
Abstract
Background:
A coracoclavicular (CC) fixation technique using an all-suture anchor with the assistance of fluoroscopy can prevent iatrogenic anterior deltoid detachment from the clavicle; however, soft anchor pullout has been reported as a complication.
Purpose:
To compare the biomechanical properties of conventional metallic and all-suture anchors for CC suture fixation.
Study Design:
Controlled laboratory study.
Methods:
A total of 24 fresh-frozen cadaveric specimens were divided into 2 groups: metal anchor group (group M) and all-suture anchor group (group A). In group M, 5.0-mm metallic suture anchors were used for CC fixation, whereas 2.8-mm all-suture anchors were used in group A. The prepared specimens were mounted on a materials testing machine. After preconditioning at 0 to 20 N for 10 cycles, the specimens were subjected to cyclic loading from 20 to 70 N for 1000 cycles. Finally, all the specimens were loaded to failure. Cyclic elongation, linear stiffness, ultimate load, and failure modes were recorded, and the Mann-Whitney U test was used to compare nonparametric parameters between the 2 groups.
Results:
All of the specimens completed the cyclic loading test. The elongation after cyclic loading in group M (1.6 ± 0.6 mm) was significantly smaller compared with that in group A (2.5 ± 1.2 mm) (P = .02). No between-group differences were found in linear stiffness (42 ± 17 N/mm in group M and 41 ± 17 N/mm in group A). The ultimate failure load in group M (263 ± 66 N) was significantly greater than that in group A (177 ± 76 N) (P = .02). All specimens failed because of suture anchor pullout.
Conclusion:
The use of all-suture anchors in CC fixation resulted in significantly greater cyclic displacement and smaller ultimate failure load than that of metallic anchors.
Clinical Relevance:
Understanding the most biomechanically sound suture anchor may assist in lowering the risk of clinical failure in CC fixation and repair.
The coracoclavicular (CC) ligaments (conoid and trapezoid ligaments) and acromioclavicular (AC) ligaments are important stabilizers of the AC joint. 4 Numerous treatments have been proposed for treating acute AC joint dislocation, including hook plate fixation and reconstruction of the CC ligament using autogenous or synthetic ligaments. 7 When a hook plate is chosen for treating acute AC joint dislocation, additional suture fixation contributes to decreased subacromial osteolysis, less postoperative pain, and better short-term functional outcomes. 1
In addition, restoring the function of the CC ligament is an important issue in treating distal clavicle fractures.5,14 A systematic review indicated that locking compression plate with CC augmentation was the best internal fixation method for treating unstable distal clavicle fractures. 14 Wu et al 13 compared hook plate fixation for treating distal clavicle fractures with and without CC suture fixation and found that hook plate fixation with suture anchor fixation provided better functional outcomes than hook plate fixation alone.
As the CC suture fixation has become a common procedure, iatrogenic anterior deltoid injury has started to attract attention. 8 Iatrogenic anterior deltoid detachment from the clavicle is usually necessary to accurately insert the conventional suture anchor or loop sutures beneath the coracoid process. 8 To avoid iatrogenic deltoid detachment, Seo et al 8 proposed a CC fixation technique using an all-suture anchor with the assistance of fluoroscopy and observed that this technique avoided the iatrogenic postoperative deltoid atrophy. In their technique, a drill guide was used for identifying the anchor insertion site under fluoroscopy, and the all-suture anchor was then inserted through the drill guide after drilling. 8 On the other hand, potential complications caused by other implants that require bone tunnels with a relatively large diameter are a clinical concern. 12 To overcome this complication risk, Jeong et al 3 proposed a unique arthroscopic CC fixation technique using multiple all-suture anchors. The all-suture anchors were advocated as small-width tunnels reduced the risk of fracture.
Although the CC fixation technique using all-suture anchors features clinical advantages, soft anchor pullout has also been reported, 8 leading to a concern about whether the all-suture anchor provides biomechanical properties comparable with those of conventional anchors. Therefore, in this study, we aimed to compare the biomechanical properties of conventional metallic and all-suture anchors in CC suture fixation. We hypothesized that the all-suture anchor would have greater cyclic elongation and a smaller ultimate pullout strength compared with conventional metallic anchors.
