
Abstract
Background:
Soft tissue swelling in shoulder arthroscopy is common and may lead to complications. Measures aimed at reducing this phenomenon are routinely used with limited efficacy.
Purpose/Hypothesis:
The purpose of the study was to assess (1) soft tissue swelling of the shoulder (the operated site) and (2) soft tissue swelling of the neck, chest, and arm (the surrounding tissue) in patients with versus without compressive draping during shoulder arthroscopy. It was hypothesized that compressive draping of the shoulder with adhesive incise drape would reduce soft tissue swelling during shoulder arthroscopy.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 50 patients undergoing arthroscopic rotator cuff repair were prospectively randomized to either the study group (in which the shoulder was draped with adhesive incise drape tightened around the shoulder) or the control group (in which a standard shoulder arthroscopy drape was used). The circumferences of the shoulder, arm, chest, and neck were measured preoperatively and postoperatively and compared between the groups.
Results:
The shoulder circumference in the standard draping group increased by 16% during the procedure (from 21.2 ± 1.5 cm preoperatively to 24.5 ± 1.7 cm postoperatively) compared with only 6% in the compressive draping group (from 21.0 ± 1.3 cm preoperatively to 22.3 ± 1.1 cm postoperatively) (P < .01). No serious postoperative complications were observed in either group.
Conclusion:
Compressive shoulder draping with adhesive incise drape was effective in reducing soft tissue swelling around the shoulder in arthroscopic rotator cuff repair compared with standard arthroscopic draping and was not associated with any adverse reactions.
Registration:
NCT03216590 (ClinicalTrials.gov identifier).
Keywords
Fluid extravasation into the surrounding tissue is common in shoulder arthroscopy. It frequently leads to soft tissue swelling and edema, which result in poor visualization and prolonged surgical duration.3,12 While it usually resolves uneventfully within 12 hours, excessive fluid extravasation into the soft tissue around the shoulder has been reported to potentially lead to serious consequences and complications, such as airway compromise, tracheal deviation, neuropraxia, rhabdomyolysis, and skin necrosis.2,4,9,13 Measures aimed at reducing soft tissue swelling during shoulder arthroscopy to avoid complications (eg, low pump pressure and short arthroscopic time) are routinely practiced.8,10,14 Because of the limited efficacy of those methods, fluid extravasation and soft tissue swelling remain a concern in shoulder arthroscopy.
The primary objective of this study was to compare soft tissue swelling of the shoulder (the operated site) during shoulder arthroscopy in patients with and without compressive draping. The secondary objective was to compare soft tissue swelling of the neck, chest, and arm (the surrounding tissue) between these patients. We hypothesized that applying local intraoperative compression to the shoulder, by shoulder draping with adhesive incise drape, would reduce soft tissue swelling during shoulder arthroscopy.
Methods
Study Design and Setting
This was a prospective, randomized, single-blinded trial. Participants were recruited from among the patients who underwent shoulder arthroscopy in our shoulder surgery unit between July 2017 and June 2018. The study was designed in accordance with the International Conference on Harmonization Guidelines for good clinical practice, and the study protocol was approved by our institutional ethics committee.
Patient Selection
The clinical decision regarding surgical intervention was made by 1 of 2 senior shoulder surgeons (O.U. and G.L.) based on clinical evaluation and relevant imaging tests. Criteria for inclusion in the study were (1) symptomatic rotator cuff tear with no clinical improvement after a nonoperative treatment for at least 3 to 6 months, (2) superior rotator cuff tears <3 cm (which represents the majority of our patients), (3) age >18 years, (4) American Society of Anesthesiologists class 1 or 2, (5) body mass index (BMI) between 18 and 35 kg/m2, and (6) informed consent given. Criteria for exclusion from the study were (1) pregnancy, (2) conversion from arthroscopy to an open procedure, and (3) noncompliance with the inclusion criteria as described above.
