
Abstract
Background:
Recently, the posterior horn lateral meniscal oblique radial tear (LMORT) was identified in 12% of acute anterior cruciate ligament (ACL) injuries. However, patient-reported outcomes for repair of this relatively common tear have not been reported.
Purpose:
To determine the minimum 2-year functional outcomes after LMORT repair at the time of ACL reconstruction (ACLR) compared to a matched cohort of patients who underwent isolated ACLR (iACLR).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 100 patients (mean age at surgery, 21 years; range, 13-45 years) who underwent primary ACLR between 2010 and 2018. The mean follow-up period was 4.1 ± 2.0 years (range, 2.0-9.2 years). A total of 50 patients with surgically repaired LMORT type 3 or type 4 lesions, defined as partial or complete tears >10 mm from the root (LMORT group) were matched 1:1 based on age, date of surgery, and graft choice with 50 patients who underwent iACLR (iACLR group). The postoperative outcomes were compared between groups using the International Knee Documentation Committee subjective score (sIKDC) and the Tegner activity scale. An updated medical history was obtained via the electronic medical record to determine any subsequent complications and reoperations.
Results:
There was 1 ACL graft failure in each group as well as 5 (10%) reoperations per group. None of the patients in the LMORT group necessitated a lateral meniscal revision repair or partial meniscectomy. The LMORT and iACLR groups reported comparable sIKDC scores (92.5 ± 6.8 vs 91.9 ± 8.2, respectively; P = .712) as well as Tegner scores (6.7 ± 1.8 vs 6.6 ± 1.8, respectively; P = .910) at final follow-up. No failures of the LMORT repairs were reported.
Conclusion:
The study findings demonstrated that reoperations, graft failure rates, patient-reported outcomes, and patient activity levels at ≥2 years after type 3 and 4 LMORT repairs at the time of ACLR compared favorably with those of a matched cohort of patients who underwent iACLR with intact meniscus.
Lateral meniscal tears commonly occur with anterior cruciate ligament (ACL) injuries.1,10,15 Posterior root tears of the lateral meniscus have been identified in 7% to 14% of patients with ACL pathology.10,15,30 A recent study has identified the lateral meniscal oblique radial tear (LMORT) of the posterior horn as one of the more common tear types, occurring in as many as 12% of patients with ACL injuries. 15 The proposed classification system identified 78% of LMORTs as partial (type 3) or complete (type 4) oblique tears extending >10 mm from the root. 15 These are distinct from both LMORT types 1 and 2, which are classified as occurring ≤10 mm from the root, as well as pure root tears.8,16
Appropriate treatment of LMORTs is to correct the altered knee kinematics that occur in the setting of these meniscal lesions.2,13,17,24,39 The biomechanical consequences of LMORTs and root tears are similar, both resulting in increased contact pressures, meniscal extrusion, and increased instability.12,18,29,34,36 A biomechanical study of LMORT types 3 and 4 by Smith et al 36 demonstrated worsening anterior translation, rotatory instability, and meniscal extrusion in ACL-deficient knees when compared with knees with an intact lateral meniscus. Additionally, the knee instability and meniscal extrusion persisted following ACL reconstruction (ACLR) if the LMORT was not repaired at the same time. 36 However, little evidence is available on the clinical outcomes for repair of these tear patterns. 8
The purpose of this study was to determine the minimum 2-year functional outcomes after LMORT repair at the time of ACLR compared to a matched cohort of patients who underwent isolated ACLR (iACLR). We hypothesized that patients who underwent LMORT repairs would have comparable failure and reoperation rates, as well as patient-reported outcomes (PROs), when compared with patients who underwent iACLR.
Methods
Patient Selection
Following institutional review board approval, a retrospective multicenter case-control study was performed at 2 academic sports medicine centers between 2010 and 2018. Patients who underwent primary ACLR with concomitant LMORT repair between 2010 and 2018 by 4 high-volume sports medicine and arthroscopic specialists (P.A.S., M.J.S., B.A.L., and A.J.K.) were identified. Arthroscopic photographs were carefully examined to classify the meniscal tear according to previous investigations. 15
An a priori power analysis for noninferiority 25 was performed with α = .05, β = 0.80, 10.4 for the noninferiority limit based on prior reports of the minimal clinically important difference of the International Knee Documentation Committee (IKDC) for patients undergoing ACLR 43 and a population SD of 11.5 based on prior reports in similar populations.1,3,41,45 A minimum sample size of 32 participants per group was determined.
