
Abstract
Background:
Failure after isolated Bankart repair has led surgeons to consider when to address the Hill-Sachs lesion, which is thought to be a contributor to recurrent instability. One approach utilizes the glenoid track concept to determine whether a Hill-Sachs lesion is classified as “off-track,” suggesting that the addition of a remplissage procedure may aid stability. However, the accuracy and reliability of using this approach require validation using an appropriate reference.
Purpose:
To determine the accuracy and reliability of using the glenoid track concept against dynamic arthroscopic assessment of Hill-Sachs lesion engagement.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 49 patients undergoing arthroscopic Bankart repair surgery for recurrent traumatic anterior shoulder instability were enrolled in this diagnostic validation study. Shoulders were classified as on-track or off-track using 3-dimensional computed tomography (3DCT) and static arthroscopic measurements. These classifications were compared with dynamic arthroscopic assessment (engagement of the Hill-Sachs lesion on the anterior glenoid rim in the ‘athletic position’) to determine their accuracy and reliability.
Results:
The 3DCT-based measurements to determine glenoid track status had a higher positive predictive value (66% vs 42%), higher specificity (47% vs 42%), and higher accuracy (65% vs 59%) compared with static arthroscopic measurements. Static arthroscopic measurements to determine glenoid track status had a higher negative predictive value (96% vs 64%) and higher sensitivity (96% vs 81%) compared with 3DCT-based measurements. Interrater reliability (Krippendorff α) was ‘fair’ for determining the glenoid track status using 3DCT (0.368; 95% CI, 0.217-0.519) and ‘moderate’ for static arthroscopic measurements (0.523; 95% CI, 0.364-0.666). Intrarater reliability (intraclass correlation coefficient [ICC] 3,k) was ‘moderate’ for 3DCT measurements (0.660; 95% CI, 0.444-0.798) and ‘good’ for static arthroscopic measurements (0.769; 95% CI, 0.629-0.862).
Conclusion:
Determining glenoid track status using either 3DCT or static arthroscopic measurements yielded moderate accuracy and reliability. Surgeons using the glenoid track concept to aid surgical decision-making in traumatic recurrent anterior shoulder instability should utilize 3DCT or static arthroscopic measurements with caution.
Recurrent traumatic anterior shoulder instability remains a common problem encountered by shoulder surgeons. 4 Surgical stabilization is often needed to prevent further episodes of instability. While the most common procedure performed for shoulder instability in many countries is an arthroscopic Bankart repair, 4 the need for an adjunctive procedure continues to be refined. Hill-Sachs lesions are commonly found in recurrent traumatic anterior instability. A remplissage procedure, whereby the posterior capsule and infraspinatus tendon are tenodesed into the Hill-Sachs lesion, “filling in” the defect, has been used invariably. Deciding when to include a remplissage with an arthroscopic Bankart repair remains a contentious issue of debate. While bone lesions of the glenoid and humerus were initially quantified and evaluated in isolation in recent years, a greater emphasis has been placed on assessing combined bone loss.
The concept of the glenoid track has become popular as a means of quantifying glenoid and humeral bone loss. 15 This technique was developed using a cadaveric model and describes the track the glenoid articular surface takes on the humeral head during motion. This method requires the user to calculate the Hill-Sachs interval (HSI) and the glenoid track width (GTW). The HSI is the widest part of the Hill-Sachs defect plus the bony bridge from the edge of the defect to the insertion of the rotator cuff. 2 The GTW is calculated by multiplying the true glenoid width by 0.83. The true glenoid width is determined using a circle method to calculate the diameter of the circle minus the width of the bone lost. If the GTW is greater than or equal to the HSI, it is determined to be “on-track.” If the GTW is lower than the HSI, then it is determined to be “off-track.” Off-track lesions are considered to be at high risk for failure with arthroscopic Bankart repair alone, leading some surgeons to determine which patients should have a remplissage and/or a bony procedure for the anterior glenoid. 5 Intraoperatively, these same measurements (HSI and GTW) may be measured, as well as the dynamic assessment of the Hill-Sachs lesion with the anterior glenoid rim. The concept of the “engaging” Hill-Sachs lesion was described by Burkhart and De Beer. 1 Hill-Sachs lesions that engaged the anterior glenoid rim at 90° of abduction and 0° to 30° of external rotation were similarly at higher risk of failure of an arthroscopic Bankart repair. 1
There remains uncertainty as to which method is optimal for achieving successful surgical decision-making. For some, the glenoid track concept has superseded the engaging Hill-Sachs concept. However, there remains significant dissonance among surgeons as to which method adds the most value to surgical decision-making. The aim of this study was to determine the reliability, accuracy, and correlation of the glenoid track with the arthroscopic assessment of engaging Hill-Sachs lesions.
