
Abstract
Background:
Acromioclavicular osteoarthritis and rotator cuff tears are commonly coincident.
Purpose:
To determine the rate of subsequent distal clavicle excision (DCE) when rotator cuff repair (RCR) is performed without DCE and the risk factors for subsequent DCE after RCR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
The operative logs of 2 surgeons from 2007 to 2016 were retrospectively reviewed for all patients who underwent RCR with or without DCE. Preoperative demographic data, symptoms, physical examination, and standardized outcomes (visual analog scale for pain, Simple Shoulder Test, and American Shoulder and Elbow Surgeons score) were noted. Acromioclavicular (AC) arthritis was classified on preoperative radiographs. The rate of subsequent surgery on the AC joint was determined via chart review, and univariate and multivariate analyses were conducted to determine risk factors for revision.
Results:
In total, 894 patients underwent isolated RCR, and 46 underwent concomitant RCR and DCE. On retrospective chart review, of those who underwent isolated RCR, the revision rate for any reason was 7.5% (67 patients), and the rate of subsequent AC surgery was 1.1% (10 patients). Preoperatively, 88% of the total cohort was considered to have a radiographically normal AC joint. On multivariate analysis of patients who underwent isolated RCR, the risk factors for subsequent AC surgery included preoperative tenderness to palpation at the AC joint (10% vs 63%, P < .001), female sex (35% vs 80%, P < .001), and surgery on the dominant side (60% vs 100%, P = .002). On multivariate analysis, these 3 factors explained 50% of the variance in revision AC surgery. When these 3 factors were present in combination, there was a 40% rate of revision AC surgery.
Conclusion:
This records review found that 10 of 894 (1.1%) rotator cuff repairs underwent subsequent distal clavicle resection. Risk factors for subsequent DCE included tenderness to palpation at the AC joint, female sex, and surgery on the dominant side, with subsequent DCE performed in 40% of cases with a combination of these 3 factors. Because the duration of follow-up was short and the number of reoperations small, some caution is recommended in interpreting these results, as the analyses may be underpowered.
Keywords
Acromioclavicular (AC) osteoarthritis (ACOA) is one of the most common pathologies of the shoulder. 20,27,30,31 The outcomes of distal clavicle excision (DCE), regardless of approach, are generally excellent. ‡ ACOA and rotator cuff tears are commonly coincident. 2,4,9,18,26,30 The outcomes of concomitant rotator cuff repair (RCR) and DCE are also excellent. 5,13,22,23
However, ACOA is age related and is present in up to 88.7% of asymptomatic individuals. 20,27,30,31 Thus, radiographic features of ACOA may not correlate with symptoms. 24 Indeed, 1 skeletal study suggested the AC joint to be among the most frequent joints in the body to undergo osteoarthritic changes. 31 However, DCE remains a very commonly performed procedure. 1 In the setting of a rotator cuff tear, it can be difficult to determine the contribution of concomitant ACOA to the patient’s symptomatology. Some authors have also thought that distally pointing osteophytes from ACOA may cause rotator cuff tears. 4,26 One retrospective study demonstrated superior outcomes with combined DCE + RCR as compared with isolated RCR. 28 To determine whether DCE improves outcomes in the setting of RCR, 3 randomized clinical trials were performed that determined that DCE does not improve outcomes with concomitant RCR with radiographic ACOA, asymptomatic ACOA, or symptomatic ACOA. 13,22,23
Furthermore, DCE is not without disadvantages. Resection of as little as 5 mm of distal clavicle reduces AC joint stiffness in cadaveric models. 6,14 Clinically, violation of the AC joint leads to radiographic instability in up to 38% of patients, 15 residual symptoms in up to 40% of patients, 8 and a poor outcome in up to 13% of patients. 17 DCE also extends surgical time, may involve additional portals, and requires the introduction of additional instruments and debris into the subacromial space, which could increase infection rates or postoperative pain.
