
Abstract
Background:
There is a dearth of knowledge on anterior shoulder instability in older patients.
Purpose/Hypothesis:
The purposes of this study were to describe the incidence and epidemiology, injury characteristics, and treatment and outcomes in patients ≥50 years old with first-time anterior shoulder instability. We also describe the historical trends in diagnosis and treatment. It was hypothesized that the rates of obtaining a magnetic resonance imaging (MRI) scan and surgical intervention have increased over the past 20 years.
Study Design:
Descriptive epidemiology study.
Methods:
An established geographic database was used to identify 179 patients older than 50 years who experienced new onset anterior shoulder instability between 1994 and 2016. Medical records were reviewed to obtain patient characteristics, imaging characteristics, and surgical treatment and outcomes, including recurrent instability. Comparative analysis was performed to identify differences between age groups. Mean follow-up time was 11 years.
Results:
The incidence of first-time anterior shoulder dislocation in our study population was 28.8 per 100,000 person-years, which is higher than previously reported. Full-thickness rotator cuff tears were found in 62% of the 66 patients who underwent MRI scans. Of all patients, 26% progressed to surgery at a mean time of 1.6 years after injury; 57% of all surgical procedures involved a rotator cuff repair, and 17% included anterior labral repair. All patients who underwent a labral repair also underwent concomitant rotator cuff repair. The rate of recurrent instability for the cohort was 15% at a median of 176 days after the initial instability event. There were no instances of recurrent instability after operative intervention. At an average of 7.5 years after the initial instability event, 14% of patients developed radiographic progression of glenohumeral arthritis. The rate of surgical intervention within 1 year of initial dislocation increased from 5.1% in 1994 to 1999 to 52% in 2015 to 2016.
Conclusion:
The incidence of first-time anterior shoulder instability in patients aged ≥50 years was 28.8 per 100,000 person-years. Full-thickness rotator cuff tears (62%) were the most common condition associated with anterior shoulder instability, followed by Hill-Sachs lesions (56%). The rate of recurrent instability for the entire cohort was 15%, with no instances of recurrent instability after operative intervention.
Shoulder dislocations are common in the young and old alike. 22,23 Approximately 1% to 2% of the general population will sustain a traumatic shoulder dislocation each year. 37 Although most of the literature focuses on younger patients, nearly 20% of all shoulder dislocations occur in patients over the age of 60 years. 15 Although incidence of shoulder instability peaks in the third decade of life, there is a bimodal distribution, with a second smaller peak in incidence seen in the eighth decade of life. 39 The incidence of first-time anterior shoulder dislocation (FTAD) in the age group 50 to 70 years ranges anywhere from 12.9 to 28.1 per 100,000 person-years compared with an incidence of 80.5 per 100,000 person-years for male patients aged 16 to 20 years. 25,39
FTAD in patients older than 50 years has substantial differences in injury patterns compared with FTAD in younger patients. Older patients are much less likely to experience a recurrent shoulder dislocation compared with their younger counterparts. 5,11,15,38 Overall rates of recurrent instability for patients aged ≥50 years are reported to be <10% in most literature. 19,27,35 Because of age-related rotator cuff degeneration, 13 the rotator cuff tendons become the weak point of the stabilizing structures of the shoulder, as opposed to the capsulolabral complex in young patients. Therefore, rotator cuff tears are quire commonly associated with anterior dislocations. 7,12 The shoulder may be predisposed to residual instability if the rotator cuff restraints are lost. 4 A cadaveric study demonstrated that a 50% decrease in rotator cuff muscle firing was associated with a 50% increase in dislocations. 21 Because of these tears, pain and disability can persist long after the initial dislocation event. 6,18 In addition to tendon injuries, because elderly patients are more likely to have osteoporotic bone, even low energy injuries can cause large humeral head compression fractures (Hill-Sachs lesions) or glenoid fractures. 15 Surgical management in this patient population often centers around repair of the rotator cuff rather than the capsulolabral complex as would be expected in the younger patient. 17
The majority of the published literature on anterior shoulder instability has concentrated on young athletic patients. Because of the unique presentation and constellation of injuries associated with the older patient, this population deserves specific attention and further study. Many of the studies looking at FTAD in older patients were published before the turn of this century, and some include cases from >80 years ago. Few studies have examined the natural history of FTAD in patients aged ≥50 years or reviewed how the diagnosis and treatment of FTAD has changed over the past 2 decades. Similarly, long-term outcomes in this patient population are lacking.
