
Abstract
Background:
The stability of the glenohumeral joint is associated with anatomic characteristics including bony structures and soft tissues.
Purpose:
To compare the differences in specific bony glenohumeral geometries between shoulders with anterior shoulder instability (ASI), unaffected contralateral shoulders, and healthy control shoulders.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Shoulder computed tomography (CT) scans of 36 patients with ASI and 36 matched healthy controls were retrieved and 3-dimensionally reconstructed. We measured the glenoid radius of curvature (GROC) in the anterior-posterior (AP) and superior-inferior directions, humeral head radius of curvature (HROC) in the AP direction, conformity index, glenoid height, glenoid width, glenoid index, stability angle, glenoid version, and glenoid depth. The differences between the groups were statistically calculated. CT scans of the unaffected contralateral shoulders from 21 of the ASI patients were also collected to identify the consistency of the bony structures in bilateral shoulders.
Results:
Patients with ASI had greater GROC in the AP direction (P < .001), HROC in the AP direction (P = .002), glenoid height (P = .005), and glenoid index (P < .001) and smaller conformity index (P < .001), glenoid width (P = .002), stability angle (P < .001), and glenoid depth (P < .001). In addition, the glenoid of the ASI patients was more anteverted compared with that of controls (P = .001). There was no statistical difference in half the measurements between the bilateral shoulder joints in patients with ASI.
Conclusion:
In this study, glenohumeral geometric differences were found between ASI patients and healthy control participants. Glenoid curvature and conformity index, based on bilateral comparisons of affected and contralateral shoulders, appear inherent and may predict ASI risk.
Keywords
Anterior shoulder instability (ASI) is common in young and physically active workers or athletes. Zacchilli et al 22 estimated an overall incidence of 23.9 cases per 100,000 person-years in the United States. The incidence of ASI may be up to 18 times higher in high-risk populations. 5 Because of its short- and long-term complications and psychological and economic burdens on patients, it would be useful to predict ASI risks and to develop corresponding prevention strategies.
Anatomic structures that affect the stability of the glenohumeral joint include soft tissue (glenoid rim, glenohumeral ligaments, etc) and bony structures (glenoid and humeral head). The role of soft tissue in the stability of the shoulder has been well studied,4,9,17 while attention has been on the skeletal geometries of the glenohumeral joint in recent years. 2 Previous studies have reported significant morphological differences between healthy individuals and patients with shoulder instability; for example, Meyer et al 10 conducted a prognosis study and found that a specific acromial shape, named the steep “Swiss chalet roof-type” acromion, was associated with posterior shoulder instability. A retrospective study by Aygun et al 1 suggested that the glenoid version is a high-risk factor for ASI. Haas et al 7 demonstrated the association of developing instability arthropathy with constitutional glenoid concavity shape. Peltz et al 14 measured various geometric parameters of the shoulder joint using 3-dimensional (3D) reconstruction technology and found that patients with ASI had a significantly greater glenoid height-to-width ratio (ie, glenoid index), flatter articular surface, smaller conformity index, and smaller stability angle in the anterior-posterior (AP) direction.
The purpose of this study was to further determine the differences in the bony glenohumeral morphological features between patients with ASI and matched healthy controls in the Chinese population and to confirm the consistency of the measurements between the affected and unaffected contralateral shoulders of the ASI patients. We hypothesized that ≥1 glenohumeral bony characteristics (glenoid radius of curvature [GROC], humeral head radius of curvature [HROC], conformity index, glenoid height, glenoid width, stability angle, glenoid version, and glenoid depth) would differ between patients with ASI and healthy controls.
Methods
Study Participants
The protocol for this study was approved by the ethics committee of our institution, and informed consent was obtained from all included participants. A total of 48 consecutive adult patients with ASI who were treated in our department between March 2018 and March 2023 were initially enrolled in this study. The inclusion criteria were patients who had experienced ≥1 episode of anterior shoulder dislocation or subluxation. The exclusion criteria were any previous surgical history on the affected shoulder; coexistence of shoulder instability in any other direction; the presence of any other injury, disorder, or disease in the same shoulder; and the unavailability of digital data from shoulder computed tomography (CT).