One traditional argument for concomitant DCE and RCR has been that it reduces the reoperation rate for late DCE. Traditionally, subsequent DCE has been performed in 7% to 28% of cases after subacromial decompression. 3,7,11,21 If the AC joint is violated during subacromial decompression, subsequent DCE may be necessary as frequently as 39% of the time but is rarely subsequently necessary if the AC joint is not violated. 8 If subsequent DCE is rare after RCR, with sample sizes of 83, 13 78, 22 and 58, 23 the currently available randomized clinical trials may not be adequately powered to find a difference in this relatively infrequent complication. The purpose of this study was to determine the rate of subsequent DCE when RCR is performed without DCE and the risk factors for subsequent DCE after RCR. We hypothesized that DCE would be infrequently performed after RCR.
Methods
Design
This was a retrospective comparative study that was found exempt from review by an institutional review board. The case logs of the senior authors (R.Z.T. and R.T.B.) were reviewed. Inclusion criteria comprised (1) history of arthroscopic RCR (Common Procedural Terminology code 29827) and/or arthroscopic or open DCE (codes 29824 and 23120) and (2) surgical date between January 1, 2007, and April 1, 2016. Patients who underwent medial clavicle excision or excision of the middle of the clavicle were also excluded. The study dates were selected because patients prior to 2007 were not included in our electronic medical record. Patients after April 1, 2016, were excluded to provide a year for reoperation, although there were no exclusions based on length of follow-up. Because this was a retrospective study, preoperative data for those patients who underwent concomitant DCE and RCR were compared with data for those who underwent isolated RCR to examine for selection bias.
Data Collection
The following demographic data were collected via chart review: age, sex, hand dominance, and whether the patient had an open workers’ compensation claim. The following historical data were collected: whether there was a history of trauma and the timing of this trauma, the duration of the preoperative symptoms, whether the patient had a history of surgery on the ipsilateral shoulder, whether the patient had symptoms referable to the AC joint, and preoperative scores, including the Simple Shoulder Test, a visual analog scale for pain, and the American Shoulder and Elbow Surgeons score. The following physical examination data were collected: whether the patient had tenderness to palpation (TTP) at the AC joint, whether the patient had pain with a cross-body adduction test, and whether the patient had a preoperative injection and, if so, what the location of the injection was and whether that improved symptoms. As this was a retrospective study, no a priori standardized protocol was used to decide whether to perform DCE at the time of RCR. Each included surgeon decided on a case-by-case basis whether to perform DCE. Generally, during the 9-year study period, a variety of RCR techniques were performed with no standardization. During this same period, DCE was performed from a subacromial approach with a high-speed cylindrical bur but again with no a priori standardization.
Radiographic Analysis
Preoperative radiographs were reviewed and the AC joint evaluated and graded for severity of arthritis per the Petersson classification by 2 attending orthopaedic surgeons with fellowship training in shoulder and elbow surgery, each of whom was blinded to the grade of the other reviewer (P.N.C. and R.Z.T.) (Figure 1). 23,27 Preoperative radiographs were evaluated to determine whether there was any osteolysis of the distal clavicle. We did not evaluate preoperative magnetic resonance images, as these were only variably available.

Anteroposterior radiographs providing examples of acromioclavicular osteoarthritis grades (A) 0, (B) 1, (C) 2, and (D) 3, as well as (E) distal clavicular osteolysis. The difference between grades 2 and 3 is primarily with regard to the size of the periarticular osteophytes. 27
Revision Analysis
Via chart review, we determined whether there were any complications and/or subsequent operations and, if so, their exact nature. The operative reports for each subsequent surgery were reviewed and categorized into the most frequently encountered reasons for reoperation: revision AC surgery, revision for stiffness, revision for retear of the rotator cuff, and revision for infection.
Statistical Analysis
Continuous variables for those patients who underwent RCR but did not undergo subsequent DCE were compared with those who did undergo subsequent DCE via Mann-Whitney U tests and Student t tests, depending on data normality as determined with the Kolmogorov-Smirnov test. Categorical variables for those patients who underwent RCR but did not undergo subsequent DCE were compared with those who underwent subsequent DCE via Fisher exact tests. For ACOA radiographic grade, interrater reliability was determined with the Cohen kappa coefficient, with agreement graded as slight (0-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), and perfect (0.81-1). 16 Radiographs were also secondarily analyzed as “normal” (ie, grade 0) or “abnormal” (grades 1-3 or osteolysis) via a consensus method. Those variables that differed between groups with a P value <.1 were then included in a stepwise multivariate logistic regression analysis with R 2 estimated via the Nagelkerke method. 19 All data analysis was performed in Excel X (Microsoft Corp) and SPSS (v 23; IBM Corp). P values <.05 were considered statistically significant.