The primary aim of this study was to address those deficits in the literature and produce an age-based geographic population-based analysis of FTAD in an older cohort with long-term follow-up. Specifically, the goals of this study were to describe the (1) incidence and epidemiology, (2) injury characteristics, and (3) treatment and outcomes in patients aged ≥50 years with FTAD, along with (4) historical trends in diagnosis and treatment. It was hypothesized that the rates of obtaining a magnetic resonance imaging (MRI) scan and surgical intervention have increased over the past 20 years.
Methods
Study Population and Design
The Rochester Epidemiology Project (REP) was used to identify patients with FTAD between January 1, 1994, and July 31, 2016. More than 500,000 patients compose the REP geographic database, complete with medical records of all residents in Olmsted County, Minnesota, and neighboring counties in southeast Minnesota and western Wisconsin. Individuals are included in the database if they have resided in Olmsted County for any point between 1966 and 2008. The validity and generalizability of the REP has previously been described in detail. 33,34 Patients were identified utilizing International Classification of Diseases, Revision 9, diagnosis codes for shoulder instability. Inclusion criteria consisted of (1) patients diagnosed with ≥1 anterior shoulder dislocation events, (2) aged ≥50 years at the time of initial instability, (3) minimum of 2 years of follow-up, and (4) consent given for research. Exclusion criteria consisted of patients with (1) multidirectional or posterior shoulder instability, (2) previous instability events occurring before the age of 50 years, or (3) primary acromioclavicular/sternoclavicular joint dislocations. Institutional review board approval for this study was obtained from both Mayo Clinic and Olmsted Medical Center.
Incidence/Epidemiology
A patient was considered to have FTAD if there was a documented clinical diagnosis of either glenohumeral dislocation that was made by a consultant physician on the basis of physical examination, history, and radiographic evaluation or glenohumeral subluxation, which was made by radiographic evaluation. Patient medical records were reviewed to obtain patient characteristics and demographics (including age, sex, body mass index [BMI], occupation, smoking status, previous surgery on affected shoulder). All exclusion criteria were confirmed with manual chart review.
Injury Characteristics
The radiographs and radiology report were scrutinized for the presence of a Bony Bankart lesion, Hill-Sachs lesion, or humeral head fracture. Osteoarthritis was graded by the primary author (A.A.S.) using the Samilson and Prieto grading system for postinstability arthritis. Any patient with grade 1 to 3 changes was considered to have arthritis.
Similarly, the magnetic resonance imaging (MRI) scans and MRI report were scrutinized for the presence of a Bankart lesion (soft tissue vs bony), cartilage impression fracture, Hill-Sachs lesion, biceps pathology (tendinopathy, partial/complete tear), and rotator cuff tear (partial/full thickness). The indications for obtaining an MRI scan were provider specific; however, most commonly listed indications were residual shoulder pain and concern for rotator cuff tears.
Treatments and Outcomes
Patients who underwent surgery were identified through manual chart review. Operative reports were reviewed for all patients who underwent surgical repair. Various surgical details were noted such as type of repair (rotator cuff tendons, labrum, fracture). Timing of operative intervention was noted in relation to the date of the initial instability event. Early surgical management was defined as intervention within 3 months of initial dislocation event. The main outcome of interest was recurrence of instability for the entire cohort. This diagnosis of recurrent dislocation or subluxation was made by a consulting physician.