Of the 48 enrolled patients, 10 patients with incomplete digital data from CT examinations and 2 patients with coexisting posterior shoulder instability were excluded. Thus, 36 patients with ASI (36 shoulders) were included as the ASI group. These shoulders were matched by sex and age with a control group of 36 shoulders without instability or any history of shoulder surgery or trauma, with chest CT scans that included the shoulders, found through our institutional picture archiving and communication system and electronic medical record system. The CT scans of the unaffected contralateral shoulders of 21 of the 36 ASI patients were also collected.
CT Measurements
Data in DICOM (Digital Imaging and Communications in Medicine) format were imported into Mimics Medical software (Version 16.0; Materialise). The scapula and humerus were segmented and reconstructed as 3D bone models. The superior-inferior (SI) axis (12 o'clock to 6 o’clock) of the glenoid and the longest AP axis (9 o'clock to 3 o’clock) perpendicular to the SI axis were identified in the en face view of the 3D glenoid model (Figure 1).

En face view of the 3-dimensional bone model of a left glenoid. The superior-inferior (SI) axis (12 o'clock to 6 o’clock) of the glenoid and the longest anterior-posterior (AP) axis (9 o'clock to 3 o’clock) perpendicular to the SI axis were identified.
The glenoid height and glenoid width were measured respectively between the glenoid surface edges on the SI and AP axes, and the glenoid index was calculated as glenoid height/glenoid width. The length of the glenoid anterior bone defect was measured in all patients. The contralateral glenoid models were mirrored and overlapped with the affected side, and the length of the defect was the difference in glenoid width between the models.
Since any tilt in the slicing direction of the CT may result in inaccuracy in subsequent measurements, 12 standardized axial, sagittal, and coronal images were created with the reslicing tool in the Mimics software program for all the models, using the AP and SI axes as the reference lines. The following parameters were measured in the standardized axial plane. On the image containing the AP axis, the “Measure Diameter” tool in the Mimics program was used to create a best-fit circle that matched the curvature of the glenoid articular surface. The radius of the best-fit circle was defined as the GROC in the AP direction. The same method was used for the humeral head to determine the HROC (Figure 2).
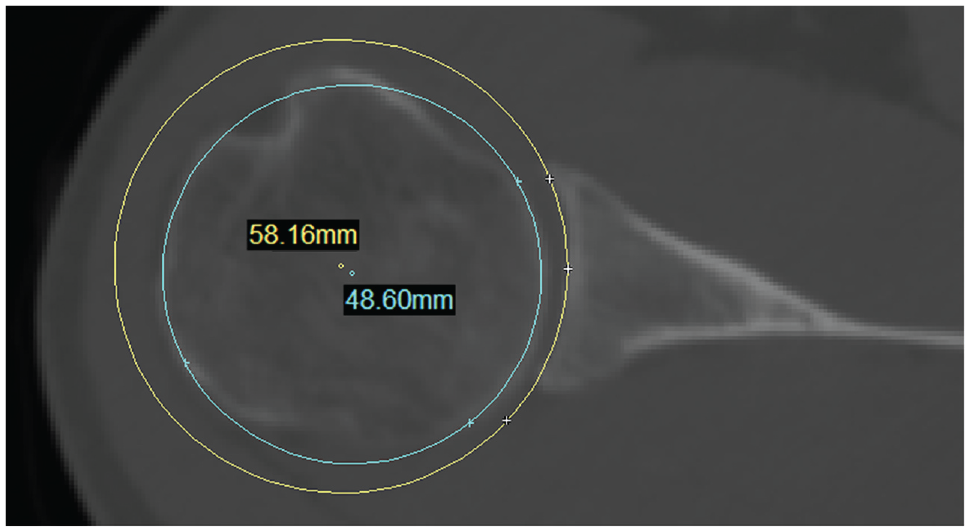
The glenoid radius of curvature (radius of the yellow circle) and humeral head radius of curvature (radius of the blue circle) in the anterior-posterior direction measured using the “Measure Diameter” tool in the Mimics software program on the standardized axial plane of a right shoulder.
The conformity index was calculated as HROC/GROC in the AP direction. The stability angle, also known as the humerus-containing angle, was calculated as the angle enclosed by the line connecting the center and the anterior edge of the glenoid, with the line connecting the center and the posterior edge of the glenoid (Figure 3A). Glenoid version was determined by the tangential line of the glenoid edges and the line connecting the innermost point of the scapula and midpoint of the glenoid concavity (Figure 3B). 3 Glenoid depth was the vertical distance from the deepest point of the glenoid articular surface to the tangential line of the anterior and posterior edges of the glenoid (Figure 3C). GROC in the SI direction was measured in the standardized coronal imaging plane using the same method as in the AP direction.