Results
In total, 940 patients met our inclusion criteria, of whom 894 underwent an isolated RCR and 46 underwent concomitant RCR + DCE; the mean ± SD follow-up was 0.7 ± 0.8 years. Regarding demographics, those patients who underwent isolated RCR were significantly older (P = .001) and were more likely to have a history of trauma (P = .019) than those who underwent RCR + DCE. Otherwise, there were no significant demographic differences between groups (Table 1). In terms of clinical data, significantly more patients in the RCR + DCE group had preoperative symptoms referable to the AC joint (P < .001). For the preoperative physical examination, significantly more patients in the RCR + DCE group had tenderness at the AC joint and a positive cross-body adduction test result (P < .001 in each case). Regarding the preoperative standardized outcome measures, there was no statistical difference in results between groups.
Preoperative Data for the Isolated RCR and Combined RCR + DCE Groups a

a Values are presented as mean ± SD for continuous data and % (proportion of patients for which the data were available/relevant) for discrete data. Bolded P values indicate statistically significant between-group differences, P < .05. AC, acromioclavicular; ASES, American Shoulder and Elbow Surgeons; DCE, distal clavicle excision; RCR, rotator cuff repair; VAS, visual analog scale.
There were also no differences between groups in preoperative radiographic grading of AC arthrosis (Table 1). Preoperatively, 88% of those who underwent isolated RCR were considered to have a normal AC joint, with a mean radiographic grade of 1.56 ± 0.99. 27 When radiographs were graded, the Cohen kappa was 0.707 (P < .0001), representing substantial agreement.
The likelihood of reoperation did not differ between groups (Table 2). Of those who underwent isolated RCR, the overall revision rate was 7.5% (67 patients), and the rate of subsequent AC surgery was 1.1% (10 patients) (Table 2). These operations were performed 1.2 ± 1.1 years after RCR. There were no rotator cuff retears noted on these 10 specific procedures, although an additional 37 patients underwent revision for rotator cuff retear.
Revision Rates for the Isolated RCR and Combined RCR + DCE Groups a
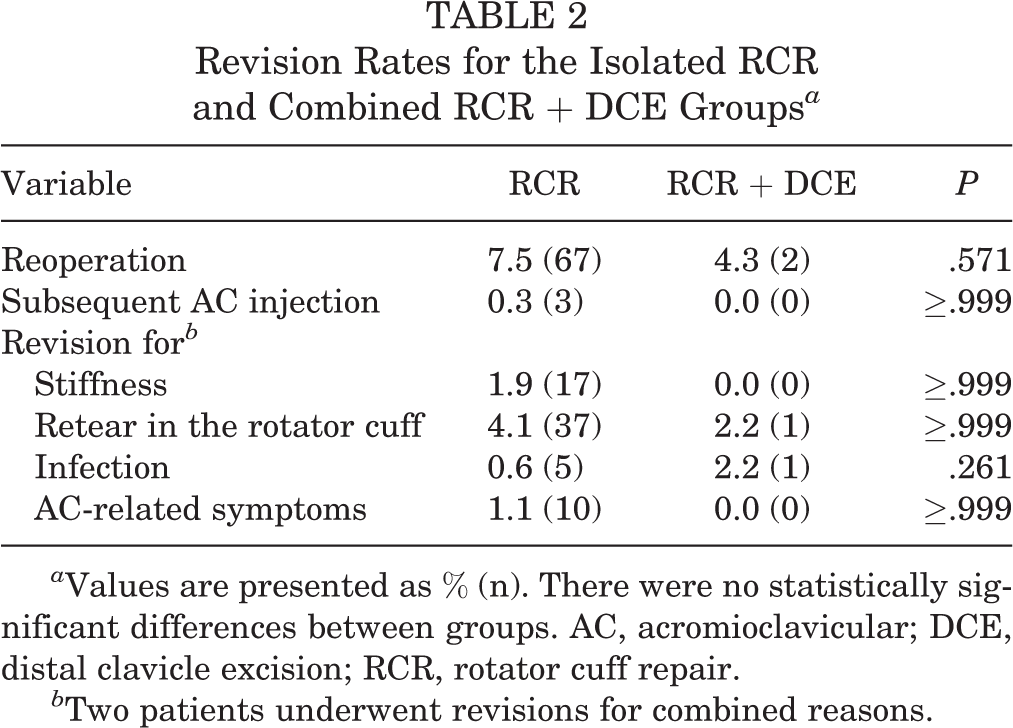
a Values are presented as % (n). There were no statistically significant differences between groups. AC, acromioclavicular; DCE, distal clavicle excision; RCR, rotator cuff repair.