Statistical Analysis
Descriptive statistics were reported as means and standard deviations for continuous variables and counts and percentages for categorical variables. Age- and sex-specific incidence rates of FTAD in Olmsted County were calculated by using the number of new-onset FTAD occurrences (incident cases) as the numerator and the corresponding population estimates based on decennial census counts as the denominator. A subgroup analysis was conducted by age group, which was delineated by half decade. Incidence rates were adjusted for age and sex by direct standardization to the 2010 US total population and are reported as rate per 100,000 person-years. The 95% CIs for the incidence rates were constructed with the assumption that the number of incident cases per year follows a Poisson distribution.
Trends over time and across age groups in the rate of radiographic and MRI findings were evaluated using logistic regression. Time-to-event outcomes (such as the need for surgery) were analyzed using survivorship methodology, including Kaplan-Meier estimation. All statistical tests were 2-sided and P values <.05 were considered statistically significant. All analyses were conducted using SAS Version 9.4 (SAS Institute, Inc.) and R Version 3.6.2 (R Foundation for Statistical Computing; 2019).
Results
Incidence and Epidemiology
A total of 179 patients were identified as having a clinically confirmed diagnosis of FTAD after the age of 50 years. The mean age of initial instability was 59.6 years (range, 50-70.5 years) (Table 1); 54.2% of the cohort was female and the average follow-up was 10.8 years (range, 2-26.2 years). Mean BMI was 31.3 ± 7.1. The dominant shoulder was involved in 62.2% of all patients; 4.5% (8 patients) had previously had surgery on the same shoulder. All 8 of these operations involved a rotator cuff repair. Of the entire cohort, 26.8% identified as laborers.
Patient Demographics a

a Data are reported as n (%), mean (range), or mean ± SD. BMI, body mass index.
The overall age- and sex-adjusted incidence rate of FTAD was 28.8 per 100,000 person-years from 1994 to 2016. The highest incidence rates occurred in the age group 60 to 64 years, with 28.3 for men and 38.1 for women, 33.4 overall. The lowest incidence rates occurred in the age group 50 to 54 years, with 22.6 for men and 21.2 for women, 21.8 overall (Figure 1). There were no statistically significant findings between the various age groups.

Incidence of anterior instability by age (years).
Injury Characteristics
Radiographic Findings
At time of initial evaluation, 177 patients underwent radiographs, which were examined for additional findings (Figure 2 and Table 2). Radiographic images were reviewed by the primary author; however, images were not available for 47 patients. In those cases, the radiology report served as the basis for diagnosing pathology. The most frequent pathologic finding on radiographs were Hill-Sachs lesions (47.7% overall), especially in the patient cohort aged 55 to 59 years (56.8%). Bony Bankart fractures were seen in 20.3% of all patients, again with an increased prevalence in the 55- to 59-year age cohort (28.9%). Humeral head fractures were the least common lesion observed, occurring in 10.3% of all cases. Out of 19 patients with humeral head fractures, 15 had isolated greater tuberosity fractures; 4 of these patients underwent open reduction and internal fixation (ORIF) of the greater tuberosity. One patient sustained a 3-part comminuted intra-articular head split fracture at the humeral neck that required ORIF; 1 patient sustained a comminuted, impacted fracture through the proximal humeral neck with displaced fractures of the greater tuberosity and the lesser tuberosity, which were treated nonoperatively. Humeral head fractures were more common in the 50- to 54-year (13.6%) and 55- to 59-year (13.6%) age groups compared with the 60- to 64-year (6.3%) and 65- to 70-year (8.1%) age groups; however, this did not reach significance (P = .26 and .46, respectively).

Radiographic findings by age at first-time anterior shoulder dislocation. Radiographs were not available for 47 patients.
Radiographic Findings by age at FTAD a

a Data are reported as percentages. Radiographs were not available for 47 patients. FTAD, first-time anterior shoulder dislocation. .