Measurements on an axial computed tomography plane of a right shoulder. (A) The endpoint of the stability angle (SA) was the center of the best-fit circle of the humeral head. The 2 lines defining the stability angle passed through the anterior and the posterior edges of the glenoid articular surface. (B) The alpha angle (α) was measured between the tangential line of the glenoid edges and the line connecting the innermost point of the scapula and the midpoint of the glenoid concavity. The glenoid version equals α minus 90° (negative value indicates anteversion; positive value indicates retroversion). (C) The glenoid depth (length of the short red line) was the vertical distance from the deepest point of the glenoid articular surface to the tangential line of the edges of the glenoid.
The reconstructions and measurements were performed independently by 2 experienced attending surgeons, each with 5 years of experience in musculoskeletal disorders and radiology (Z.N. and M.L.). Measurements were conducted twice within the space of 1 month, and the intraclass correlation coefficient (ICC) was used to calculate inter- and intraobserver reliability.
Statistical Analysis
Comparisons were made between the ASI and control groups and between the affected and healthy contralateral shoulders of the ASI patients for whom CT scans were available. For continuous variables, the paired t test was used for parametric data; otherwise, the Wilcoxon signed-rank test was used. For categorical variables, the chi-square test was used. Within the ASI group, the correlation between the length of the glenoid bone defects and the glenoid measurements (GROC in the AP direction, glenoid width, glenoid version, stability angle, and glenoid depth), as well as the correlation between the width of the Hill-Sachs lesions and the humeral measurements (HROC in the AP direction), were evaluated utilizing the Pearson correlation coefficient and the Spearman rank-order correlation coefficient, contingent upon the data distribution. All statistical analyses were performed using SPSS Statistics software (Version 25.0; IBM). Statistical significance was set at P < .05.
Results
Characteristics of the Study Groups
Demographic information for the ASI group and matched controls is shown in Table 1. There were no significant differences in age, sex distribution, or side affected between the groups. For the ASI group, additional data were recorded, including the cause of shoulder instability, the duration between the first dislocation event and the CT examination, the number of dislocation/subluxation events, bilateral shoulder instabilities, the length of the glenoid bone defects, and the width of the Hill-Sachs lesions (Table 2).
Comparison of Demographic Data Between the ASI and Control Groups a

Values are presented as n or mean ± SD.
Characteristics of the ASI Group a

Values are presented as n or mean ± SD (range). ASI, anterior shoulder instability; CT, computed tomography.
CT Measurements
The intraobserver ICCs of the CT scan measurements ranged from 0.83 to 0.99, and the interobserver ICCs ranged from 0.82 to 0.99, indicating that both were associated with excellent reliability.
Compared with the control group, the ASI group had greater GROC in the AP direction, HROC in the AP direction, glenoid height, and glenoid index, as well as a smaller conformity index, glenoid width, stability angle, and glenoid depth in their affected shoulders. Of the shoulders with ASI, 52.78% were associated with an anteverted glenoid, and only 19.44% of control shoulders had an anterior glenoid version. There was no significant difference in GROC in the SI direction between the ASI and control groups (Table 3). In the comparison of the bilateral shoulders of the ASI group, significant differences were only found for glenoid version (P = .001), glenoid width (P < .001), glenoid height (P = .009), stability angle (P = .021) and glenoid index (P < .001) (Table 4). The mean length of the bone defect in the 36 ASI shoulders was 2.62 ± 2.21 mm, and that in the 21 ASI shoulders with bilateral data was 2.37 ± 1.92 mm (range, 0.01-7.42 mm).