Patient exclusion criteria consisted of (1) revision ACLR, (2) type 1 or 2 LMORT, (3) LMORT treated with transtibial root repair, inside-outside repair, or partial meniscectomy, and (4) patients who were found to have grade 3 or 4 cartilage lesions at time of arthroscopy. Of 58 eligible LMORT patients, 8 patients were unable to be contacted, resulting in an 86% follow-up rate. The final LMORT group consisted of 50 patients who (1) underwent ACLR with concomitant type 3 or 4 LMORT repaired with an all-inside technique (Figure 1), (2) had minimum 2-year follow-up data, and (3) were available for contact follow-up regarding confirmation of any complications, reoperations, and PROs. These patients were matched 1:1 with patients who received iACLR based on age, date of surgery, and graft choice. Matching was conducted with blinding of clinical outcomes. All participants provided informed consent.

Arthroscopic view from the anterolateral portal demonstrating a type 3 LMORT. (A) LMORT 3 prior to repair. (B) LMORT 3 reduced by a probe from the anteromedial portal. (C) Repaired LMORT 3. LMORT, lateral meniscal oblique radial tear.
Surgical Technique
An all-inside technique with 1 to 5 horizontal sutures was utilized as described by Smith et al. 36 In brief, a suture passer was used to pass a 0.9-mm suture tape on each side of the tear nearest the capsule for a spanning suture. A locking, sliding Tuckahoe-type knot was then tied followed by 2 alternating half-hitches. A second spanning suture was then placed closer to the free edge of the meniscus.
Postoperative Rehabilitation
The iACLR group underwent a standard ACL rehabilitation protocol consisting of 2 weeks of weightbearing as tolerated with crutches, 4 weeks of bodyweight-limited open chain exercises, and 6 weeks of weight-resisted open chain exercises with increasing range of motion. The LMORT group underwent the same rehabilitation program with limited weightbearing until 4 weeks and limited loads on weightbearing with the knee at ≥90° of flexion for 16 weeks.
Data Collection
An electronic chart review was performed to obtain baseline characteristics including age at surgery, sex, body mass index, laterality, and concomitant injuries. Perioperative data included classification of LMORT using arthroscopic images, ACL graft type, fixation type for all-inside meniscal repair, and cartilage quality. Postoperative end points collected were reoperation/failure, IKDC subjective (sIKDC) scores and Tegner activity scores. 5 The threshold Patient Acceptable Symptom State (PASS) for the sIKDC was set at 75.9 based on published data.21,23
Statistical Analysis
Data were reported as means with standard deviations for quantitative variables and frequencies with percentages for qualitative variables. The Student t test was used to compare parametric quantitative variables. The Pearson chi-square test was used to compare parametric qualitative variables. Data analysis was performed using JMP (Version 17; SAS Institute Inc), and P < .05 was considered statistically significant.
Results
Patients and Injury Characteristics
Included were 100 patients (mean age at surgery, 21 years; range, 13-45 years). The mean follow-up period for the overall cohort was 4.1 ± 2.0 years (range, 2.0-9.2 years). The characteristics of the patients by group are summarized in Table 1. Patient age, sex, body mass index, laterality, and mean final follow-up times were comparable between the LMORT and iACLR groups. In the LMORT group, 35 (70%) tears were type 3 and 15 (30%) tears were type 4.