Methods
Experimental Specimens
A total of 24 fresh-frozen cadaveric shoulder specimens (mean age, 67 ± 7 years) were obtained from the MedCure Foundation. The specimens were stored at -20°C and thawed at room temperature (22°C) for at least 24 hours before the biomechanical experiment. Bone mineral density was obtained with dual-energy X-ray absorptiometry (Lunar Prodigy; GE HealthCare). The soft tissue around the shoulder was removed carefully, leaving the scapula bone alone. With a random number table, the specimens were divided randomly into 2 groups: a metallic anchor group (group M) and an all-suture anchor group (group A). In group M, a 5.0-mm metallic suture anchor (Super Revo; ConMed) with double-loaded No. 2 braided sutures was inserted in the coracoid base, whereas a 2.8-mm all-suture anchor (Y-Knot RC; ConMed), with triple-loaded No. 2 braided sutures, was inserted after predrilling in group A. These anchors were selected according to previous clinical studies.8,9 The depth of the all-suture anchor insertion was determined as when the most distal laser line falls below the cortical layer, in accordance with manufacturing instructions. In all specimens, the locations of the soft anchors were inferior to the coracoid.
Biomechanical Testing Setup
Each scapular specimen was mounted on a universal materials testing system (AG-X; Shimadzu) using a custom-made clamp (Figure 1). The suture ends of the anchors were tied together on the adapter of the material testing machine. The distance between the inferior border of the adapter and superior cortex of the coracoid bone was standardized in accordance with a previous biomechanical study 10 : 10 mm in the superior-inferior direction and 6 mm in the anterior-posterior direction, resulting in a spatial distance of 12 mm.

The biomechanical setup. Each specimen was mounted on a universal materials testing system. The suture ends of the anchors were tied together on the adapter of the materials testing machine. The distance between the inferior border of the adapter and superior cortex of the coracoid bone was standardized: 10 mm in the superior-inferior direction and 6 mm in the anterior-posterior direction, resulting in a spatial distance of 12 mm.
Biomechanical Testing Protocol
The biomechanical testing protocol was in accordance with a previous study. 10 First, each specimen was preconditioned from 0 to 20 N for 10 cycles to eliminate the creep phenomenon at a crosshead speed of 1 mm/s. After preconditioning, the specimens were loaded cyclically from 20 to 70 N for 1000 cycles at a crosshead speed of 1 mm/s. The range of load in cyclic loading test was selected as it fit at least 10% of the ultimate load and covered physiological loading in a light postoperative rehabilitation program. 10 The cyclic elongation was defined as the difference in elongation recovery from the 1000th loading to the length of the complex after the first cycle. 10 After cyclic loading, each specimen was loaded to failure with a crosshead speed of 50 mm/min. Linear stiffness, ultimate load, and failure modes were recorded after the load-to-failure test.
Statistical Analysis
The required sample size for the current study was calculated based on a pilot study with 8 specimens assigned randomly to 2 groups (group M and group A) using G*Power Version 3.1.9.7 software (Heinrich Heine-University of Dusseldorf). An α equal to .05 and a power (1 - β) of 0.80 were used in the Wilcoxon-Mann-Whitney test model. After imputing the means and standard deviations of the 2 pilot study groups, an effect size of 1.08 was obtained. Accordingly, a sample size of 24 specimens with 12 in each group was determined to be appropriate.
Statistical comparisons were performed using SPSS Statistics software Version 22 (IBM SPSS Inc). Descriptive statistics, including mean and standard deviation, were calculated for each group. The Mann-Whitney U test was used to compare nonparametric parameters between the 2 groups. Statistical significance was set at P < .05.
Results
A total of 24 cadaveric shoulder specimens were enrolled and divided into 2 groups of 12 specimens each. The bone marrow density in group M (0.84 ± 0.13 g/cm2) and group A (0.85 ± 0.12 g/cm2) were not significantly different (P = .93). All the specimens completed the cyclic loading protocol for biomechanical testing. The elongation after cyclic loading in group M (1.6 ± 0.6 mm) was significantly smaller compared with that in group A (2.5 ± 1.2 mm) (P = .02). No statistically significant difference was found in linear stiffness between group M (42 ± 17 N/mm) and group A (41 ± 17 N/mm) (P = .80). The ultimate failure load in group M (263 ± 66 N) was significantly greater than that in group A (177 ± 76 N) (P = .02). All specimens failed because of the anchor pullout from the coracoid process. The load-elongation curves are illustrated in Figure 2. The curve in group A indicates the bicortical fixation of the all-suture anchor.
