
Abstract
Background:
Limited data are available on the outcomes and return-to-sport rates after osteochondral allograft transplant in professional athletes.
Purpose:
To evaluate the experience of a single senior surgeon in treating professional athletes with osteochondral allograft transplant, including analyzing clinical outcomes and return to sport.
Study Design:
Case series; Level of evidence, 4.
Methods:
The authors performed a retrospective review of professional athletes treated with primary osteochondral allograft to the knee between January 1, 2001, and January 1, 2021, by a single surgeon. Athletes were required to play at the professional level in their sport and have a minimum of 2 years of follow-up. Return-to-sport rates and timing were evaluated. Patient-reported outcomes were assessed preoperatively and at final follow-up. Reoperations and failures were also tabulated.
Results:
The study included 15 professional athletes who represented a variety of sports, with follow-up at a mean of 4.91 ± 2.2 years (range, 2.0-9.4 years). The majority (8 athletes; 53%) had undergone prior surgeries to the operative knee. Eleven (73%) returned to sport at a mean of 1.22 ± 0.4 years (range, 0.75-2 years), and of the 8 undergoing isolated osteochondral allograft, 7 (87.5%) returned at 1.28 ± 0.3 years. Ten athletes (66.7% of total; 90.9% of those who returned) returned to sport at the same level or higher compared with before surgery. Significant improvements were seen in each assessed patient-reported outcome score at final follow-up. Two of the 3 (66.7%) patients who underwent concomitant meniscal allograft transplant were able to return to sport at the same level or higher than presurgery. Three (20%) underwent second-look arthroscopy, 1 (6.7%) of whom underwent cartilage debridement of the osteochondral allograft.
Conclusion:
Osteochondral allograft transplant in professional athletes can result in a high rate of return to play at a similar or higher level as presurgery, even when performed with concomitant procedures such as meniscal allograft transplant. High-level athletes should expect significant postoperative improvement in clinical outcomes.
Keywords
Articular cartilage injuries pose problems to patients who have high demands on their knees, causing pain and swelling that limit their ability to partake in high-level athletics. The incidence of articular cartilage injuries in the knee may be higher in athletes than nonathletes.9,15,18,21,26,30 Damage to articular cartilage is particularly challenging to manage given its limited healing potential.
Smaller lesions may be managed with at least good short-term relief through debridement, chondroplasty, or bone marrow stimulation. However, in high-level athletes, microfracture has one of the poorest return-to-play results in the literature relative to other orthopaedic surgeries.1,25 For instance, basketball players in the National Basketball Association (NBA) have return-to-play rates of 66.7% to 82.4% after microfracture in the knee. 1 Furthermore, chondroplasty and marrow stimulation are not well suited for larger defects or defects that have undergone prior treatment. Although osteochondral autograft transfer remains a viable option for certain lesions and provides high rates of return to sport, concerns exist with regard to donor site morbidity and management of large-sized defects. 24 In contrast, autologous chondrocyte implant, although appropriate for larger defect areas, has worse outcomes after prior marrow stimulation and is not well-suited for deeper osteochondral defects or for those with subchondral change. 5
Osteochondral allograft transplant is a facile solution to treat deep and large osteochondral lesions, typically at least 2 cm2 in surface area. By fitting an allograft osteochondral plug in a congruent fashion to the patient’s articular surface, osteochondral allograft transplant provides a viable option for defects with extensive subchondral edema, even in the setting of prior marrow stimulation, without donor site morbidity. Current literature demonstrates that expected return-to-sport rates in athletes of all levels ranges from approximately 68% to 80%.3,6,17,22,27 One meta-analysis demonstrated a return-to-sport time of 9.6 ± 3.0 months. 16 Despite these reassuring outcomes of osteochondral allograft transplant in the general athletic population, few data exist on the success of return to high-level, professional athletics. Professional athletes have high demand and impact requirements on their knees. In the active-duty military population, another high-demand group, outcomes for return are rather poor, with 1 study demonstrating 42.1% of patients unable to return to military activity postoperatively. 29 An understanding of how osteochondral allograft transplant fares in the professional athlete population is important for performance expectations and career longevity. Notably, however, return-to-sport literature must be interpreted with some degree of caution given the many independent variables, beyond the treatment of the articular cartilage defect itself, that are influential determinants related to returning an athlete to his or her preinjury status.20,31
The purpose of this study was to evaluate the experience of the senior author (B.J.C.) in treating professional athletes by means of osteochondral allograft transplant, including analyzing clinical outcomes and return to sport. We hypothesized that athletes would have improved outcomes after surgery with a high rate of return to sport at a similar or higher performance level compared with before surgery.