Methods
Study Patients
The study protocol received institutional review board approval. Study inclusion criteria were any adult patient (>18 years of age) undergoing arthroscopic stabilization surgery (ie, Bankart repair) for recurrent traumatic anterior shoulder instability with preoperative computed tomography (CT) imaging. Eligible patients needed to be fluent in English to be able to comply with the study and provide informed consent. Patients undergoing open surgery, bone block procedures, revision surgery, and Latarjet procedures were excluded, as were patients with multidirectional instability, connective tissue disorders, and workers’ compensation claims. Patients meeting these criteria were invited to participate in the study after giving consent for surgery.
Preoperative Imaging
Three-dimensional CT (3DCT) was performed on all patients preoperatively. The glenoid track was measured as described by Di Giacomo et al. 2 Briefly, the 3DCT scan was oriented to provide an en face view of the glenoid, and a best-fit circle was drawn to fit the inferior two-thirds of the glenoid (Figure 1). The largest distance within the circle and through the glenoid defect was measured (D in Figure 1). Then, the largest distance from the edge of the circle to the glenoid rim, determining the largest bone loss measurement, was calculated (d in Figure 1). The GTW was calculated as D(0.83) –d. The HSI was calculated using a posterior view of the humeral head on 3DCT. The medial margin of the Hill-Sachs defect (point a), lateral margin of the Hill-Sachs defect (point b), and medial margin of the rotator cuff footprint (point c) were identified. The HSI was calculated by combining the measurement of the bony bridge (distance from points b to c) and the Hill-Sachs lesion width (distance from points a to b), which is the distance from the medial margin of the rotator cuff footprint to the medial margin of the Hill-Sachs defect. If the GTW was greater than the HSI, the shoulder was deemed on-track. If the GTW was smaller than the HSI, the shoulder was deemed off-track.

3DCT measurements. (A) En face view of glenoid fossa with best fit circle drawn. Red line shows glenoid width within the best fit circle (D). Yellow line shows width of bone loss area within best fit circle (d). Glenoid Track width = 0.83(D) - d. (B) Posterior view of proximal humerus. Grey shaded area denotes the Hill Sachs defect. Point a denotes the medial margin of the HS defect. Point b shows the lateral margin of the Hill Sachs defect. Point c shows the insertion of the posterior rotator cuff. The Hill Sachs Interval = Hill Sachs width (distance between points a and b) + Bony Bridge (distance between points b and c).
Arthroscopic Assessment
Each patient underwent static and dynamic assessments of their glenoid and humeral bone lesions at the time of arthroscopy. All arthroscopic measurements were video recorded. Static measurements were performed as follows (Figure 2).

Static arthroscopic measurements used to measure glenoid track width and Hill-Sachs interval. (A) Posterior radius of the glenoid measured from the middle of the bare spot to the posterior glenoid rim. (B) Anterior radius of the glenoid measured from the middle of bare spot to the anterior glenoid rim. (C) Hill-Sachs (HS) lesion width. (D) Bony bridge (BB) measured from the lateral margin of the Hill-Sachs lesion to the rotator cuff insertion. Glenoid track width = 0.83(posterior radius × 2) – (posterior radius – anterior radius). Hill-Sachs interval = HS + BB.
Glenoid Track Width
While viewing from the anterosuperolateral portal, a calibrated probe (Arthrex) was placed via the posterior portal. At the level of the glenoid bare spot, the posterior radius was measured (from the middle of the bare spot to the posterior rim of the glenoid). Care was taken to ensure the orientation of the probe as tangential to the glenoid face, perpendicular to the bone loss and centered over the inferior aspect of the glenoid. The native glenoid width (D) was calculated by multiplying this distance by 2. The anterior radius was measured from the middle of the bare spot to the anterior glenoid rim. The glenoid bone loss (d) was calculated by subtracting the anterior radius measurement from the posterior radius measurement. The GTW was calculated as before (D[0.83] –d) using the arthroscopic measurements outlined.
Hill-Sachs Interval
While viewing from the anterosuperolateral portal, a calibrated probe (Arthrex) was placed via the posterior portal. The bony bridge between the lateral margin of the Hill-Sachs lesion and the medial margin of the rotator cuff insertion was measured. The width of the Hill-Sachs lesion from the medial to the lateral margin was also measured. Care was taken to ensure that the measurement was made at the widest part of the Hill-Sachs lesion. The HSI was calculated as above by combining the distances for the bony bridge and the Hill-Sachs lesion width. If the GTW was greater than the HSI, the shoulder was deemed on-track. If the GTW was smaller than the HSI, the shoulder was deemed off-track.