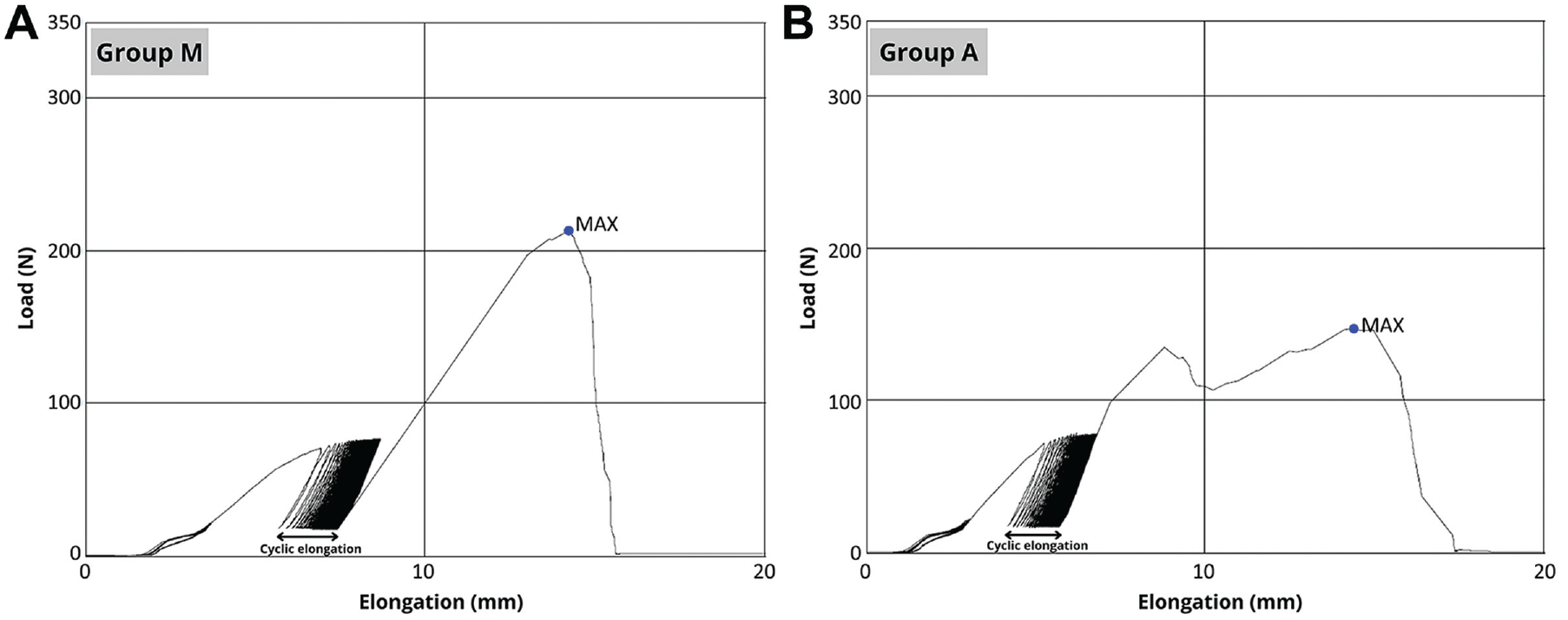
Load elongation curves in (A) the metallic anchor group (group M) and (B) the all-suture anchor group (group A). The curve in group A indicates the bicortical fixation of the all-suture anchor. MAX, maximal load.