Patient Characteristics by Group a
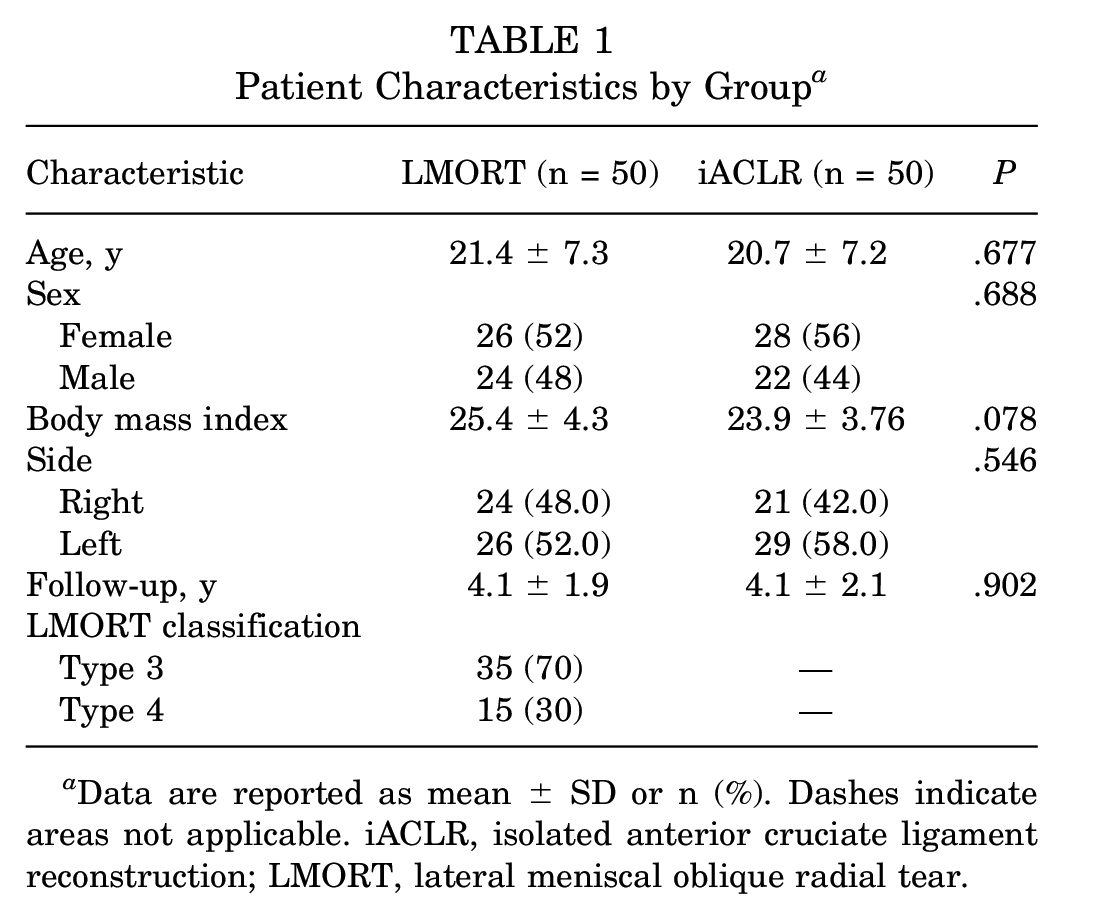
Data are reported as mean ± SD or n (%). Dashes indicate areas not applicable. iACLR, isolated anterior cruciate ligament reconstruction; LMORT, lateral meniscal oblique radial tear.
Associated Pathology and Operative Characteristics
Concomitant nonlateral meniscal surgeries were performed in 30 (60%) of LMORT patients and 3 (6%) of iACLR patients (Table 2). Medial meniscal procedures were performed in 19 (38%) of LMORT patients and zero of 50 iACLR patients (P < .001). There were no significant differences in any other concomitant procedures between groups.
Operative Characteristics by Group a

Data are reported as n (%). Dashes indicate not applicable. ACLR, anterior cruciate ligament reconstruction. APM, arthroscopic partial meniscectomy, BTB, bone-tendon-bone; iACLR, isolated ACLR; LMORT, lateral meniscal oblique radial tear; MCL, medial collateral ligament; MPFL, medial patellofemoral ligament.
One reoperation may consist of >1 procedure (eg, meniscal procedures often occur concurrently with revision ACLRs).
Debriding procedures include notchplasties, synovectomies, interference screw removals, and excision of fat pad fibroses.