Methods
Patient Population and Data Collection
In this retrospective review, a database of prospectively collected data from a single institution was queried for patients who underwent primary osteochondral allograft transplant of the knee for articular cartilage defects between January 1, 2001, and January 1, 2021. The study protocol received institutional review board approval. Patients were included regardless of the presence of concomitant procedures at the time of osteochondral allograft transplant. Inclusion criteria were as follows: (1) the patient must be a professional athlete in the respective sport, and (2) patients were required to have minimum 2-year follow-up. Patients were evaluated for return-to-sport level and ability, return-to-sport timing, patient-reported outcome measures (PROs), complications, reoperations, and failures.
Return to sport was defined as the time from initial surgery to first preseason or regular season game or first professional debut in which the professional athlete appeared. Additionally, information was obtained from the athletes regarding whether they believed that they returned to a lower level, the same level, or a higher level of play compared with their preoperative performance, as has been done in prior studies.12,19,22 International Knee Documentation Committee subjective score, Lysholm score, and Knee injury and Osteoarthritis Outcome Score subscale surveys were completed preoperatively and at minimum 2-year follow-up. Reoperation was defined as subsequent surgical intervention of the transplanted osteochondral allograft, including second-look arthroscopy for graft evaluation, debridement, and/or loose body removal. Failure was defined as revision cartilage procedure, graft delamination on second-look arthroscopy, or conversion to unicompartmental knee arthroplasty or total knee arthroplasty.
Surgical Technique
All osteochondral allograft transplant procedures were performed by the senior author (B.J.C.), a fellowship-trained orthopaedic surgeon with a high-volume referral-based practice in cartilage restoration. Staging arthroscopy is sometimes performed to assess the extent and location of symptomatic cartilage disease and the presence of concomitant ligamentous or meniscal injury before ordering fresh osteochondral allograft. Allografts were accepted based on osteochondral allograft availability and patient surgical scheduling logistics. For all steps that entailed reaming or graft cutting with powered instruments, copious irrigation was used during those steps to avoid thermal necrosis of the graft or recipient site.
In brief, patients were under general anesthesia and were positioned supine on the operating table. After an examination under anesthesia, diagnostic arthroscopic surgery was performed to visually confirm the osteochondral defects and identify any other existing abnormalities. Concomitant procedures such as meniscectomy, meniscal allograft transplant, osteotomy, or ligament reconstruction were performed first to prevent any iatrogenic injury to the newly restored articular cartilage. Fresh (15-28 days after harvest) osteochondral allografts (JRF Ortho) of the distal femur or patella were gradually rewarmed to room temperature in saline on the back table. A lateral parapatellar arthrotomy with soft tissue lengthening or a limited, medial vastus–sparing arthrotomy was performed for exposure. For patellar defects, a lateral approach was used, and the patella was everted. A cannulated cylindrical sizing guide was placed over the defect to determine the diameter of donor allograft necessary for defect coverage. A guide pin was inserted through the cannulated sizing guide in the center of the defect. The sizing guide was removed, and a cannulated bone reamer was placed over the guide pin to ream to a total depth of 5 to 8 mm including the cartilage surface. The reamer and guide pin were removed, and a small ruler was used to measure the depth of the 4 quadrants (3, 6, 9, and 12 o’clock) for congruent size matching.