Discussion
The major finding of the current study was that the use of metallic anchors in CC fixation resulted in significantly smaller cyclic displacement (1.6 ± 0.6 mm) and greater ultimate failure load (263 ± 66 N) than that of all-suture anchors (2.5 ± 1.2 mm and 177 ± 76 N, respectively). CC fixation is not only an important additional augmentation for treating acute AC joint dislocation using a hook plate 1 but also vital for treating distal clavicle fractures using either a locking compression plate or a hook plate.13,14 As iatrogenic anterior deltoid detachment from the clavicle is usually required using the methods currently available for CC fixation, Seo et al 8 proposed a novel technique using an all-suture anchor without additional deltoid detachment and reported no deltoid atrophy at 1-year follow-up. The present study further investigated the all-suture anchor pull-out strength in a CC-fixation model, the results of which suggested that one should be cautious when selecting this technique as it provided inferior biomechanical properties compared with those with a metallic anchor.
The cyclic loading test is commonly used in biomechanical testing to simulate rehabilitation activities. 11 In this study, the cyclic testing protocol was set from 20 to 70 N for 1000 cycles, fitting at least 10% of the ultimate load and covering a physiological load situation in a light postoperative rehabilitation program. 10 Hence, the elongation of the sutures after cyclic loading represented the loosening of a repaired construct during early rehabilitation, increasing the potential clinical failure risk. This study employed triple-loaded all-suture anchors and double-loaded metallic anchors for biomechanical testing according to previously published clinical studies.8,9 Although anchors in group A contained more sutures than those in group M, the cyclic elongation in group A was significantly greater, suggesting that the anchor-bone interface may be the major contributor to this phenomenon. Therefore, careful consideration of the aforementioned biomechanical findings is required when using an all-suture anchor for CC fixation.
The all-suture anchor achieved anchor-bone fixation by implementing the anchor against the cortical bone. 6 The maximum pullout force of an all-suture anchor was correlated significantly with the thickness of the cortex rather than the cancellous bone mineral density measured at the implantation site. 6 The load-elongation curve in the present study revealed that bicortical fixation was achieved using the all-suture anchor fixation technique. However, all-suture anchor pullout could still be observed during surgery, leading to a clinical concern. 8 The findings of the load-to-failure tests in the present study could confirm the aforementioned clinical findings that the all-suture anchors had relatively smaller pullout strength. 8 Based on these biomechanical findings, the use of all-suture anchors in CC fixation was not suggested, in consideration of the anchor pullout risk. In addition, medical expenses also imposed an issue because an all-suture anchor is costlier (US$1000) than a metallic suture anchor (US$170). 2
Although findings from different studies cannot be compared directly, the biomechanical testing results in the current study are generally compatible with those in a previous study. 10 Wellmann et al 10 reported that the elongation after cyclic loading was 1.69 ± 0.74 mm for the 5.0-mm Twinfix anchor. In this study, a similar cyclic elongation was found in group M (1.6 ± 0.6 mm), in which another 5.0-mm anchor was used. Regarding the ultimate loads during tensile testing, Wellmann et al 10 reported an ultimate failure load of 295 ± 83 N for the 3.5-mm Twinfix anchor and 331 ± 61 N for the 5.0-mm Twinfix anchor. Similarly, in our study, the ultimate failure load in group M was 263 ± 66 N.
Limitations
The present study has some limitations. First, this biomechanical study was an in vitro study. Although the testing protocol was set to simulate physiological loading, 10 care should still be taken when interpreting the results for clinical use. Second, the sample size of cadaveric samples in both groups was relatively small, and individual differences in cadavers potentially affected the testing results. To ensure sufficient power in the statistical analysis, an a priori power analysis was conducted to calculate the required sample size. Third, the clavicle was not used in this study. To decrease the influence of the clamp stability on the clavicle, we used an adapter connected to the materials-testing machine. By setting the adapter to the position where the clavicular footprint of the CC was, 10 the moving of the adapter in biomechanical testing could simulate clavicular movements. However, the rotation effects from the clavicle during overhead motion could not be simulated.
Conclusion
The use of all-suture anchors in CC fixation resulted in significantly greater cyclic displacement and smaller ultimate failure load than that of metallic anchors. Understanding the most biomechanically sound suture anchor may assist in lowering the risk of clinical failure in CC fixation and repair. Future studies are needed to identify the most appropriate suture anchor for CC fixation.
Footnotes
Final revision submitted June 3, 2023; accepted August 10, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from Skeleton Materials and Bio-compatibility Core Lab, Research Center of Clinical Medicine, National Cheng Kung University Hospital (NCKUH-11204010). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.