Advanced Imaging Findings
Of the initial 179 patients, 66 underwent MRI at an average of 1.3 years (range, 4 days–13 years) after the initial injury (Figure 3 and Table 3). Five were magnetic resonance arthrograms, 61 were traditional MRIs. MRI images were primarily reviewed by the primary author; however, images were not available for 8 patients. In those cases, the radiology report served as the basis for diagnosing pathology. The indications for obtaining an MRI scan were varied and dependent on provider preference. The most commonly cited indications were persistent shoulder pain and concern for rotator cuff tear. Of those who underwent an MRI evaluation, rotator cuff tears were the most prevalent injury, found in 92.4% of all patients; 62.1% presented with a full-thickness rotator cuff tear while 30.3% had a partial-thickness rotator cuff tear. Of the full-thickness rotator cuff tears, 48% were isolated supraspinatus tears, 2.4% were isolated infraspinatus tears, and 4.8% were isolated subscapularis tears; 24% had a combined supraspinatus and infraspinatus tear and 9.6% had a combined supraspinatus and subscapularis tear; 11.9% had a complete supraspinatus, infraspinatus, and subscapularis tear. Soft tissue Bankart lesions were observed in 52.4% of the cohort, whereas only 22.7% had a bony Bankart lesion. Biceps pathology was found in 42.4% of patients; however, only 3 patients had complete full-thickness tears of the biceps with retraction. The rest presented with tendinopathy and/or partial tearing of the long head of the biceps. The frequency of Hill-Sachs lesions in the MRI cohort (56.1%) was slightly higher than the frequency discovered in the radiographic cohort (47.7%). Chondral fractures were the least common diagnosis and occurred in only 10.8% of all patients. There were no statistically significant differences found in MRI findings and age at FTAD diagnosis.

Magnetic resonance imaging findings by age at first-time anterior shoulder dislocation.
MRI Findings by Age at FTAD a

a Data are reported as percentages. FTAD, first-time anterior shoulder dislocation; MRI, magnetic resonance imaging; RCT, rotator cuff tear.
Treatment and Outcomes
Surgical Intervention
A total of 47 patients (26.3%) ultimately underwent surgery at a mean time of 1.6 years after injury. 26 (14.5%) underwent early surgical management (within 3 months of initial dislocation event), whereas 21 (11.7%) had delayed surgical treatment. The Kaplan-Meier estimates for progression to surgery were 7.5% at 30 days (95% CI, 3.5%-11%), 15% at 90 days (95% CI, 9.6%-20%), 22% at 1 year (95% CI, 15%-28%), and 25% at 10 years (95% CI, 19%-32%).
Of the 47 operations, the most common surgical intervention was rotator cuff repair (57.4% of all operations), followed by anterior labral repair (17.0%) (Figure 4 and Table 4). All 8 patients who underwent an anterior labral repair also underwent a concomitant rotator cuff repair. Two patients (4.3%) underwent a Latarjet and 8 patients (17.0%) required an ORIF of either the humeral head or the glenoid. Only 1 patient underwent a rotator cuff repair and a biceps tenodesis. The majority of patients (51.0%) underwent surgery for persistent shoulder pain. The indication for surgical intervention for 8 patients (17.0%) was recurrent instability. There were no instances of recurrent instability after surgical intervention. There were 8 patients (17.0%) who underwent a reverse/total shoulder arthroplasty at a mean of 8.3 years after initial instability event. All of these surgeries occurred after the year 2010. Two patients underwent anatomic total shoulder arthroplasty for advanced glenohumeral arthritis. The indications for reverse total shoulder arthroplasty were cuff tear arthropathy in all patients except for 1. One patient presented with a 10-year history of a locked anterior dislocation and so the decision was made to proceed with a reverse shoulder arthroplasty.