b Two patients underwent revisions for combined reasons.
Patients who underwent RCR + DCE were excluded from our analysis of the risk factors for subsequent AC surgery. Risk factors for subsequent AC surgery on univariate analysis are presented in Table 3. There were no differences in radiographic grade of ACOA (P = .698) or the percentage of patients with a radiographically normal AC joint (P = .593) between those who underwent revision and those who did not. On multivariate analysis, AC TTP, female sex, and surgery on the dominant side were all significant predictors of need for revision AC surgery (Table 4). In combination, these 3 factors had an R 2 value of 0.50, suggesting that 50% of the variance in the need for further AC surgery could be predicted by these 3 values alone. When 2 of these factors were present, the rate of further AC surgery was 3.4% to 6.4% depending on the combination of factors. When these 3 factors were present in combination, the rate of further AC surgery was 40%. For those patients with AC TTP, the subsequent revision rate was 9.6%.
Preoperative Data for Patients Who Did and Did Not Require AC Joint Revision a

a Values are presented as mean ± SD for continuous data and % (proportion of patients for which the data were available/relevant) for discrete data. The cross-body adduction test was recorded for 115 patients who did not undergo revision, and 86 patients who did not undergo revision had a prior AC injection. Statistically significant P values are bolded, P < .05. AC, acromioclavicular; ASES, American Shoulder and Elbow Surgeons; NA, not available; RCR, rotator cuff repair; VAS, visual analog scale.
Multivariate Analysis Results a

a AC, acromioclavicular.
Discussion
We hypothesized that DCE would be infrequently performed after RCR, and we found that indeed, DCE was infrequently performed (1.1%) after RCR. Risk factors for subsequent DCE on multivariate analysis included TTP at the AC joint, female sex, and surgery on the dominant side. When these risk factors were present in combination, subsequent DCE was performed in 40% of cases.
Within our cohort, only 1.1% of patients underwent subsequent DCE after RCR, similar to previous studies. 13,22,23 For instance, in the 3 randomized clinical trials, Kim et al 13 included 52 patients who underwent RCR without DCE and only 1 underwent revision DCE; Oh et al 22 included 39 patients who underwent RCR without DCE, with no revision DCEs performed; and Park et al 23 included 32 patients who underwent RCR without DCE, with no revision DCEs performed. However, some retrospective studies have suggested that the rate may be significantly higher. In a 2009 retrospective comparative study of arthroscopic and open DCE, Elhassan et al 7 included 105 patients, of whom 11 (10.5%) had undergone a prior RCR. In an older analysis (2000) of failed subacromial decompressions, physical and differential examinations revealed AC symptoms to be a contributing factor in 28%. 3 A similar historical (1989) analysis revealed AC symptoms to be a contributing factor in 20%. 11 A third analysis from a similar period (1990) revealed AC symptoms to be contributing factor in 7.5% of failed subacromial decompressions. 21
Our results are similar to the more recent randomized clinical trials supporting a low revision rate. The prior trials are nonconcordant with respect to outcomes, as Kim et al 13 found better outcome scores among patients who underwent concomitant DCE, while Oh et al 22 and Park et al 23 did not find any differences in outcome scores. In addition, for unclear reasons, the rate of radiographic osteoarthritis was substantially lower in our study than in historical studies. 20,27,30,31 Our study found that reoperation for subsequent DCE after RCR is uncommon, suggesting that DCE may be avoided in the majority of cases.