On the back table, the donor allograft was prepared, and a bushing was firmly held by an assistant over the desired harvest location. A donor harvester was used to create an allograft cylinder that matched the reamed diameter. Graft measurements were marked on the donor plug, and the donor allograft was trimmed to the appropriate depth using an oscillating saw, rasp, and rongeurs. Pulsatile lavage with bacitracin-mixed saline was used for 2 minutes over the donor plug to reduce marrow elements and immunogenicity. Pressurized carbon dioxide was used after pulsed lavage to further remove marrow elements and improve porosity. In some cases, an orthobiologic substance such as bone marrow aspirate concentrate (BMAC) or platelet-rich plasma (PRP) was added to the bone plug before implantation to enhance biologic potential. Although use of an orthobiologic adjunct (BMAC or PRP) is now routine in the senior surgeon’s current practice for its potential to improve allograft integration, the time point for initial patient enrollment corresponds to a period when orthobiologics were not readily available or used. The donor plug was then press fit by hand, with care to ensure that the 12-o’clock positions on the graft and recipient site were matched. An oversized tamp was used to assist, if necessary, in gently impacting the plug flush to the surrounding articular surface. After graft implant and copious irrigation, layered wound closure was performed and a hinged knee brace was applied.
Rehabilitation Protocol
For patients undergoing isolated osteochondral allograft transplant of the medial or lateral femoral condyles, heel-touch weightbearing began between postoperative weeks 0 and 6. For postoperative weeks 0 to 2, patients wore a brace that was locked in extension full time when not performing exercises. Exercises consisted of quadriceps sets, patellar mobilization, calf pumps, and straight leg raises. When not bearing weight, knee flexion was limited to 0° to 90°. Patients progressed to full weightbearing as tolerated during weeks 6 to 8 postoperatively. For patients undergoing osteochondral allograft transplant of the patellofemoral joint, weightbearing as tolerated in full extension was allowed early in the postoperative period as long as a concomitant procedure did not dictate otherwise (ie, osteotomy). Closed-chain exercises were introduced gradually. After 12 weeks, elliptical bicycling and swimming were encouraged. At 6 to 12 months, a gradual return to functional activities was permitted. Patients were cleared by the attending physician to resume full activity by 8 months postoperatively. Additional adjustments were made to the rehabilitation protocol based on concomitant procedures performed.
Statistical Analyses
Statistical analyses were performed using RStudio Version 4.2.0 (Posit, PBC). Descriptive statistics for continuous variables were reported as means with standard deviations, whereas binomial variables were presented as frequencies and proportions. Shapiro-Wilk testing was used to assess normality of data, and Mann-Whitney U test or independent-samples t test was used accordingly to compare preoperative versus postoperative PROs. Kaplan-Meier survival analysis was used to determine survival probabilities. Results were considered statistically significant when P < .05.
Results
Patient Demographics and Lesion Characteristics
Fifteen professional athletes undergoing primary osteochondral allograft transplant were identified during the study period. All 15 athletes (87% male) met study inclusion criteria, including minimum follow-up, and were followed for a mean of 4.91 ± 2.2 years (range, 2.0-9.4 years) (Table 1). These professional athletes had a mean age of 25.6 ± 4.4 years at the time of surgery. Five athletes (33.3%) had an articular cartilage defect on the medial femoral condyle (mean size, 398 ± 79 mm2), 4 (26.7%) on the lateral femoral condyle (mean size, 361 ± 181 mm2), 4 (26.7%) on the trochlea (mean size, 450 ± 211 mm2), and 2 (13.3%) on the patella (mean size, 362 ± 54 mm2) (Table 1).