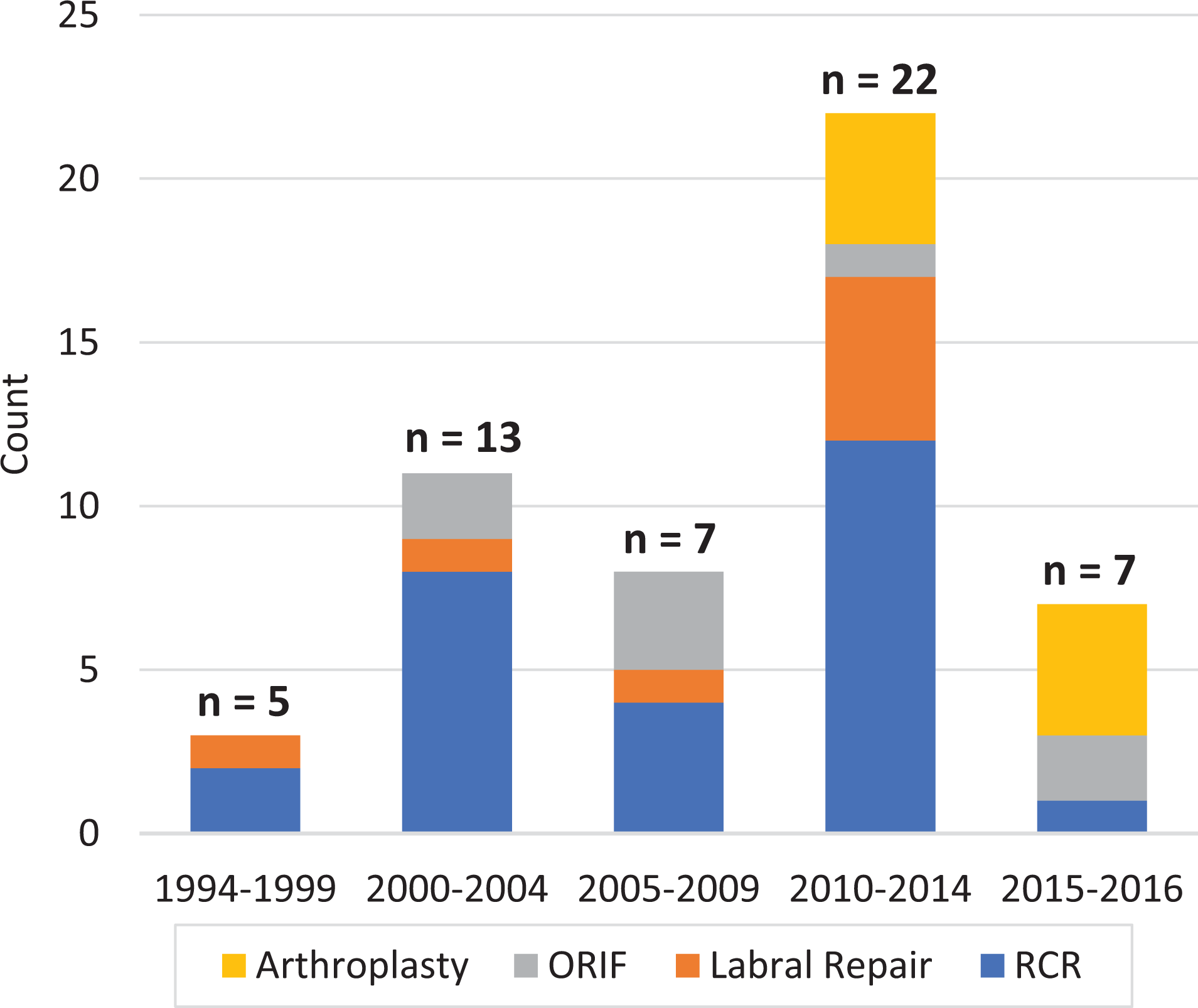
Types of surgical treatment, 1994 to 2016. Some patients underwent >1 procedure, and 3 patients did not fit the criteria of RCR, labral repair, ORIF, or arthroplasty. ORIF, open reduction and internal fixation; RCR, rotator cuff repair..
Types of Surgical Treatment From 1994 to 2016 a

a Values are presented as No. Some patients underwent >1 procedure, and 3 patients did not fit the criteria of RCR, labral repair, ORIF, or arthroplasty. ORIF, open reduction and internal fixation; RCR, rotator cuff repair.
