. A comparison dataset was created using the NEISS data on youth football-related concussions. The cause of concussion was categorized into player-to-player, player-to-stick, player-to-ball, or player-to-ground contact.
Results:
A total of 37,974 concussion injuries related to lacrosse were identified in players with a mean age of 14.5 ± 3.5 years; 70% of concussions occurred in boys. National participation in lacrosse increased from 2006 to 2011 by a mean of 10.3% annually, followed by a lower annual growth rate of 2.5% from 2012 to 2019. The overall incidence of concussion injuries increased over the study period (r = 0.314), with the incidence rate in boys being greater than that of girls from 2009 to 2013. The most common cause of concussion was player-to-ground contact for boys and player-to-ball or player-to-stick contact for girls. The mean annual concussion incidences in youth lacrosse and youth football were 443 and 355 per 100,000 participants, respectively.
Conclusion:
Over the study period, 16% of lacrosse injuries were diagnosed as concussions, a higher mean annual incidence per 100,000 participants than that of youth football (443 vs 355). The cause of concussion was different based on sex, with higher rates of player-to-ball or player-to-stick contact in female players versus player-to-ground contact in male players.
Keywords
Recent studies suggest that an estimated 38 million children and adolescents are involved in organized sports, and 1.1 to 1.9 million sport-related concussions occur in children in the United States (US) each year. 12 In a study by Diamond and Gale, 6 it was noted that children between the ages of 4 and 11 years experienced the highest percentage of head and face injuries. Given the long-term impact and implications of concussions, there is now increased media attention on this in the youth sports population.21,24
Although these concussion rates are well established for football, limited evidence exists for youth lacrosse, which is considered one of the fastest-growing sports among this population in the US.3,8,11,14,19 A recent report 27 found that 180,399 high school boys and 292,695 youth boys <14 years old played lacrosse in 2016. As for girls, lacrosse has been noted to be the fastest-growing team sport in the US, with participation rising from 64,929 participants in 2008-2009 to 99,750 participants in 2018-2019. 25 Given the increasing popularity and participation in lacrosse among the youth population, better awareness regarding the incidence of head and face injuries in youth players is needed.4,11 This is especially important when considering that injuries to the head and face of lacrosse participants are significantly more prevalent among women than men across all age ranges, partly due to less protective equipment in these same cohorts. 5
Previous studies have examined concussion rates in college lacrosse players using the National Collegiate Athletic Association (NCAA) Injury Surveillance System. In a study by Covassin et al, 5 both male and female lacrosse players were listed as at the highest risk among the collegiate athletes for sustaining a concussion without significant sex differences. Although there are established rates at the collegiate level, limited research has been done on the rates for youth lacrosse or sex differences in the sport, especially given the rules differ by sex in youth lacrosse.5,28 Understanding current epidemiology and differences in rates of concussion for boys and girls might help better guide regulations and prevention programs at the youth level.
The primary aim of this study was to determine the concussion rates in the pediatric lacrosse population and the common causes of concussions at this level. The secondary aim was to understand differences in concussion rates based on sex and compare them with those of youth football, which is a more well-established sport.
Methods
Ethics committee approval was not required for this study. The National Electronic Injury Surveillance System (NEISS) was used to gather data on lacrosse and football injuries reported from 2006 to 2019 for athletes <19 years old. The NEISS is composed of annual samples collected by the US Consumer Product Safety Commission (CPSC) from 100 hospitals selected as a probability sample of all (≥5000) hospitals with emergency departments across the US. Data were updated daily, and missing patient data were collected via telephone interviews. Incidents involving consumer products were reported in emergency departments. Patient information is recorded in the database for every visit to an emergency department involving a consumer product, such as sports equipment. Data are continuously reviewed and updated via telephone calls with patients within 1 week of reporting their injury. From this sample, national rates of injuries can be