Because arthroscopic procedures in the subacromial space (in the absence of a rigid articular capsule) involve more soft tissue edema than isolated procedures in the glenohumeral joint,1,4 we chose to exclude isolated arthroscopic labrum repairs (performed in the glenohumeral cavity) and to include only arthroscopic rotator cuff repairs (involving the subacromial space). To avoid a bias related to different tear sizes between the groups and because the majority of rotator cuff repairs performed in our clinic are of small- and medium-sized tears, we preferred to include only patients with tear sizes up to 3 cm. Patients with a BMI >35 kg/m2 were excluded from the study, in view of the risk of prolonged hospitalization and the increased tendency for soft tissue edema during surgery in obese patients.5,6
Study Protocol
Patients who were eligible for study inclusion were randomized to either the control group or the study group by opening a pre-prepared sealed envelope (made by a independent secretary from the orthopaedic ward), with the same probability of allocation to each group. A total of 54 patients were randomized; of these patients, 50 (25 patients in each group) were included in the data analysis (Figure 1).
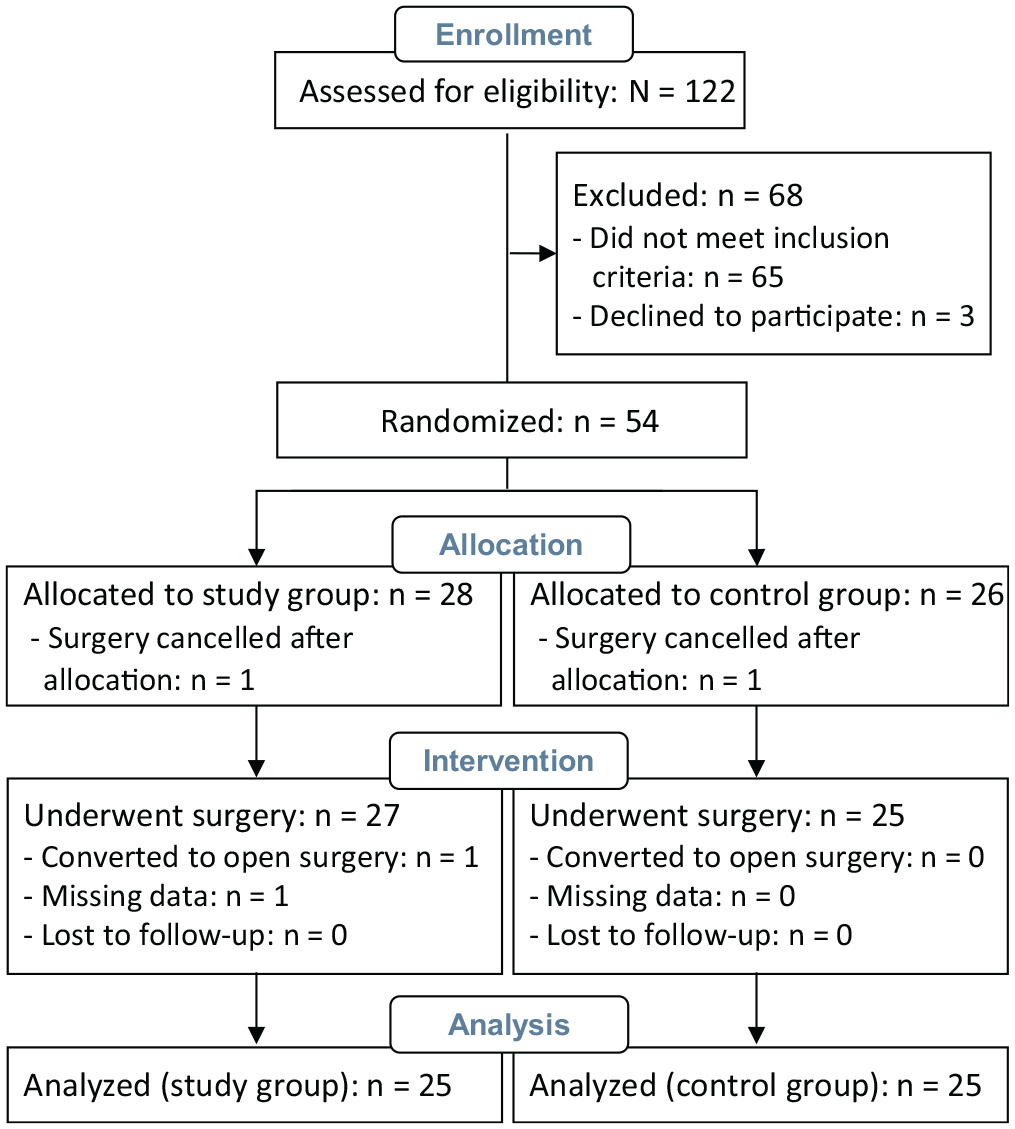
Flow diagram of patient enrollment.