Demographics and Intraoperative Variables of Patients Included in Analysis
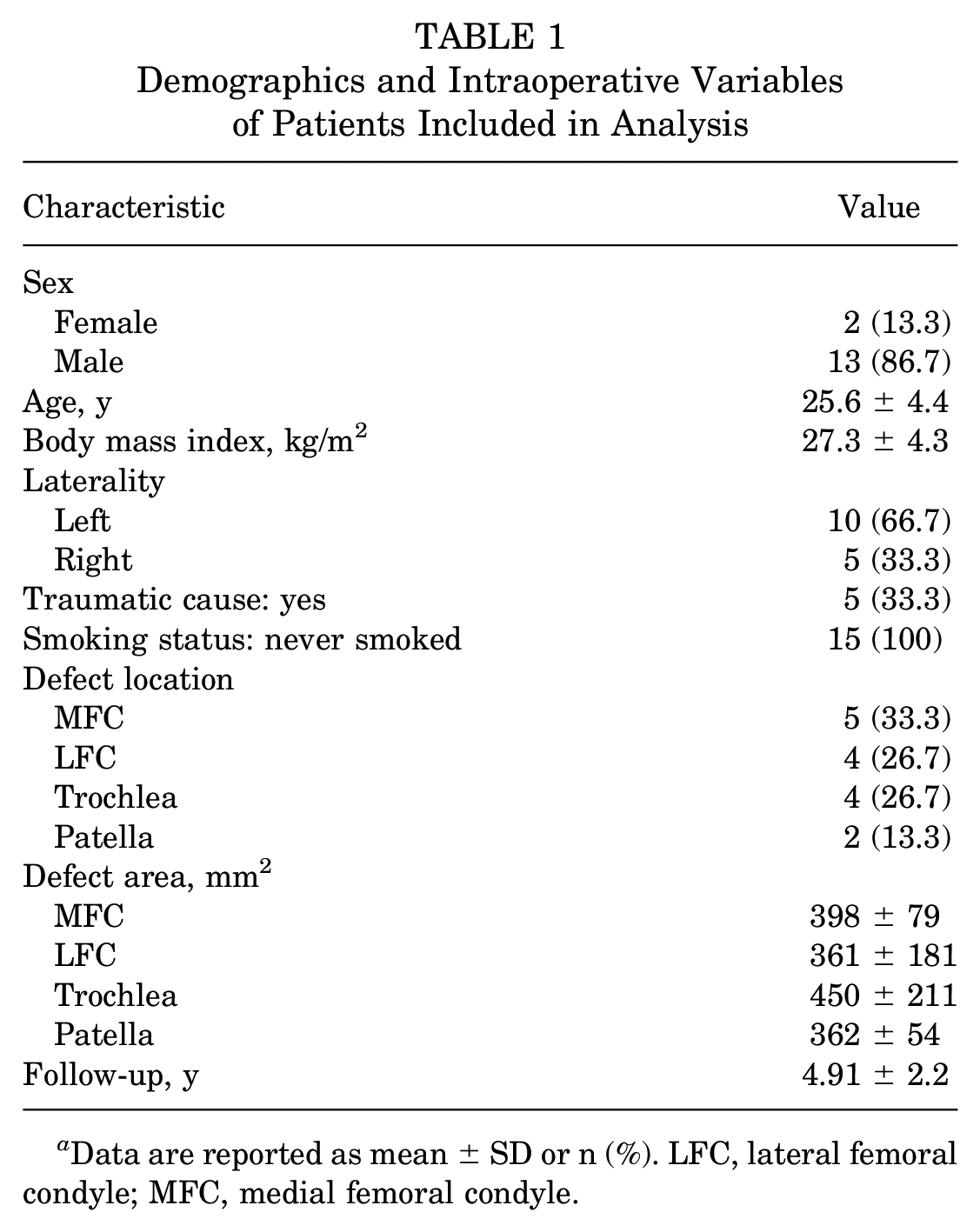
Data are reported as mean ± SD or n (%). LFC, lateral femoral condyle; MFC, medial femoral condyle.
Athletes’ Professional Association and Position Played
A variety of professional leagues were represented in this cohort, including Major League Baseball (MLB), Minor League Baseball (MiLB), National Football League (NFL), National Hockey League (NHL), Major League Soccer, and other professional-level athletics (Table 2).
Sport and Position of the Included Athletes a

Dashes indicate position was not provided.
Previous and Concomitant Procedures
Eight patients (53%) had prior surgeries (Table 3). A total of 9 concomitant procedures in 7 patients were performed at the time of osteochondral allograft transplant. Five patients received adjunctive BMAC, and 1 received PRP (Table 3).
Previous and Concomitant Procedures a

Data are shown as n (%) or n unless otherwise indicated. ACL, anterior cruciate ligament; BMAC, bone marrow aspirate concentrate; DFO, distal femoral osteotomy; HTO, high tibial osteotomy; LMAT, lateral meniscal allograft transplant; MPFL, medial patellofemoral ligament; PRP, platelet-rich plasma.
A major concomitant procedure was defined as any of the listed procedures apart from adjunct use of orthobiologic substances (eg, BMAC or PRP).