Comparison of Glenohumeral Bony Characteristics Between ASI and Control Groups a
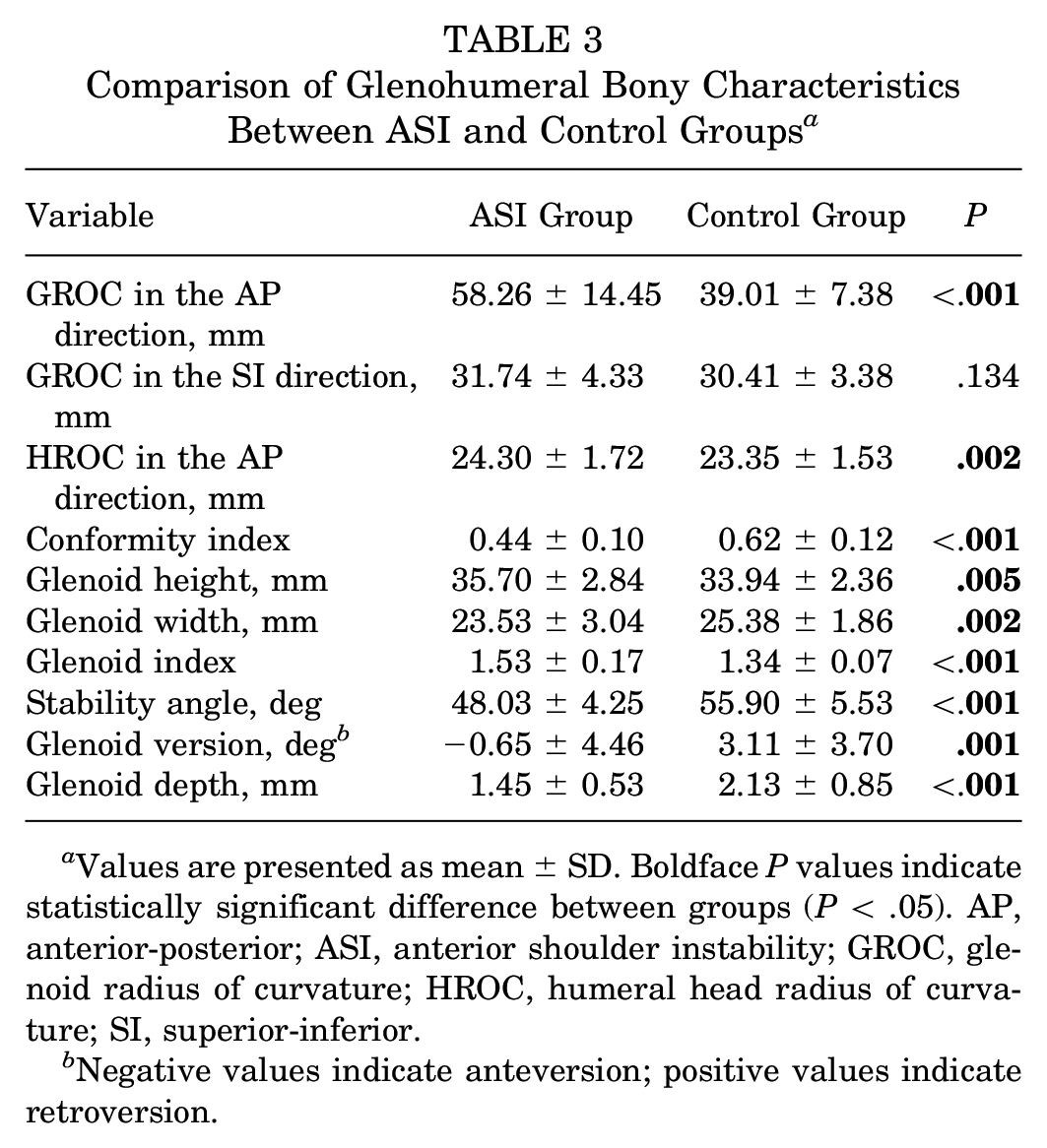
Values are presented as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). AP, anterior-posterior; ASI, anterior shoulder instability; GROC, glenoid radius of curvature; HROC, humeral head radius of curvature; SI, superior-inferior.
Negative values indicate anteversion; positive values indicate retroversion.
Comparison of Glenohumeral Bony Characteristics Between Affected and Contralateral Shoulders of ASI Patients a

Values are presented as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). AP, anterior-posterior; ASI, anterior shoulder instability; GROC, glenoid radius of curvature; HROC, humeral head radius of curvature; SI, superior-inferior.
Negative values indicate anteversion; positive values indicate retroversion.
Results of the correlation analysis indicated that in the ASI group, the length of the glenoid bone defect exhibited a negative correlation with glenoid width (r = −0.658; P < .001), stability angle (r = −0.638; P < .001), glenoid version (r = −0.398; P = .02), and glenoid depth (r = −0.344; P = .04). No correlation was found between glenoid defect and GROC or between the width of the Hill-Sachs lesion and HROC.