Within our study, predictors for the need for revision AC surgery included female sex, surgery on the dominant side, and TTP at the AC joint. These risk factors may allow the findings of the 3 prior randomized clinical trials to be reinterpreted. For instance, Kim et al 13 and Oh et al 22 excluded patients with preoperative AC TTP. However, in their randomized study, Park et al 23 included only patients with preoperative AC TTP. In addition, most of their cohort was female (38 of 47, 81%). However, in most cases, the dominant extremity was not involved (29 of 47, 62%). These exclusions may be the reason why no difference was found in these studies. These authors did not find any postoperative differences between patients who underwent concomitant DCE and those who did not, even when all had preoperative symptomatic ACOA; however, the authors had relatively small cohorts to make these comparisons. 23
Our results suggest that further study with these risk factors may be helpful to better determine the need for DCE at the time of RCR. Interestingly, preoperative outcome scores (visual analog scale, Simple Shoulder Test, and American Shoulder and Elbow Surgeons) did not differ between those patients who did and did not undergo DCE or between those patients who did and did not require revision for the AC joint. In addition, preoperative AC injections were not predictive of the need for a concomitant DCE, as 83 patients in the isolated RCR group had a preoperative AC injection with relief, did not undergo a DCE, and did not require revision AC surgery. We thus cannot recommend AC injections to evaluate for the need for concomitant DCE.
Strengths of the study include the size of the cohort and the comparative design. Limitations include the retrospective design and chart review for information. Short duration of follow-up is another weakness, as a longer follow-up period may alter revision rates. Because this was a single-institution retrospective chart review study, patients who had revision procedures performed outside our institution would not have been captured by this study. Furthermore, despite a large sample size, only a small number of patients required reoperation, thereby providing a small comparison group; thus, some comparisons may be underpowered. In addition, the preoperative evaluation was not performed in a standardized or consistent manner. However, this limitation applies equally to the RCR group and the RCR + DCE group. The physical examination was not performed in a prospectively standardized manner.
There was significant heterogeneity within the cohort with regard to surgical indications for revision DCE, operative approach, RCR technique, clavicle resection technique, and postoperative rehabilitation protocol. Heterogeneity in procedural indications can create selection bias. However, this heterogeneity applied to both the revised and the nonrevised control groups. In addition, this heterogeneity increases the generalizability of our findings. Furthermore, there was no standardized protocol used to decide whether to perform DCE or a revision operation, as this is a retrospective study. Residual unmeasured bias may exist between groups. To mitigate the effect of potential selection bias, preoperative functional outcome scores from those who underwent concomitant DCE + RCR were compared with those who underwent isolated RCR, and no differences were found, aside from the younger age of those who underwent DCE + RCR. Finally, we were not able to include some variables that may predict the need for DCE, such as range of motion, specific measurement of AC instability, and Constant scores, as these were not uniformly available retrospectively.
Conclusion
This retrospective records review identified 10 of 894 (1.1%) RCRs that underwent subsequent distal clavicle resection because of symptoms. Our study indicates that reoperation for subsequent DCE after RCR is uncommon, suggesting that DCE may be avoided in the majority of cases. Risk factors for subsequent DCE include TTP at the AC joint, female sex, and surgery on the dominant side. When these risk factors were present in combination, subsequent DCE was performed in 40% of cases. Because the duration of follow-up was short and the number of reoperations small, some caution is recommended in interpreting these results, as the analyses may be underpowered.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: P.N.C. is a paid consultant for DePuy Mitek and has received hospitality payments from Tornier. R.T.B. receives royalties from Arthrex, has stock in KATOR, is a paid consultant and paid presenter/speaker for DePuy Mitek, and has received educational support from Pinnacle. R.Z.T. has received consulting fees from DePuy, Cayenne Medical, and Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the University of Utah Institutional Review Board (00071740).