For sterile draping in the control group, we used a standard arthroscopic shoulder drape with the shoulder exposed (Figure 2A). Sterile draping in the study group was done using a similar standard shoulder drape plus compressive draping around the shoulder with an adhesive incise drape (Ioban 2 Antimicrobial Incise Drape; 3M Inc) applied by the first author (O.U.) (Figure 2B).
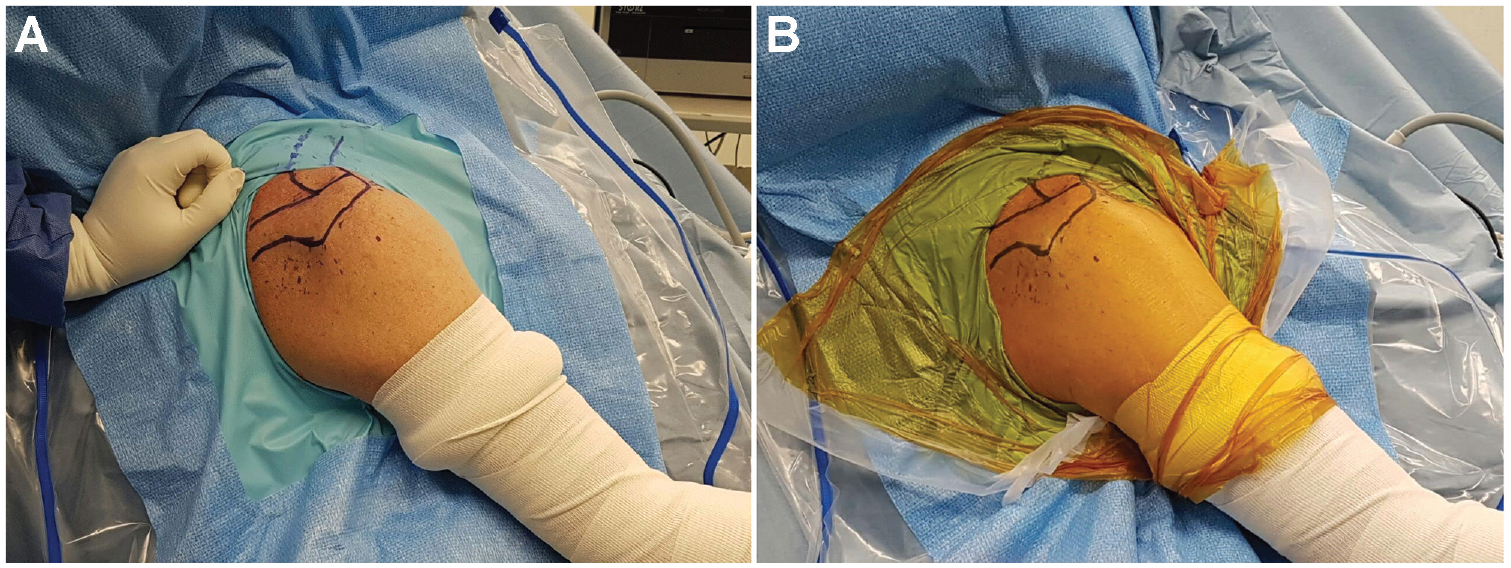
Sterile draping for patients in the (A) control group and (B) study group.
All arthroscopic surgeries were performed by 1 of 2 senior shoulder surgeons (O.U. and G.L.) under similar conditions and in a similar method, including (1) preoperative prophylactic antibiotics, (2) ultrasound-guided interscalene brachial plexus nerve block, (3) beach-chair positioning with a dedicated arm holder (Spider2; Smith & Nephew), (4) elastic bandage around the arm to the axilla level, (5) irrigation with normal saline in 3-L bags with 1 mg epinephrine, (6) a specially designed arthroscopic pump (FMS DUO + Fluid Management System; DePuy Synthes) at a constant pressure of 50 mm Hg, (7) hypotensive anesthesia with systolic blood pressure ranging from 90 to 100 mm Hg, (8) use of conventional arthroscopic portals (posterior, anterior, lateral, and anterolateral as needed) without the use of cannulas, (9) subacromial decompression including acromioplasty in all cases and repair of the tears by suture anchors, and (10) 24-hour in-hospital stay after surgery. All patients remained blinded until their discharge.