Discussion
In the current study, significant differences were observed between the ASI and control groups in GROC and HROC in the AP direction, conformity index, glenoid height, glenoid width, glenoid index, stability angle, glenoid version, and glenoid depth. Meanwhile, only glenoid height, glenoid width, glenoid index, stability angle, and glenoid version were significantly different between the affected and contralateral shoulders of the same ASI patients.
Notably, even though statistical significance was reached, HROC and glenoid height demonstrated small differences between the ASI and control groups, which may limit their practical significance in clinical settings. However, their roles in the calculations of conformity index and glenoid index were still noteworthy. In addition, although glenoid height, stability angle, glenoid version, and glenoid depth also exhibited statistically significant between-group differences, considering the impact of glenoid defect on these measurements, further discussions on their clinical significance are warranted. In the correlation analysis, we observed a negative association between the glenoid defect and glenoid width, glenoid version, stability angle, and glenoid depth, as the anterior bone defect would significantly affect these measurements. On the other hand, GROC and HROC were not correlated with any glenoid or humeral bone defects, respectively. This lack of association may be attributed to the fact that the lesion occupies only a limited portion of the articular curvature.
The ASI group had significantly greater GROC in the AP direction compared with controls (58.26 ± 14.45 mm vs 39.01 ± 7.38 mm, respectively; P < .001), although the comparison of bilateral GROC in the AP (P = .964) and SI (P = .684) directions were similar within the shoulders of the ASI patients. Based on these findings, we believe that glenoid curvature in the AP direction can be inherent and is strongly associated with the risk of anterior shoulder dislocation. Studies have demonstrated that the bony structural characteristics of the shoulder are related to the stability of the glenohumeral joint. In their case-control study, Peltz et al 14 found that the glenoid articular surface of both the affected and the contralateral shoulders of the ASI patients was flatter in the AP direction than that in healthy controls, although the differences in the morphology of the bilateral shoulders were small. However, that study was most likely underpowered due to the small sample size, and the lack of matching conditions in their control group was also a limitation. Our study included more patients and used a match-pairing design to further identify the differences in glenohumeral joint morphology between the affected and contralateral healthy shoulders, and we found results similar to those of Peltz et al. However, we also found the GROC in both the AP (58.26 ± 14.45 mm) and the SI (31.74 ± 4.33) directions was greater than that reported by Peltz et al. Such differences can be explained by the different measurement methods and ethnicities of the participants. Vaswani et al 18 used magnetic resonance imaging (MRI) to measure the GROC of patients who underwent arthroscopic Bankart repair, and the mean value of GROC (23.6 mm) was also smaller than our results. This may be due to the different measurement sources (MRI vs CT), and the changes in the glenoid labrum after surgery may also contribute to the differences. Although the measurements were different among the studies, the comparison results between the affected and contralateral shoulders were consistent. In addition, our finding that in patients with ASI, the GROC in the SI direction was smaller than in the AP direction was also consistent with previous studies.14,18
The conformity index, calculated as HROC/GROC, was used to measure the congruency of the glenohumeral joint. We found that this measurement was significantly smaller in the ASI group than in controls (0.44 ± 0.10 vs 0.62 ± 0.12, respectively; P < .001). Previous studies have shown that the stability of the glenohumeral joint depends on the geometric congruity of the humeral head and the glenoid articular surface. Using stereophotogrammetry, Soslowsky et al 15 found the congruency between the glenoid and humeral head was very high. If the thickness of cartilage is included, the difference in curvature radius between articular surfaces would be <2 mm in most cases. Even during the motions of the shoulder in all directions, the surfaces maintained good consistency. 16 Flatter articular surface or low congruency of the joint was associated with negative impacts on the stabilization mechanism.11,14 Theoretically, the congruency of the glenohumeral joint is greater if the conformity index is closer to unity. Compared with the measurements of radius of curvature alone, our conformity index values were closer to those in the literature, and the results among different studies were also consistent. In addition, the conformity index between the affected and contralateral sides for ASI patients in this study were basically unchanged (0.41 ± 0.09 vs 0.40 ± 0.06; P = .240). Therefore, we believe that the conformity index can be used as a reliable indicator for the prediction of ASI risks.