There were 5 (10%) reoperations in each group. There was 1 ACL graft failure as well as 1 patient who underwent subsequent lysis of adhesions in each group. There were no significant differences in the types of procedures performed. There were no subsequent lateral meniscal procedures (revision repair or partial meniscectomy) noted in the LMORT group.
PRO Scores
The mean sIKDC and Tegner scores at the final follow-up were comparable between the groups (Table 3). Three patients in the iACLR group and 1 patient in the LMORT group did not meet the PASS threshold.
Patient-Reported Outcome Scores at Final Follow-Up a

Data are reported as mean ± SD. iACLR, isolated anterior cruciate ligament reconstruction; LMORT, lateral meniscal oblique radial tear; sIKDC, International Knee Documentation Committee subjective score.
Discussion
In this study, the failure/reoperations, PROs, and activity level after repair were equivalent to the patient population undergoing iACLR. This is the first clinical study to our knowledge comparing the outcome of type 3 and type 4 LMORT repair at the time of ACLR with a control group of iACLR patients.
We identified a reoperation rate of 5 (10%) in each group, with no LMORT repair failures, which is consistent with prior reports of excellent healing rates of lateral meniscal repairs in the setting of ACLR.3,7 De Leissegues et al 9 reported a reoperation rate of 10% (10/99) in a series of patients who underwent concomitant ACLR and lateral meniscal repairs or transtibial root repairs with a mean follow-up 42 months (Table 4). Anderson et al 3 reported reoperation in 5 of 24 patients undergoing combined ACLR and lateral meniscal repair with a mean follow-up of 58.6 months. These reports are similar to other studies regarding the reoperation rates of iACLR with the literature overall demonstrating a reoperation rate of 10% to 26% at mid- to long-term follow up.31,40
Studies of Lateral Meniscal Repairs in Setting of ACLR a

ACLR, anterior cruciate ligament reconstruction; NR, not reported; Reop, reoperation; sIKDC, International Knee Documentation Committee subjective score.
Mean or mean ± SD.
A 2022 study by Jeon et al 11 reported a complete healing rate of 80.3% in LMORTs with second-look arthroscopy. Similarly, a recent systematic review of lateral meniscal repairs in the setting of ACLR that included several of these studies found a complete or partial healing rate of 93.6%. 44 One possible explanation for the high rate of healing of repaired posterolateral meniscal tears associated with ACL rupture versus isolated radial tears could be the relatively increased vascularity near the meniscus roots versus the body. 7
There were no significant differences in the sIKDC scores between the 2 groups in this study, and scores were consistently better than those of previously reported series of ACLR and ACLR with lateral meniscal repair.7,9,24,33 Randsborg et al 31 reported a mean sIKDC of 84.3 in 1024 patients undergoing ACLR with no meniscal lesion at a mean 7.2-year follow-up. A recent series of 79 patients with minimum 2-year follow-up who underwent ACLR with LMORT repair reported a mean sIKDC score of 82.9. 11
A high activity level was maintained by patients in both groups in the current study, and the Tegner scores in our cohort were comparable with those of previously published series. Sonnery-Cottet et al 38 reported a mean Tegner score of 6.4 in patients undergoing iACLR. In a series of 8 patients undergoing all-inside lateral meniscal repair with ACLR, Anderson et al 3 noted a mean postoperative Tegner score of 5.8. Similarly, Song et al 37 reported a postoperative Tegner score of 6.7 at ≥12 months, at mean 24-month follow-up for posterolateral radial meniscal repairs in the setting of ACL tears. Other published studies of lateral meniscal repairs in the setting of ACLR with 2-year minimum follow-up include Jeon et al 11 who reported a mean Tegner score of 6.4 at a mean 32-month follow-up, Zhuo et al 45 who reported a mean Tegner score of 5.4 at a mean 26.7-month follow-up, and De Leissegues et al 9 who reported a mean Tegner score of 6 at a mean 42-month follow-up.