Outcome Measures
The following measurements were taken preoperatively and postoperatively by the first author (O.U.) with the patient in the beach-chair position: (1) shoulder circumference from the midpoint between the coracoid process and the anterior axillary fold anteriorly to the midpoint between the posterior axillary fold and the scapular spine posteriorly, (2) arm circumference at midarm level, (3) neck circumference, and (4) hemichest circumference from the midsternal line through the axilla to the medial scapular border at the back of the thorax (Figure 3).
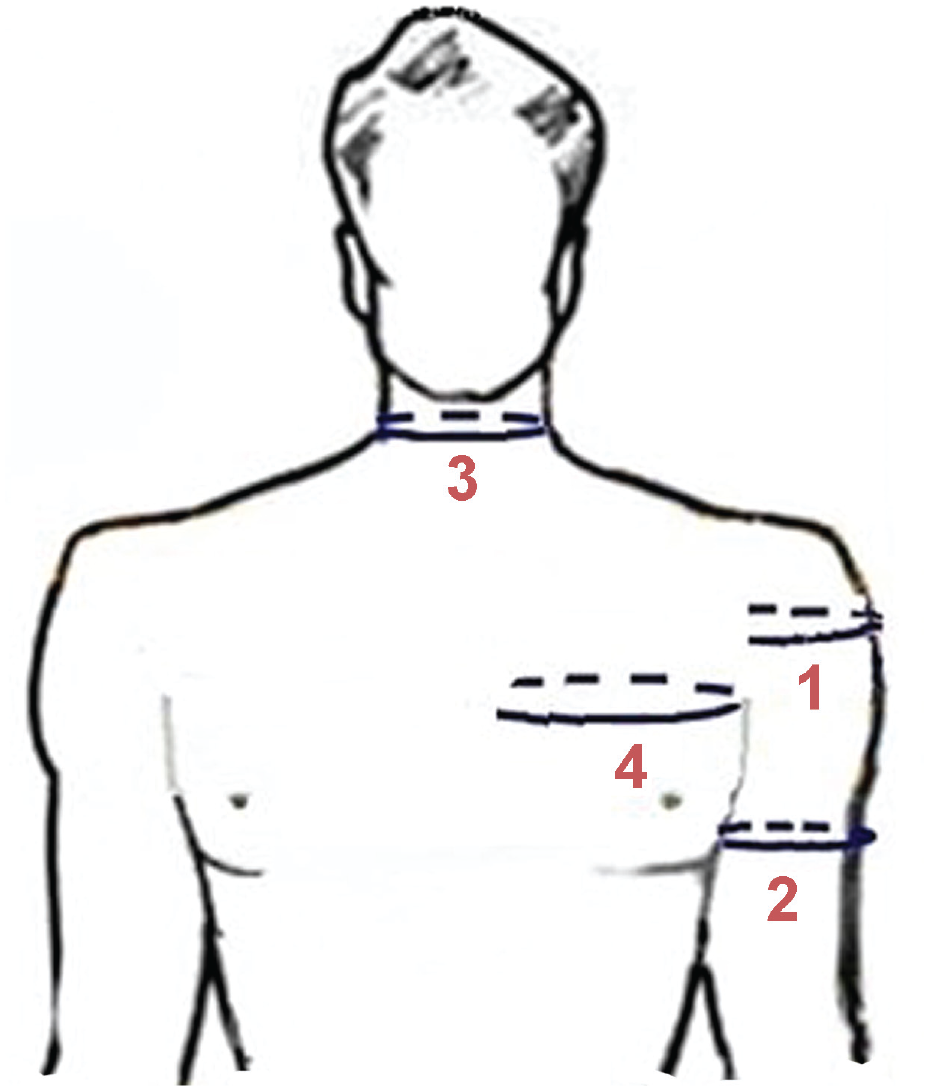
Circumference measurements. (1) Shoulder circumference from the midpoint between the coracoid process and the anterior axillary fold anteriorly to the midpoint between the posterior axillary fold and the scapular spine posteriorly. (2) Arm circumference at midarm level. (3) Neck circumference. (4) Hemichest circumference from the midsternal line through the axilla to the medial scapular border at the back of the thorax.