Return to Sport
Eleven athletes (73%) returned to sport at a mean of 1.22 ± 0.4 years (range, 0.75-2 years) (Table 4). Seven athletes (87.5%) with an isolated osteochondral allograft procedure returned to sport at a mean of 1.28 ± 0.3 years after the initial procedure. Of those who returned to sport, 2 athletes had a concomitant meniscal transplant and 2 had a concomitant osteotomy. The 2 athletes who underwent concomitant lateral meniscal allograft transplant returned to sport at 0.75 years and 1 year after their initial surgery, both at a higher level of play. One athlete with concomitant high tibial osteotomy, lateral meniscectomy, and medial meniscectomy returned to sport at the same level of play at 0.83 years. One athlete with concomitant distal femoral osteotomy returned to sport at 1.75 years at a higher level of play. Four athletes who did not return to sport were an NFL tight end, an NFL defensive end, an NHL defenseman, and a professional volleyball player. Lesion characteristics, prior surgeries, and concomitant procedures of this group are noted in Table 5.
Return-to-Sport Rate (n = 15 Athletes) a
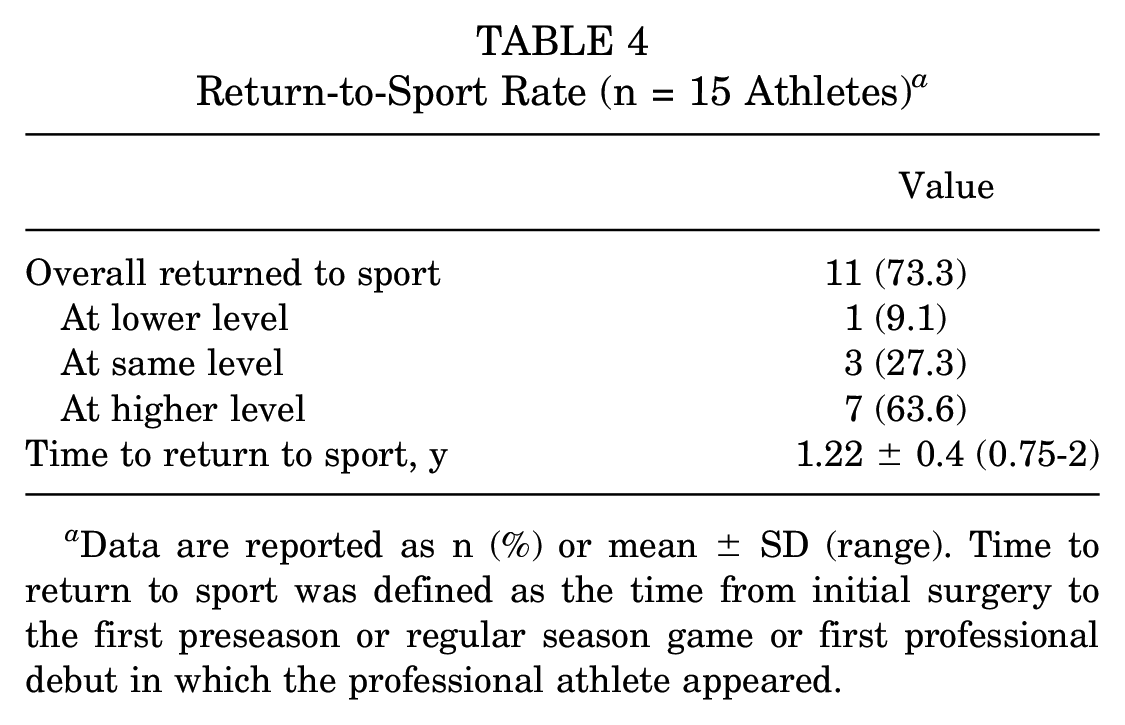
Data are reported as n (%) or mean ± SD (range). Time to return to sport was defined as the time from initial surgery to the first preseason or regular season game or first professional debut in which the professional athlete appeared.
Lesion Characteristics, Prior Surgeries, and Concomitant Procedures in the Athletes Who Did Not Return to Sport a

HTO, high tibial osteotomy; LFC, lateral femoral condyle; LMAT, lateral meniscal allograft transplant; MFC, medial femoral condyle; NFL, National Football League; NHL, National Hockey League.
Patient-Reported Outcome Scores
All 15 athletes had preoperative and postoperative PROs available for analyses. Patients demonstrated statistically significant postoperative improvements at the most recent time point for all PROs (P < .01) (Figure 1).