Recurrence
Of the 27 patients (15.1%) who had recurrent instability after their initial event, 5 (18.5%) experienced only subluxations, while 22 (81.5%) had at least 1 recurrent dislocation event. These patients experienced an average of 2.8 additional dislocations/subluxations (range, 1-5). The median time until recurrent instability was 176 days (range, 1 day–18 years) after initial instability. 7 out of 27 (25.9%) of the recurrent dislocations occurred >3 years after the initial instability event. The mean age of patients experiencing recurrent instability was 60.2 years old (range, 52-68 years). There were no instances of recurrent instability after surgical intervention. Only 13 of the patients with recurrent instability underwent MRI evaluation; 4 out of 13 (30.8%) had full-thickness rotator cuff tears and did not undergo initial surgical management.
Arthritis
A total of 25 (14.0%) patients developed arthritis at an average of 7.5 years (range, 0.4-17.5 years) after their initial instability event. The mean age of patients developing arthritis was 64.6 years old (range, 51.1-80.9 years). Only 8 (4.5%) patients ultimately went onto require shoulder arthroplasty surgery. Of the patients who went on to shoulder arthroplasty, 6 were treated with initial conservative management; 2 patients who went on to shoulder arthroplasty were treated with initial operative management: 1 had undergone a labral repair and partial rotator cuff repair, whereas the other had undergone a rotator cuff repair.
Historical Trends in Diagnosis and Treatment
The rate of diagnosis of first-time shoulder dislocation in patients aged ≥50 years has stayed relatively stable over the past 2 decades (32.9 per 100,000 person-years for 1994-1999, 31.0 per 100,000 person-years for 2000-2004, 28.4 per 100,000 person-years for 2010-2016) with a slight decrease in the 2005-2009 (24.1 per 100,000 person-years) time period. Contrary to this, the rate of obtaining an MRI scan and proceeding to any kind of surgical intervention has greatly increased. The 30-day rate of obtaining an MRI scan after an initial presentation of FTAD increased from 7.8% in 1994 to 1999 to 24% in 2010 to 2014 and 20% in 2015 to 2016 (Figure 5). The 90-day rate of obtaining an MRI scan increased from 7.8% in 1994 to 1999 to 37% in 2010 to 2014 and 30% in 2015 to 2016. The 1-year rate of obtaining an MRI scan has increased from 10% in 1994 to 1999 to 47% in 2010 to 2014 and 42% in 2015 to 2016.

Rates of magnetic resonance imaging (MRI) at 30 days, 90 days, and 1 year after first-time anterior shoulder dislocation, 1994 to 2016.
The number of soft tissue Bankart lesions diagnosed by MRI increased in the years 2015 to 2016 (100%) compared with 1994 to 1999 (33.5%) (Table 5). Chondral fractures were more prevalent in the more recent cohort 2015 to 2016 (50%) compared with the 1994 to 1999 cohort (0%). The diagnosis of rotator cuff tears (full/partial thickness) has remained consistently high throughout the past 20 years, ranging from 83.3% of patients in 1994 to 1999 to 100% in years 2005 to 2009.
MRI Findings by Year of FTAD a

a FTAD, first-time anterior shoulder dislocation; MRI, magnetic resonance imaging; RCT, rotator cuff tear.
Similarly, the 30-day rate of surgical management for FTAD has increased from 5.1% in 1994 to 1999 to 20% in 2015 to 2016 (Figure 6). The 90-day rate of surgical management has increased from 5.1% in 1994 to 1999 to 30% in 2015 to 2016. The 1-year rate of surgical management has increased from 5.1% in 1994 to 1999 to 52% in 2015 to 2016.

Rates of surgical intervention for first-time anterior shoulder dislocation at 30 days, 90 days, and 1-year, 1994 to 2016.
Discussion
In this work, 179 patients diagnosed with initial FTAD event after the age of 50 years were followed for a mean of 11 years. In this population-based cohort study, the incidence of primary anterior shoulder dislocation was 28.8 per 100,000 person-years for patients aged 50 to 70 years. There was a peak in incidence in the age group 60 to 64 years, with a slight female predominance in the overall cohort. The most common concomitant pathologies present on MRI scans were full-thickness rotator cuff tears (62%) followed by Hill-Sachs lesions (56%). In all, 26% of patients ultimately underwent surgery at an average of 1.6 years after the injury. The rate of recurrent instability for the entire cohort was 15%, but the median time to recurrence was 176 days after the initial instability event.