Soft tissue “swelling” at the end of the arthroscopic procedure was defined as the postoperative increase in the shoulder and surrounding tissue circumference relative to the preoperative measurement (percentage) according to the following equation: Circumference increase (%) = [(Postoperative circumference – Preoperative circumference)/Preoperative circumference] × 100.
In addition, the following data were recorded: (1) duration of surgery (minutes); (2) volume of the irrigation used (liters); (3) appearance of edema in a manner that caused prominent unilateral asymmetry in the deltoid, scapular region, trapezius, pectoralis, and neck; (4) surgical complications (eg, respiratory, neurological, and vascular complications), evaluated at the end of the surgery and before discharge from the hospital; and (5) delayed complications (eg, neurapraxia, deep venous thrombosis, wound complications, and infection), evaluated at the 2-week postoperative outpatient visit.
Statistical Analysis
Patient and clinical parameters (age, BMI, surgery duration, volume of irrigation, and swelling measurements) are presented as mean ± standard deviation (SD) and were compared between the groups using the unpaired 2-tailed t test. Categorical parameters (patient sex and rate of apparent swelling within each group) are presented as proportions and were compared between the groups using the Fisher exact test. Data analysis was performed using MedCalc Statistical Software Version 19.7.2 (MedCalc Software Ltd). With the alpha level set at .05, we determined prospectively (based on preliminary pilot results) that 22 patients per group would give 90% power to identify a 5% difference in shoulder swelling between the groups.
Results
The mean age was 57 ± 9 years (range, 42-73 years), and the mean BMI was 25 ± 4 kg/m2 (range, 19-32 kg/m2). The surgical duration was a mean of 61 ± 14 minutes (range, 45-100 minutes), and the amount of irrigation fluid used was 9 ± 4 L (range, 7-15 L). All parameters were similar for both groups (Table 1).
Patient and Clinical Data of the Study Groups a
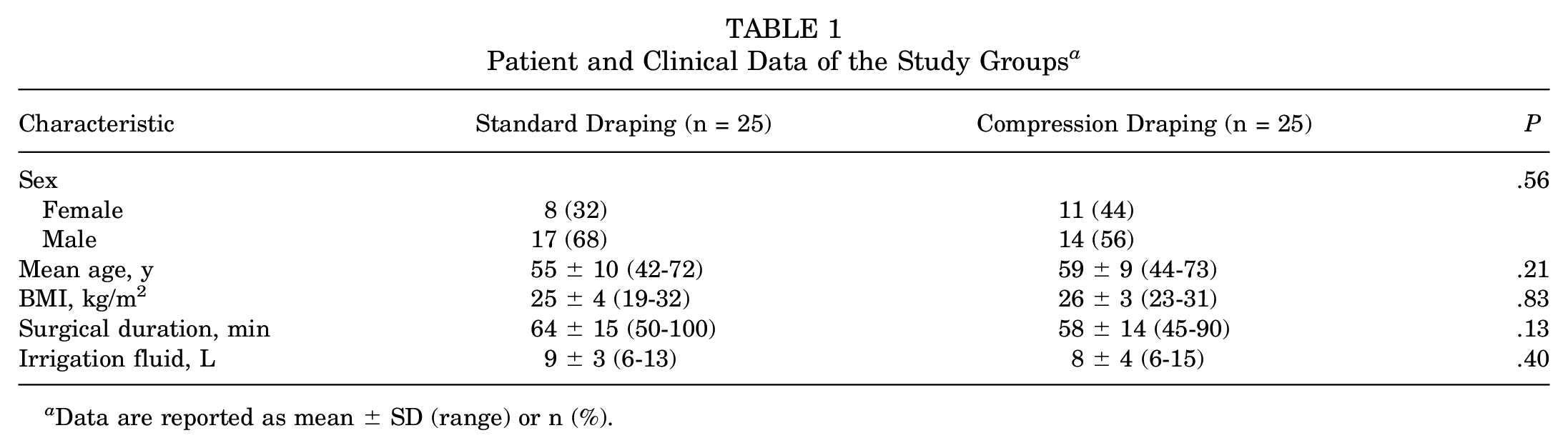
Data are reported as mean ± SD (range) or n (%).