estimated. The sampling procedure and statistical basis for determining national estimates using the NEISS data are validated approaches and are described in depth on the CPSC website.22,26 These approaches are meant to refresh the hospital sample while maintaining the core sampling plan. To minimize statistical variance and ensure sufficient geographical representation, the sampling frame—a list of hospitals that meet the required criteria—has been organized based on hospital size and arranged by geographic location. This methodology attempts to minimize biases for regional variations and provide accurate national estimates. In addition, the derivation of sampling weights used by the NEISS is well established and used by researchers and government agencies. 2 After being weighted, the NEISS data provide estimates for the total number of injuries related to each consumer product that is included. Variables that are recorded include treatment date, sex, race, diagnostic category, injured body part, patient disposition, and location of injury.
Using the NEISS diagnosis code for concussion (52), cases in the dataset were filtered to identify all concussions relating to lacrosse and football and further stratified for lacrosse according to age and sex. The cause of concussion was categorized as player-to-player, player-to-ball, player-to-stick, or player-to-ground contact. When added, the sampling weighted values provided by the CPSC allowed for comparing the national prevalence of concussions in lacrosse and football.
Participation rates were collected to calculate the incidence rate for concussions on a per-athlete basis. Lacrosse participation numbers were obtained from the USA Lacrosse Annual Participation Report, which includes data provided by USA Lacrosse membership records, the NCAA, the National Federation of State High School Associations (NFSHSA), and fanlax. com.27,29 Concussions that occurred while playing lacrosse were identified to ensure the accuracy of the type of injury occurring from direct participation in organized lacrosse. Narratives were reviewed for each injury, and the mechanism of injury was recorded. In addition, the number of concussions was collected for football as a comparison using the NEISS product codes for football (activity, apparel, or equipment). Participation rates for tackle football were gathered from the Outdoor Foundation Participation Reports, which have also been cited in other studies in the sports literature.7,18,23 The Outdoor Foundation is a nonprofit organization dedicated to encouraging and enhancing the experiences of people in the outdoors. Annually, the organization conducts online surveys and interviews to assess participation in various outdoor sports. The report generated from this includes a section on football participation in those aged ≥6 years (Football 6+), which is further stratified by flag, touch, and tackle football. The statistics generated from this report are gathered from the Physical Activity Council, a partnership of leading organizations in the US sports and fitness industries, with one of those partners being USA Football. 18 Similar to the NEISS database, a weighting technique was used to balance the data on participation rates for tackle football.
Statistical Analysis
Linear regression analyses were used to assess the statistical significance of observed trends. The Spearman correlation coefficient was used to assess the relationship between the total number of concussions and the incidence of concussions for both boys and girls in lacrosse over the study period. A subanalysis was conducted using the Spearman correlation coefficient to compare the incidence of concussions in lacrosse and football over the study period. All analyses were performed using SPSS software (Version 29; IBM Corp). For this study, P < .05 was considered statistically significant. Reported values were rounded to the next highest integer to eliminate the reporting of fractional concussion cases.
Results
A weighted total of 37,974 concussions in lacrosse were reported from the NEISS database during the 13-year study period (2006-2019). The total national estimates of lacrosse-related injuries over the study period were 235,187, with 16% (n = 37,974) of those injuries diagnosed as concussions. When stratified by sex over the study period, boys had a total of 181,379 lacrosse-related injuries, while girls had 53,808 lacrosse-related injuries. Of the injuries diagnosed as a concussion, boys had 26,425 (15%) concussions, while girls had 11,549 (22%) concussions. The mean age of the cohort was 14.5 ± 3.5 years. A mean of 1887 concussions occurred in male players each year, and a mean of 825 concussions occurred in female players each year during the study period (Table 1).
Lacrosse Injuries and Concussions in Youth Players, 2006-2019