Mean patient-reported outcome measure scores after primary osteochondral allograft transplant of the knee in professional athletes. *Significant improvement from preoperative to postoperative (P < .01). ADL, activities of daily living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, quality of life; Sport, sport and recreation; Sx, symptoms.
Complications, Reoperations, and Failures
At final follow-up, 3 patients (20%) had undergone repeat osteochondral allograft–associated intervention (second-look arthroscopy for graft evaluation due to persistent symptoms) at a mean of 1.90 ± 2.3 years after initial surgery. One MLB athlete underwent microfracture for a new 20 × 8–mm trochlear cartilage defect, separate from the intact, well-incorporated primary trochlear osteochondral allograft. One MiLB athlete was found to have a macroscopically well-integrated and healing graft. No further treatment was necessary at his most-recent follow-up at 3.27 years. Finally, 1 NFL athlete had 50% graft delamination during second-look arthroscopy. This was the only noted failure (6.7%) among this cohort. He was treated with articular cartilage debridement/chondroplasty with a planned revision medial femoral condyle osteochondral allograft and medial meniscal transplant if symptoms persisted. This athlete retired from play and has not undergone revision surgery. No intraoperative or postoperative complications were encountered in any athlete included in this cohort.
Discussion
The primary finding of the present study was that the majority of professional athletes undergoing osteochondral allograft transplant were able to return to sport at a similar or higher level than before surgery. Patients in a variety of sports can play again at the highest levels with a low rate of revision surgery on the primary graft site. Clinical outcomes are expected to substantially improve after this procedure, whether in isolation or combined with other procedures. This study presents one of the largest long-term series on outcomes after osteochondral allograft transplant in the professional athlete population.
The overall return-to-sport rate was 73.3%. This overall rate is similar to the rate of 77% found in a prior study on isolated femoral condyle osteochondral allografts in competitive high school and collegiate athletes 22 and similar to the rate of 75% in a study evaluating 4 NBA athletes. 3 In the present study, when we evaluated patients with isolated primary osteochondral allografts separately, the return-to-sport rate was even higher at 87.5% (7/8 athletes), compared with 57.1% (4/7 athletes) in the group undergoing concomitant procedures. This finding suggests that concomitant procedures to offload forces on the defect site, such as high tibial osteotomies, distal femoral osteotomies, and meniscal allograft transplant, may possibly contribute to worse return-to-play rates in professional athletes than those undergoing isolated cartilage treatment, but the numbers in the present study are small and it is difficult to draw definitive conclusions. However, 2 athletes with concomitant meniscal allograft transplant successfully returned to sport after their procedure without a retear of their meniscal allograft. It is possible that professional athletes or those at the highest levels may have greater challenge returning after these concomitant procedures compared with recreational athletes. For instance, a systematic review on patients undergoing high tibial osteotomy found an overall return-to-sport rate of 87.2%, with 78.6% returning to the same or higher level; however, when the authors of that review isolated competitive athletes, only 54% returned to competition. 8 In the present study, 66.7% of athletes (90.9% of those who returned) were able to return to an equivalent or higher level of sport postoperatively. Ultimately, the return-to-sport rates of 73.3% overall and 87.5% for isolated primary osteochondral allografts in the present study’s professional athletes are not dissimilar to data in the NBA for players undergoing microfracture (66.7%-82.4% return-to-play rate), but the indications for osteochondral allografts tend to be for larger and more severe lesions. Furthermore, it is likely that the durability of osteochondral allograft transplant is greater in long-term follow-up.2,14
The return-to-sport time in these professional athletes averaged just over 1 year. This time period is longer than that found in a meta-analysis by Krych et al, 16 demonstrating a mean return-to-sport time of 9.6 ± 3.0 months. Another study found that in professional basketball players undergoing osteochondral allograft transplant, the return-to-play time was a median of 20 months postoperatively (range, 10-26 months), whereas a collegiate basketball cohort had a median return-to-play time of 8 months postoperatively. 3 It is possible that the timing for athletes to return at the highest levels is longer. However, several factors may further contribute to the discrepancies between professional and nonprofessional athletes. These factors include that professional athletes’ decisions may be attributable to ongoing contractual negotiations, and professional athletes may need to make decisions based on earning potential with additional considerations for career longevity, sport-specific demands that contribute to varied ability and timing for return to sport, and decisions about in- versus off-season return for strategic or other factors.13,20,31 Moreover, the small number of professional athletes with these injuries are subject to coaching decisions, match-ups, and availability of other players, all of which affect their timing for return. 20