Dynamic arthroscopic assessment was performed as follows. Before soft tissue release or repair, the arm was removed from the limb positioner and the shoulder was taken through the “athletic range of motion” as described by Burkhart and De Beer. 1 This consisted of placing the shoulder in 90° of abduction and maximal extension and a combination of external rotation ranging from 0° to 100°. If the Hill-Sachs lesion engaged (ie, came into contact) with the anterior glenoid rim, the lesion was considered “engaging.” For the purposes of this study, both the static arthroscopic and radiological measurements were compared with the dynamic arthroscopic assessment of engagement as the reference to determine glenoid track status.
Outcome Measures
The primary outcome of this study was the accuracy of the glenoid track concept in determining which lesions were on-track versus off-track. Both 3DCT and static arthroscopic measurements were compared with the dynamic arthroscopic assessment as the reference standard. The secondary outcomes were the inter- and intrarater reliability of (1) 3DCT to classify Hill-Sachs lesions and (2) static arthroscopic measurements to classify Hill-Sachs lesions using dynamic arthroscopic assessment as the reference standard for comparison.
Statistical Analysis
Accuracy to determine shoulders that were on-track versus off-track using the CT-based and static arthroscopic measurements was calculated by dividing the summation of the true-positive and true-negative results by the summation of true-positive, true-negative, false-positive, and false-negative results. The interrater reliability was calculated using the Krippendorff α. The intrarater (test-retest) reliability was determined by the 2-way mixed random average measures intraclass correlation coefficient (ICC) (ICC 3, k; using the Shrout and Fleiss convention). For interrater reliability, we used the convention outlined by Landis and Koch, 7 in which values >0.80 were deemed almost perfect, 0.61 to 0.80 substantial, 0.41 to 0.60 moderate, 0.21 to 0.40 fair, and 0.0 to 0.20 slight agreement. For intrarater reliability, we used the categories suggested by Koo and Li, 6 in which ICC values <0.5 were interpreted as having poor, 0.5 to 0.75 moderate, 0.75 to 0.9 good, and >0.9 excellent agreement.
Sensitivity was calculated by dividing the true-positive results by the sum of true-positive and false-negative results. Specificity was calculated by dividing the true-negative results by the sum of true-negative and false-positive results. The negative predictive value was calculated by dividing the true-negative results with the sum of true-negative and false-negative results. The positive predictive value was calculated by dividing the true-positive results by the sum of true-positive and false-positive results.
Results
A total of 49 patients were included in this study. Three fellowship-trained attending surgeons (I.K.Y.L., J.L., and A.J.B.) performed arthroscopic stabilization surgery on these patients. The mean age of the patients was 31 years (range, 19-47 years). The cohort comprised 38 men and 11 women. Right shoulders were involved in 30 patients and left shoulders in 19. The mean glenoid bone loss on 3DCT was 14.0% (range, 1.9%-32.7%). On average, 28 of 49 (57.1%) shoulders were deemed off-track. Static arthroscopic measurements to determine the HSI and GTW were comparable to 3DCT-based measurements (Table 1). When comparing to our reference standard of dynamic arthroscopic assessment of Hill-Sachs lesion engagement, 3DCT measurements were more specific, less sensitive, and more accurate than static arthroscopic-based measurements.
Performance of 3DCT and Static Arthroscopic Measurements to Determine Glenoid Tracking Compared With Dynamic Arthroscopic Assessment of Hill-Sachs Lesion Engagement a

PPV, positive predictive value; NPV, negative predictive value; 3DCT, 3-dimensional computed tomography.
Interrater reliability for determining glenoid tracking was deemed as ‘fair’ for 3DCT and ‘moderate’ for arthroscopic-based measurements. Intrarater reliability was ‘moderate’ for 3DCT and ‘good’ for arthroscopic-based measurements (Table 2).