National participation in lacrosse steadily increased from 2006 to 2011 by a mean of 10.3% annually and then experienced a lower annual growth rate of 2.5% from 2012 to 2019 (Table 2, Figure 1). The number of concussions in lacrosse each year was found to increase over the study period (r = 0.314) (Figure 2), and the percentage of concussions compared with all injuries in lacrosse ranged between 10% and 20%.
Participation and Growth Rate in Lacrosse, 2006-2019


Yearly youth lacrosse participation and growth rate, 2006-2019.

Total concussions in youth lacrosse, 2006-2019 (r = 0.314).
The incidence of concussion injuries in lacrosse had a weighted mean of 443, and there was a significant increase in concussion incidence per 100,000 lacrosse players from year to year until 2013. However, the weighted incidence of concussions dramatically decreased after 2013. Of note, there was a drastically greater incidence rate of concussions in lacrosse for boys from 2009 to 2013, but this became comparable to girls by 2019 (Table 3, Figure 3).
Prevalence of Concussion in Lacrosse, 2006-2019

Per 100,000 male and female players.
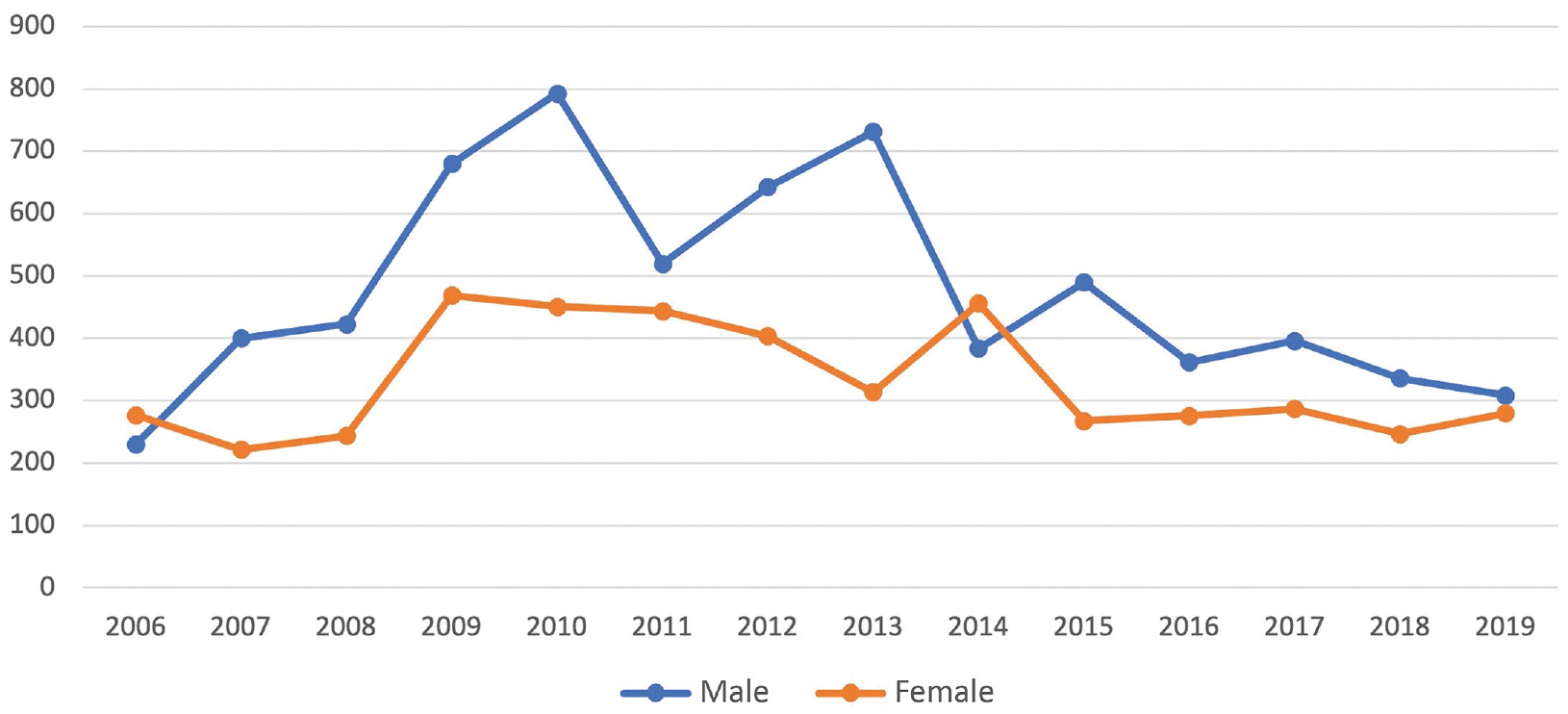
Incidence of concussions in lacrosse per 100,000 players by sex, 2006-2019.
A review of narratives related to each concussion injury found that 36% (n = 323) of concussions were caused by player-to-ground contact, followed by player-to-stick contact (29%, n = 262), and subsequently 23% (n = 205) were caused by player-to ball-contact and 13% (n = 115) by player-to-player contact (Figure 4).

Type of contact causing concussions in lacrosse.
When reviewing the types of contact that resulted in concussions for girls, we identified that the most common was player-to-ball at 37%, closely followed by player-to-stick at 36%, with the least common being player-to-player at 10%. For boys, the highest incidence was player-to-ground contact (45%), followed by player-to-stick (26%) then player-to-ball and player-to-player, which were nearly identical at 15% and 14%, respectively (Figure 5).

Contact type by concussion incidence according to sex.
When comparing youth lacrosse to youth football, both sports showed an increase in the incidence of weighted concussions per 100,000 players, with the mean being greater for lacrosse than football over the study period (443 vs 355). Interestingly, from 2006 to 2013, youth lacrosse had a greater incidence of concussions than football (477 vs 311) but was found to be lower from 2014 to 2019 (350 vs 414) (Figure 6).