While a few studies that estimate the incidence rate of shoulder instability among the general population have been performed, this study is the first we are aware of that is dedicated solely to patients who develop FTAD after the age of 50 years. 10, 25, 39 At 28.8 per 100,000 person-years, the incidence rate found in this study is slightly higher than those found in the corresponding subgroups in other investigations. One large population-based cohort study in the United Kingdom reported that the incidence rate was 19.8 per 100,000 person-years for patients 51 to 60 years old and 28.1 per 100,000 person-years for patients aged 61 to 70 years. 25 A database study in Canada that focused on anterior shoulder dislocations that required closed reduction found that the incidence rate for ages 41 to 70 years was 18.8 per 100,000 person-years. 10 A 2010 study that analyzed epidemiological trends from US census data found that, for ages 50 to 59 years, the incidence rate was 12.9 per 100,000 person-years, for ages 60 to 69 the incidence rate was 17.0 per 100,000 person-years, and for ages 70 to 79 years the incidence rate was 22.6 per 100,000 person-years. 39 There are a number of different possibilities for the higher incidence observed in the current study, such as differing demands/activities of different geographic groups; differing weather patterns in this area, with higher tripping hazards such as ice/snow; and a more robust investigational methodology that allows for identifying both surgically and nonoperatively treated patients that can then be verified via a detailed manual review of medical records.
Unsurprisingly, the most common concomitant pathology discovered with anterior shoulder instability in older patients was a rotator cuff tear. In this study, 62.1% of all patients who underwent advanced imaging were diagnosed with a full-thickness rotator cuff tear. The incidence of rotator cuff tears in patients aged >50 years with a primary traumatic anterior glenohumeral dislocation in the literature varies anywhere from 35% to 100% 1 ; however, most studies report an incidence of >80%. 6,18,27,30,35 The reasons for this finding are likely 2-fold. The prevalence of rotator cuff tears increases with age, as up to 50% of patients aged >50 years may have incidental cuff tears in some studies. 14,36 Secondly, to sustain an anterior dislocation of the humeral head, either the anterior or posterior supporting structures of the shoulder must be disrupted. After the age of 50 years, the assumption is that this usually takes place in the posterior-superior rotator cuff tendons, which is an area already highly susceptible to injury due to age-related weakening. 12,13 Craig 3 demonstrated that posterior rotator cuff tears correlate with an increased risk of anterior dislocation. In addition, in the past, high rates of concomitant full-thickness cuff tears may have been seen because of limited advanced imaging to solely capture those with clinical evidence of a cuff tear as well as significant symptoms.
Ultimately, 26% of all patients underwent surgical treatment, with almost half undergoing rotator cuff repair. This suggest that a large number of patients with full-thickness rotator cuff tears did not have symptoms severe enough to warrant surgery. There is dissent in the current literature about functional outcomes of patients aged >50 years undergoing surgical management for anterior shoulder instability. Consistently, studies have found that operative stabilization results in reduction of recurrence rates 2,20,26,32 ; however, some describe poorer functional outcomes in the older patient with concerns for the development of stiffness following stability surgery in this group. 11
Although recurrent instability is not typically thought to be a major issue for older FTAD patients, 15% of patients in this study experienced recurrent instability at a median of 176 days after the initial event. This is higher than the reported literature, which ranges from 4% to 11%. 10,19,38 This difference may be a consequence of the prolonged follow-up time in this study, as 7 out of 27 (25.9%) of the recurrent dislocations occurred >3 years after the initial instability event. Compared with young athletes, the recurrence rate is much lower, with a previous population-based study demonstrating a recurrence rate of 36% in patients with FTAD aged <40 years. 8 Overall, this supports the well-established doctrine that older patients remain at a decreased risk of recurrent instability compared with their younger counterparts 5,9,11,13,14,23 ; however, the 15% recurrence rate observed in this study is higher than was anticipated.