Glenoid depth also plays an important role in shoulder stability through the concavity-compression mechanism. In our study, the glenoid depth of the ASI shoulders was shallower than that of control shoulders (1.45 ± 0.53 mm vs 2.13 ± 0.85 mm; P < .001). During shoulder motion, the rotator cuff and deltoid muscles can press the humeral head into the glenoid concavity to increase the maximum tangential forces in all directions.9,20 In a case-control study, Moroder et al 11 found that the inherent flattening of the bony glenoid concavity, or the decrease of the glenoid depth, significantly reduced the bony shoulder stability ratio. Wermers et al 19 believed that as a predictor for the stability ratio, glenoid concavity was associated with greater impact on the developing of shoulder stability than was the size of a bony defect. In the current study, it was expected that the anterior bone loss in ASI patients would affect the glenoid depth measurements; however, the difference between the affected and contralateral healthy shoulders was not significant. Based on this finding, we believe that flattening of the glenoid can also be inherent in individuals with increased risk of ASI.
We found significant group differences in glenoid height and width. Since we did not control for patient height or body mass index in our comparisons and the original values of glenoid height or glenoid width may not be comparable among people of different sexes or heights, the glenoid index was proposed for the evaluation of shoulder dislocation. Yellin et al 21 found that a glenoid index >1.45 provided enough sensitivity (83%) and specificity (79%) to predict shoulder dislocation. A cohort study by Owens et al 13 demonstrated that patients with a glenoid index >1.58 had a 2.64 times higher risk of dislocation than those with a smaller glenoid index. Consistent with the findings in the literature, the results of the current study confirmed that the glenoid index was significantly larger in the ASI shoulders than in both the unaffected contralateral shoulders and the healthy control shoulders (P < .001 for both). Such differences can be attributed to bone defects in Bankart lesions.
The bone defect in the anterior glenoid edge was expected to make the stability angle smaller in the dislocation cases, since the stability angle was the angle enclosed by the lines connecting the center of the humeral head and the anterior and posterior edges of the glenoid articular surface. In the current study, the mean stability angles were 48.03° in the ASI group and 55.90° in the control group, which were similar to the results of Peltz et al, 14 with stability angles of 49.8° (instability patients, injured shoulder) and 56.9° (controls, dominant shoulder). However, the difference between the affected and unaffected contralateral sides was small in this study (47.14° vs 50.68°). It can be deduced that the stability angle may be inherently smaller in high-risk populations.
Glenoid version is also an important factor in both the onset and the development of ASI. Most studies have demonstrated that anterior glenoid version in ASI patients is greater than that in healthy individuals.1,6-8 However, the absolute values were different within the research, even though similar methods were applied. 3 Such differences may be associated with the group of populations investigated and the different sample sizes. However, almost all studies have shown that patients with ASI have obvious anteversion in the glenoid. In a case-control study by Aygun et al, 1 this phenomenon did not change significantly with age and sex. We found that the ASI glenoid was more anteverted than that of the healthy controls as well as of the unaffected contralateral side, which confirmed the results in the literature.
Limitations
This study has some limitations. First, our sample size was relatively small, especially for the unaffected contralateral shoulder of the ASI patients. Some of these patients had bilateral shoulders affected, and the extra costs and radiation made it more difficult to obtain such data, which potentially resulted in reduced statistical power. However, the purpose of the current study was to assess the differences between ASI patients and healthy controls, and we found significant results that were consistent with those in the literature. Consequently, we anticipated that the comparisons between affected shoulders and their unaffected contralateral sides would yield negative outcomes rather than statistically positive results, which ultimately supported our conclusions. Second, the glenoid with bone defects in ASI cases was not further classified or excluded. Considering that a smaller sample size may further reduce statistical power, the subgroups were not included in this study. According to our measurements, the influence of the glenoid bone defect was small and acceptable.
Conclusion
In this study, glenoid curvature variations were strongly linked to ASI as previously reported. Inherent factors such as the GROC and conformity index could potentially predict the risk of ASI. The stability angle and glenoid depth might also be inherent due to limited impact from glenoid bone defects. Further research with larger samples is needed to validate these findings.
Footnotes
Final revision submitted September 7, 2023; accepted November 13, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was financially supported by the International Cooperation Project of Science and Technology Department of Jilin Province (No. 20200801074GH). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from China-Japan Union Hospital of Jilin University (reference No. 2017060703).