Incidence of concussions in youth lacrosse vs football 6+, per 100,000 participants, 2006-2019.
Discussion
Our results demonstrated that the incidence of concussions was 4 per 1,000 participants, with concussions representing 16% of the injuries that were presented to the emergency department in youth lacrosse. Our results appear to be consistent with previous reports on concussion rates for boys (15%) and girls (22%), with a range reported from 5.8% to 23.1% for boys and 1.69% to 25.6% for girls; also, our study appears to be more on the higher end of this range, as we found rates of 15% for boys and 22% for girls.10,13,30 In addition, we found that the annual lacrosse-related concussion incidence per 100,000 participants initially increased from 2006 (n = 247) to 2013 (n = 576) but then declined over the remainder of the study period (n = 298 in 2019). These results may be impacted by an overall decline in participation from 2013, or these declines may also be due to rule changes implemented by the NFSHSA to reduce head and neck injuries. 9 Specifically, these revisions were made to rules regarding body checking during game play but also may have helped contribute to the decreased concussion incidence from 2013. Perhaps as more lacrosse rule changes are made for this population of athletes, the concussion rate, in particular, will continue to reduce. 1
The most common cause of concussions associated with youth lacrosse was found to be because of players hitting the ground or contact with another player's stick. Specifically for boys, player-to-ground contact was the most common cause, which could largely be attributed to player-to-player contact, while for girls, player-to-ball followed by player-to-stick contact was the most common. Other researchers also demonstrated that the most common mechanism of injury for boys was contact with a stick, while for girls, it was overuse as well as contact with a stick. 30 In addition, the findings of O’Connor et al 17 were consistent as well, indicating that the most common cause of concussions for female high school lacrosse players was ball contact and the most common cause of concussion for boys was player-to-player contact. It is important for us to identify the major causes of concussions in lacrosse for each sex, as boys and girls have differences in rules, protective equipment, and level of contact permitted during games. The only required gear for female lacrosse players is protective eyewear and mouthguards. Moreover, it was only in the spring of 2017 that female lacrosse players were allowed to wear helmets during lacrosse games at their discretion, while male players were required to wear certified helmets in addition to the gear worn by female players. 28 According to USA Lacrosse, the national governing body of lacrosse, helmet use for female field players is unnecessary since head and body contact is illegal. However, our data found that the most common cause of injury in our study was player-to-stick and player-to-ball contact, highlighting that these athletes may still be at risk of major head injuries and that appropriate protective equipment may be necessary . 28 A study by Comstock et al 4 further supports this argument that 44.7% of all concussions for female youth lacrosse players could have been prevented if girls were also required to wear the same certified helmet and face shield as boys.
Furthermore, youth lacrosse and youth football were compared to evaluate the incidence of concussions in a youth sport population and also as a result of a large multihigh school and collegiate study that found women's and men's lacrosse ranked second and third only to American football in the incidence rate of concussions. 15 Pierpoint and Collins 20 reported that concussion rates per 10,000 athlete-exposures (AEs) for high school male lacrosse players were lower than concussion rates among high school football players (4.87 vs 7.28). For women, there was no comparison for football, but they did report a concussion rate of 3.67 per 10,000 AEs for high school lacrosse players. In our study, we found a higher mean incidence of concussions for youth lacrosse compared with youth football until 2014. However, after 2014, this became comparable until the end of the study period. A possible explanation of this higher rate may be due to the “targeting rule” (Rule 2-43) that was implemented by the NFSHSA in 2014 for football, in addition to improved detection rate and officiating. In a study by Obana et al, 16 before implementing the targeting rule, the rate of concussions diagnosed in US emergency departments rose by 10.7% between 2009 and 2013, and there was a 6.2% decrease between 2015 and 2019 (P = .04) after implementing the targeting rule in 2014. As a result of these findings, future studies should focus on increased prevention efforts and education for concussions in lacrosse in a similar way to what has occurred in football over recent years. 1 Overall, these results bring to light the need for increased awareness of rule discrepancies between sexes as well as the need for increased prevention efforts and education for concussions in lacrosse, in a similar way to what has occurred in football over recent years. In addition, to better identify risks that should be mitigated, future studies should prospectively analyze concussions in lacrosse within this population.
Limitations
Although this study brought new insight into the importance of concussions in the pediatric population, it is not without limitations. Many written narratives in the NEISS database for lacrosse did not document the type of contact that resulted in the patient's concussion. The database is also limited in that it only records emergency department visits and may exclude less severe concussions in patients who did not present in a hospital setting, thereby underreporting the actual concussion injury rate in this youth population. Also, the NEISS database relies on self-reporting by patients and health care providers and does not include information on race or socioeconomic status, thus limiting our ability to identify disparities in injury rates. In addition, participation and concussion data for flag and tackle football were limited, as these sports are frequently played without formal organizations, and the concussion rates likely go unreported as a result. 18
Conclusion
Lacrosse has quickly gained popularity among young American athletes over the past 2 decades. Compared with youth football, lacrosse had a higher mean yearly incidence of concussions per 100,000 players (16%), which is significant (443 vs 355). The cause of concussion appears to be different based on sex, with higher rates of player-to-ball or player-to-stick contact in female youth lacrosse athletes compared with the player-to-ground contact in male players.
Footnotes
Final revision submitted June 28, 2023; accepted July 31, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: V.S. has received research support from Orthofix and Wright Medical Technology; education payments from Arthrex and Southern Edge Orthopaedics; consulting fees from Stryker, Wright Medical Technology, Zimmer Biomet Holdings, Arthrex, and Restor3D; nonconsulting fees from Exactech; honoraria from Encore Medical; and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.