The shoulder circumference increased in the standard draping group from a preoperative mean of 21.2 ± 1.5 cm (range, 19-24 cm) to a postoperative mean of 24.5 ± 1.7 cm (range, 21-27 cm) (a mean circumference increase of 16% ± 3%) and in the compression draping group from a preoperative mean of 21.0 ± 1.3 cm (range, 19-23 cm) to a postoperative mean of 22.3 ± 1.1 cm (range, 21-24 cm) (a mean circumference increase of 6% ± 2%). The difference between the groups was statistically significant (P = .001), representing significantly less soft tissue swelling at the end of the surgery in the compression draping group. The midarm circumference, neck circumference, and hemichest circumference increased postoperatively to a similar extent in the standard draping and compression draping groups, with no significant between-group differences (Table 2).
Comparison of Outcomes Between the Study Groups a
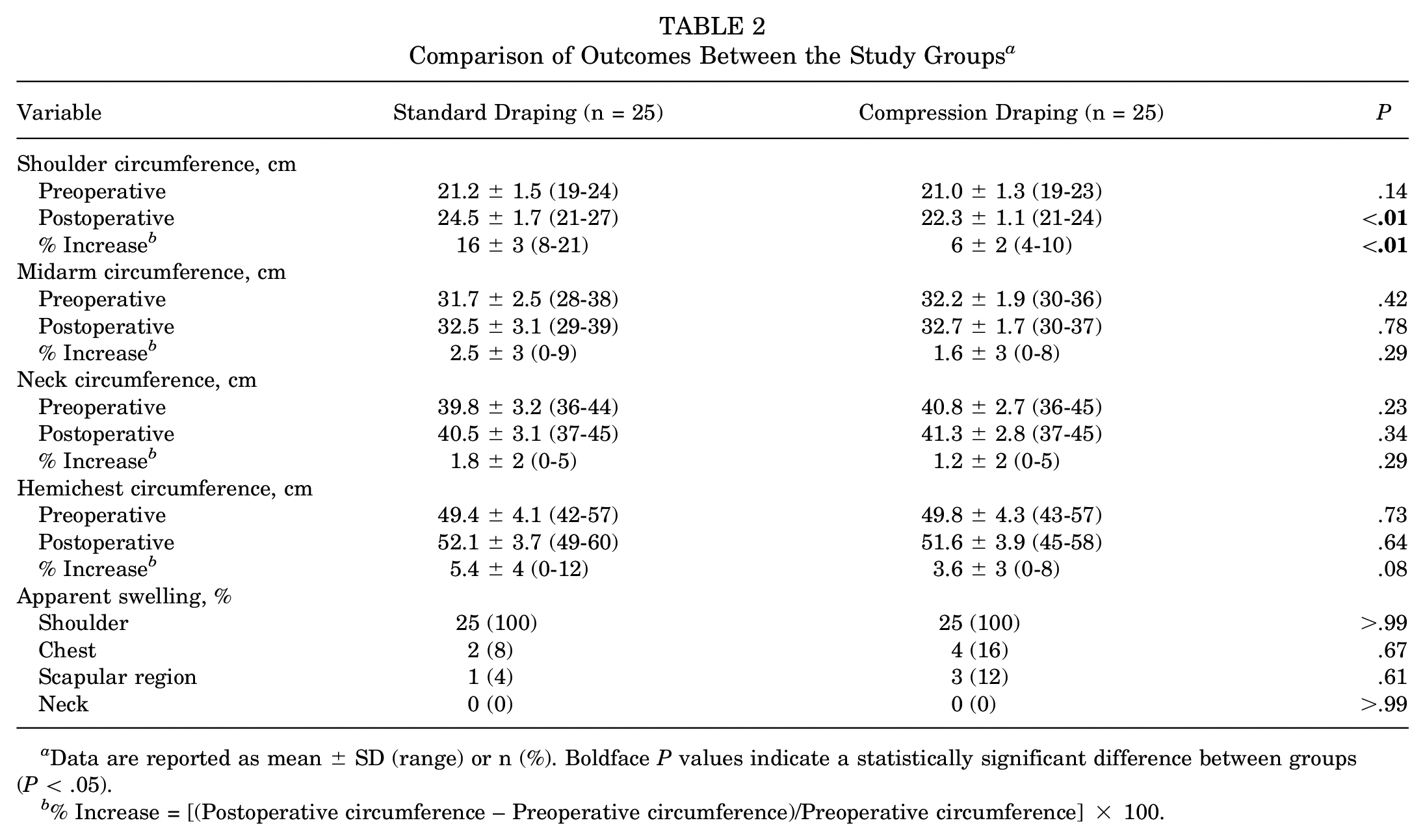
Data are reported as mean ± SD (range) or n (%). Boldface P values indicate a statistically significant difference between groups (P < .05).