Clinical outcomes significantly improved in each PRO measured postoperatively at final follow-up. Based on the data and PROs evaluated, patients can continue to expect improvement in daily activities, quality of life, and pain, in addition to sport-specific metrics. Professional athletes, therefore, see benefits and improvements that would be expected of nonathlete and recreational athlete populations.10,23 The mean improvements in each PRO assessed were well above established levels of minimal clinically important difference. 28
Importantly, the rate of reoperation for the osteochondral allograft specifically was 20% at 1.90 ± 2.3 years postoperatively, and all of these reoperations were second-look arthroscopies due to return of symptoms. Compared with other data suggesting reoperation rates of 34% to 53%, 7 the data from the present study are reassuring. Furthermore, there was only 1 intervention on the primary osteochondral allograft itself (6.6%), which was an articular cartilage debridement/chondroplasty. This rate is similar to that found by Nielsen et al 27 in a cohort of mixed-level athletes, where 9.4% experienced allograft failure. The mean follow-up in the present study was almost 5 years. It is known, however, that more reoperations, including simple knee arthroscopies, are expected with time after this procedure, and patients should be counseled of this possibility.2,11 More than half of the patients had prior surgery on their knee before the osteochondral allograft procedure. This is not uncommon, given that osteochondral allografts are frequently a second procedure with staging at the first arthroscopic procedure, although an increased number of prior surgeries may be associated with risk of failure.3,10,17,22
Limitations
The present investigation has several limitations. The data presented are from a single surgeon in the specific population of high-level athletes, and therefore the outcomes presented may not be applicable in other settings. The professional athlete cohort itself is heterogeneous, representing different sports and leagues. Moreover, many of the patients had concomitant procedures along with the osteochondral allograft transplant, which, although common in the setting of large osteochondral defects, may bias or influence outcomes and return-to-play metrics and limit the conclusions that may be drawn. Although the series is large for this specific population with midterm follow-up, overall the small numbers per group limit the ability to perform subanalyses such as comparisons by sport type, player position, defect size, and defect location. Furthermore, other confounding factors may influence results, such as patient age, sex, cause of injury, presurgical symptom duration, and prior surgeries, among others.4,10,17,27 The level of return to play was subjective as determined by the athlete and not based on performance metrics. Additionally, as previously reported, a number of variables are relevant in the decision-making related to the ultimate return of a professional athlete to play that extend far beyond clinical results.20,31 Finally, long-term follow-up is lacking, and the longevity of the osteochondral allografts in the professional athlete population is unknown.
Conclusion
Osteochondral allograft transplant in professional athletes can result in a high rate of return to play at a similar or higher level even when performed with concomitant procedures such as meniscal allograft transplant. High-level athletes should expect significant improvement in clinical outcomes after osteochondral allograft transplant. This finding is useful for patient counseling and discussing expectations for return to sport in professional athletes.
Footnotes
Final revision submitted August 11, 2023; accepted August 21, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.A. has received education payments from Smith & Nephew. R.Q. has received honoraria from Encore Medical and hospitality payments from Stryker. B.J.C. has received research support from Aesculap, Arthrex, JRF Ortho, and Operative Techniques in Sports Medicine; education payments from Endo Pharmaceuticals and Medwest Associates; consulting fees from Acumed, Aesculap Biologics, Arthrex, Bioventus, DJO, Vericel, Ossio, Pacira Pharmaceuticals, Endo Pharmaceuticals, and Flexion Therapeutics; nonconsulting fees from Arthrex, Terumo, Pacira Pharmaceuticals, and Vericel; royalties from Arthrex, Elsevier Publishing, and Operative Techniques in Sports Medicine; honoraria from Vericel; stock options from Bandgrip and Ossio; and hospitality payments from GE Healthcare. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Rush University Medical Center (ref No. 15020601-IRB01).