Interrater and Intrarater Reliability of Determining Glenoid Tracking Using 3DCT-based Measurements and Static Arthroscopic-Based Measurements a
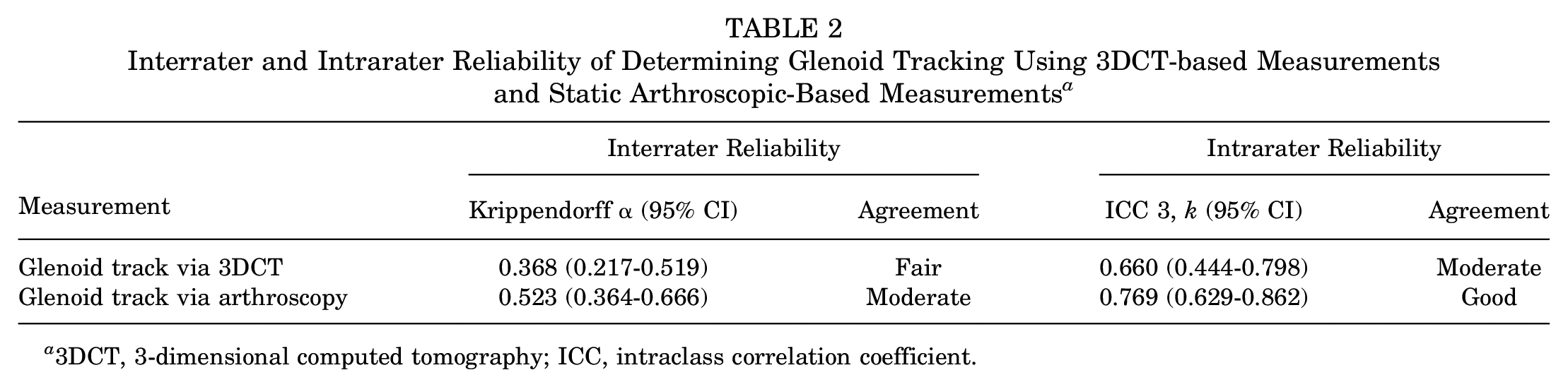
3DCT, 3-dimensional computed tomography; ICC, intraclass correlation coefficient.
Discussion
In this study, we found that both 3DCT and arthroscopic measurements of the glenoid track (i.e., on-track or off-track) had moderate accuracy and reliability. The question remains as to whether applying the glenoid track concept to surgical decision-making in this patient cohort is robust enough to yield superior clinical outcomes. Precision (positive predictive value) and accuracy were slightly higher when 3DCT-based measurements were used; however, the negative predictive value and sensitivity were greater when arthroscopic measurements were used to determine the HSI and GTW. The inter- and intrarater reliability was also greater when using arthroscopic measurements compared with 3DCT; however, there was only moderate to good reliability observed.
Several previous studies have attempted to validate the utility of the glenoid track concept using a variety of techniques. Schneider et al 12 validated the glenoid track using 3DCT in 71 shoulders and 4 raters. They reported a 72% interobserver reliability, with intraobserver reliability between 80% and 90%. Their study was adequately powered to test reliability between raters and within raters at different time points, which is different from our current study, which focused on testing the reliability of the glenoid track status, measured arthroscopically and on 3DCT, with a reference standard (dynamic arthroscopy). Our study demonstrates that while surgeons may be moderately reliable at assessing the glenoid track status, there may be instances when a patient is deemed off-track at one assessment, only to be found to be on-track at another assessment by the same surgeon. Funakoshi et al 3 retrospectively reviewed 16 shoulders, comparing arthroscopic calculations versus 3DCT to calculate the glenoid track status. They reported no difference in HSI measurements, although a greater Hill-Sachs lesion width was reported with 3DCT. The Cohen κ value between the 2 techniques was only 0.16 (none to slight agreement), with 3DCT classifying more shoulders as on-track compared with arthroscopy (15 vs 9). 3 This may be a reflection of the small number of patients used to test reliability. The lack of agreement is interesting and may be related to a number of factors. The 3DCT measurements may sometimes be recorded obliquely, leading to larger than observed Hill-Sachs lesion width. Similarly, it is difficult to appreciate the “bare area” on the posterior humeral head to which the infraspinatus attaches just lateral, further explaining why the HSI (which takes into account this area, ie, the “bony bridge”) may be measured smaller on 3DCT compared to arthroscopy. Our study used the data of 49 patients, increasing its power to determine the reliability between observers and time points.
The original study describing the concept of the glenoid track included experiments conducted on 9 fresh-frozen cadavers. 15 Using a custom apparatus, the authors placed shoulders in maximal extension and external rotation while varying the degrees of abduction. They reported that at 60° of glenohumeral abduction, the glenoid track measured 84% ± 14% of the glenoid width. This corresponds similarly to the “athletic position” for evaluating the engagement of Hill-Sachs lesions as originally described by Burkhart and De Beer. 1 Subsequent to this description, the glenoid track has been used as a method of guiding treatment, including utilization of the remplissage procedure and glenoid bony augmentation. 2
Recently, the glenoid track concept has further evolved to describe peripheral and central Hill-Sachs lesions in terms of percent occupancy of the glenoid track. 17 In a study of 50 patients with on-track shoulders, Yamamoto et al 17 used 3DCT to calculate the location of the Hill-Sachs lesion in relation to 4 zones of the glenoid track (divided into 25% increments). They concluded that patients with Hill-Sachs lesions located within the most medial 25% of the glenoid track (zone 4) had significantly worse outcomes based on Western Ontario Shoulder Instability Index scores. These lesions were deemed ‘peripheral track lesions’ and despite their being on-track, Yamamoto et al 17 recommended remplissage in this situation.