% Increase = [(Postoperative circumference – Preoperative circumference)/Preoperative circumference] × 100.
Marked soft tissue edema at the deltoid region of the operated side, causing apparent deltoid asymmetry, was observed in all patients regardless of their group assignment. None of the patients demonstrated apparent soft tissue edema or swelling of the neck.
No significant complications (eg, respiratory, neurological, vascular, and infection) were observed during the 24-hour postoperative hospital stay and at the 2-week postoperative follow-up. Nevertheless, because the study was not powered to examine complication rate, this finding may be of limited value and should be interpreted with caution.
Discussion
In the current study, we found that compressive shoulder draping with an adhesive incise drape was effective in reducing soft tissue swelling around the shoulder in arthroscopic rotator cuff repair. We found a mean increase of 16% in shoulder circumference at the end of the procedure in our control group (using standard sterile draping) compared with only 6% in our study group (using compressive draping). The modest difference between our groups may be attributed to inclusion of only small- to medium-sized tears in the study, which resulted in a relatively short surgical duration with a relatively low volume of irrigation fluid.
The main concern regarding the use of compressive draping around the shoulder is that it may cause fluid shift toward the neck, chest, and scapular region, which may lead to an adverse reaction and especially airway obstruction. However, we found a similar rate of apparent swelling and a similar increase in circumference in those areas in both groups (Table 2), and no serious complications (eg, airway compromise, nerve damage, and infection) occurred in our cohort. To our knowledge, no previous study has evaluated the influence of applying compressive draping to the shoulder on soft tissue swelling in shoulder arthroscopy.
Previous studies have reported that the volume of fluid accumulated in the soft tissue after arthroscopic rotator cuff repair ranges from 1000 to 3000 mL and is correlated to the surgical duration, volume of irrigation fluid used, and size of the rotator cuff tear.7,10,14 Syed et al 14 reported that the use of fenestrated outflow cannulas with negative pressure was helpful in reducing soft tissue edema associated with longer arthroscopic procedures and increased irrigation fluid volume compared with conventional non-outflow cannulas. Measures for minimizing intraoperative bleeding such as hypotensive anesthesia (with systolic blood pressure between 90 and 100 mm Hg), epinephrine in the irrigation fluid, and strict bleeding control were found to facilitate a shorter surgical duration and lower fluid pressure environment, which contribute to reduced fluid extravasation and soft tissue edema.4,11 Because of the limited efficacy of those techniques, fluid extravasation and soft tissue edema remain a concern in arthroscopic shoulder procedures.
Limitations
Several potential limitations should be considered when interpreting our results. First, our cohort included only patients who underwent arthroscopic repair of superior rotator cuff tears <3 cm, which makes it difficult to generalize our findings to other shoulder arthroscopic procedures. Considering the potential benefit of the technique with no apparent downsides, we believe that its effect on reducing swelling should be investigated in other arthroscopic procedures of the shoulder. Second, fluid extravasation in our study was assessed by external measurements and observation rather than by quantitative assessments of fluid balance and patients’ weight, as reported in previous studies.5,14 Finally, the effect of reduced soft tissue swelling on the ease of performing the arthroscopic procedure and surgeon’s satisfaction was not assessed in this study, and the clinical significance of our findings remains unclear.
Conclusion
We found that compressive shoulder draping with an adhesive incise drape resulted in significant, albeit modest, reduction in soft tissue swelling around the shoulder in arthroscopic rotator cuff repairs compared with standard arthroscopic draping and was not associated with any adverse reactions. The clinical significance of our findings and their relevance to other shoulder arthroscopic procedures remain a subject for future studies.
Footnotes
Final revision submitted July 30, 2023; accepted August 17, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hillel Yaffe Medical Center (reference No. 0033-17-HYMC).