Degenerative arthritis following previous shoulder instability is a well-described entity. The term dislocation arthropathy has been used to describe the development of progressive glenohumeral arthritis in the setting of previous shoulder instability. 24 While 14% of all the patients developed progressive glenohumeral arthritis, only 4% of the entire cohort ultimately required shoulder arthroplasty. Studies have demonstrated that shoulder arthroplasty for osteoarthritis of the glenohumeral joint following instability can alleviate pain and improve motion, but is associated with a high rate of revision surgery, especially in the case of previous instability operative procedures. 16,31
While the rate of anterior shoulder instability in patients aged >50 years has remained relatively stable over the past 20 years, the rate of obtaining an MRI scan and proceeding to surgery has increased greatly. In this study, the diagnosis of pathology has stayed relatively the same, with the exception of soft tissue Bankart lesions and cartilage impression fractures. These increases are probably due to technological advances over the years, with the ability to see granular detail with greater ease. In addition, the rate of obtaining advanced imaging studies has increased dramatically across the United States since the start of the 21st century. 28 These increases can be attributed to technical improvements, such as increased strength of magnets and better interpretation, leading to accurate disease diagnosis, decreased costs, and physician and patient demand. However, these tests can be costly, and it has been estimated that around 30% of all imaging may be unnecessary, costing the United States approximately $30 billion each year. 29 The trend toward operative intervention for these patients has also become more common in more recent years. Surgical intervention within 1 year of anterior dislocation event has increased 10-fold over the past 20 years from 5.1% in 1994 to 52% in 2016.
Limitations
Given the retrospective nature of this study, this work is confined by the typical limitations of retrospective investigations. The decision to obtain an MRI scan was not standardized across providers or years, which introduces certain bias. Similarly, treatment approaches were not standardized across all providers or years. In addition, for patients who did undergo surgery, a standardized postoperative protocol was not utilized, and thus an analysis of the clinical status of patients following surgery could not be performed. Similarly, there was no standardized method of obtaining and reporting objective measures such as strength and range of motion at final follow-up, and so they were not able to be included in the results of our study. This work is also confined by the typical limitations of a confined geographic database. Patients could have experienced recurrences of shoulder instability outside of the area, and these would not have been accounted for in this study. The strengths of the study are its focus on a specific age group, inclusion of a large number of patients, and the ability to obtain long-term follow-up on the cohort.
Conclusion
The incidence of FTAD in patients over the age of 50 years was 28.8 per 100,000 person-years. Full-thickness rotator cuff tears (62%), in particular supraspinatus tears, were the most common concomitant pathology associated with first-time anterior shoulder instability in older patients observed on MRI scans. The rate of recurrent instability for the entire cohort was 15%, and the median time to recurrent instability was 176 days. There were no instances of recurrent instability after operative intervention. In all, 26% of all patients ultimately progressed to surgical intervention, and rotator cuff tears were the most common reason for surgical intervention.
Footnotes
Final revision submitted July 8, 2022; accepted July 27, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: Support was received from the Foderaro-Quattrone Musculoskeletal Orthopaedic Surgery Research Innovation Fund. Funding was received from the National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950). The Rochester Epidemiology Project (REP) medical records-linkage system is supported by the National Institute of Aging (AG 058738), by the Mayo Clinic Research Committee, and by fees paid annually by REP users. A.J.K. has received grant support from DJO; consulting fees from Arthrex, JRF Ortho, and Responsive Arthroscopy; speaking fees from Arthrex; royalties from Arthrex and Responsive Arthroscopy; and honoraria from JRF Ortho and Vericel; and he is a board member for MTF Biologics. K.O. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; consulting fees from Endo Pharmaceuticals and Smith & Nephew; speaking fees from Arthrex; and hospitality payments from Medical Device Business Services, Stryker, and Wright Medical. J.D.B. has received education payments from CDC Medical, consulting fees from Stryker, speaking fees from Arthrex, and hospitality payments from Wright Medical. C.L.C. has received nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mayo Clinic and Olmsted Medical Center (reference No. 16-007084 and No. 042-OMC-16).