In the current study, however, when considering the overall accuracy and reliability of the glenoid track, determining surgical indications based on a single factor should be done with caution. While we attempted to replicate the glenoid track measurement and engagement of the Hill-Sachs lesion as originally described, laboratory studies have demonstrated an alteration in the glenoid track measurement with changes in arm position. In 1 study using open MRI on 30 healthy volunteers, the authors found that the GTW ranged from 89% ± 14% at 60° of abduction to 81% ± 10% at 150° of abduction. 10 In another study by the same group, the authors examined the influence of arm position (flexion-extension) and rotation (internal-external) on GTW using 10 fresh-frozen cadavers and reported a linear relationship with decreasing GTW as the arm is more extended and externally rotated. 16 Additionally, several clinical studies have reported on-track Hill-Sachs lesions in patients with recurrent instability.5,9,11,13,14 One study demonstrated that the addition of a remplissage procedure in “on-track” lesions reduced the rate of failure. 8 Clearly, further study is required to determine the most accurate and reliable method of calculating the glenoid track and which method correlates best with clinical outcome. Ultimately, static measurements of the glenoid and humerus, whether taken on magnetic resonance imaging, magnetic resonance angiography, 3DCT, or arthroscopy, may not provide sufficiently accurate and/or reliable information to determine how best to manage patients with traumatic recurrent anterior shoulder instability.
Strengths and Limitations
The strengths of this study are that we included patients treated by 3 different fellowship-trained shoulder surgeons, thereby increasing the external validity of our findings. Second, all patients underwent a systematic assessment using 3DCT as described by the original authors of the glenoid track concept. Arthroscopic assessments, both static and dynamic, were performed using a systematic method that was consistent across all patients and compared with a defined reference standard (dynamic arthroscopic assessment).
The limitations of this study are the inherent heterogeneity of this patient population. While we excluded those with multidirectional instability, collagen disorders, and posterior instability, we still had a reasonable range of glenoid bone loss (2%-33%; mean, 14%). This is, however, representative of the surgical population among the 3 surgeons’ practices undergoing soft tissue stabilization surgery. Despite our standardizing the static arthroscopic measurements, there remains some potential for subjectivity in these measurements. For example, for the glenoid measurements, we asked surgeons to measure from the middle of the bare spot of the glenoid, which may not be consistently determined between surgeons. However, it is unlikely that this measurement varies >1 to 2 mm. We attempted to standardize how these measurements were taken, but there was nonetheless likely some degree of variance.
Dynamic assessment of engagement was used as the reference with which glenoid track status was compared. Dynamic assessment during arthroscopy is in itself a flawed concept. Because the patient is anesthetized, this assessment does not take into account the action of the rotator cuff and scapular stabilizing muscles in the awake patient to provide dynamic stability to the glenohumeral joint. It has been suggested that Hill-Sachs engagement should be assessed after completion of the Bankart repair to determine the need for adjunctive remplissage. In practice, surgeons are understandably hesitant to place the arm is the extremes of external rotation, extension, and abduction, as this may unduly stress the repair. Another suggestion is to provide a posteriorly directed force to center the humeral head as dynamic assessment is performed. We do not believe this adequately replicates physiological conditions, especially in the earlier phases of postoperative rehabilitation, where patients are still developing appropriate proprioceptive feedback and dynamic scapular stability. Dynamic assessment of the Hill-Sachs lesion to engage the glenoid rim in the anesthetized patient may overrepresent the lesions that require remplissage; however, given the medium-term failure rate of isolated Bankart repair, there is little evidence to support this.
Conclusion
Study findings indicated that using static arthroscopic-based measurements to determine the HSI and GTW, and ultimately determine whether a shoulder is on-track or off-track, was more reliable and more sensitive, but less specific and less accurate than using 3DCT-based measurements. Interrater and intrarater reliability ranged from fair to good agreement, leading to some concern regarding the utility of the glenoid track concept as a surgical decision-making aid.
Footnotes
Final revision submitted July 11, 2023; accepted August 10, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: I.K.Y.L. has received fellowship support from Smith & Nephew, consulting fees from Smith & Nephew, and royalties from Smith & Nephew, Arthrex, and Wolters Kluwer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Calgary (reference No. REB17-0575).