The results reported here are comparable with those of reported series of repairs of radial tears of the lateral meniscus.4,18 Choi et al 6 reported results of 14 patients who underwent repair of isolated radial tears of the midbody of the lateral meniscus with an all-inside technique with a mean follow-up of 36 months and mean Lysholm score of 94.7, Tegner score of 5.7, and magnetic resonance imaging (MRI) showing full (5/14) or partial (8/14) healing in 13 of 14 patients. A recent systematic review by Milliron et al 22 included 12 retrospective studies that reported results of radial meniscal tear repair with significant and clinically important improvement in Lysholm score (range, 47-68.9 preoperatively to 86.4-95.6 postoperatively) and Tegner score (range, 2.5-3.1 preoperatively to 4.7-6.7 postoperatively) at a mean 35-month follow-up (range, 12-76 months). Additionally, of those tears assessed by MRI or second-look arthroscopy, 62% showed full healing and an additional 30% partial healing.
Although some studies indicate that small peripheral lateral meniscal tears may be left in situ and fair acceptably without repair,20,33 biomechanical studies indicate that LMORT tears have a significant negative impact on meniscal function and stability and can result in increased joint laxity and meniscal extrusion.2,35,36 These findings suggest that ACL graft integrity could be compromised from a failure to repair the meniscus. 8 Regarding healing of these tears, second-look arthroscopy in LMORT tears as described by Jeon et al 11 showed 80.3% complete healing status and 19.7% partial healing status in 61 repaired LMORTs. As a substantial portion of the tear crosses obliquely through the red-red and red-white zones of the meniscus and repair is occurring during the time of ACLR, there is ample vascularity and stimulus to encourage healing of these tears when combined with anatomic repair.4,7,27,32,42 Additionally, these studies show that repair rather than management via meniscectomy is superior.35,36 Importantly, here we validate these studies indicating that not only is repair efficacious, but, clinically, the outcomes of repair are equivalent to having no meniscal tear at all. Similarly, lateral meniscus root repair at the time of ACLR has been shown to improve functional outcomes and prevent the accelerated progression of osteoarthritis.1,33,41
Limitations
Significant limitations of this study include that it is a retrospective study and thus subject to the bias of the surgeon selection of patients with LMORTs that were deemed appropriate candidates for repair. This bias is partially mitigated, as, at the centers where the study was performed, all type 3 and 4 LMORTs routinely undergo repair. The selection of a cohort of ACLR patients without LMORTs was matched on key demographic variables, but there is a possibility that ACL tears with LMORTs reflect a specific injury mechanism or pattern that is significantly different from that associated with isolated ACL tears. However, a cohort of iACLR patients was chosen for comparison given prior biomechanics studies that demonstrated iACLR was similar to ACLR+LMORT repair. Regarding the PASS threshold for this study, it is important to note it was set by a different cohort. Finally, we did not perform second-look arthroscopy or follow-up imaging to assess the status of the LMORT repair. However, given the previous reports of high rates of healing for posterior lateral meniscal tears 11 and the lack of patient symptoms requiring reoperation, we are confident these data would not change the clinical relevance of the reported results.
Conclusion
The study findings demonstrated that reoperations, graft failure rates, PROs, and patient activity levels at ≥2 years after type 3 and 4 LMORT repairs at the time of ACLR compared favorably with those of a matched cohort with iACLR with intact meniscus. No failures of the LMORT repairs were reported; however, long-term follow-up on this type of repair is needed.
Footnotes
Final revision submitted June 17, 2023; accepted June 29, 2023.
The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the US National Institutes of Health. One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was received from the US National Institute of Arthritis and Musculoskeletal and Skin Diseases for the Musculoskeletal Research Training Program (T32AR56950) and from the Foderaro-Quattrone Musculoskeletal/Orthopaedic Surgery Research Innovation Fund. E.T. has received a grant from Arthrex, education payments from Arthrex, and hospitality payments from Stryker. M.J.S. has received research support from Stryker, education payments from Arthrex, consulting fees from Arthrex, nonconsulting fees from Arthrex, and royalties from Arthrex. B.A.L. has received consulting fees from Arthrex and Smith & Nephew; nonconsulting fees from Arthrex, Smith & Nephew, and Linvatec; royalties from Arthrex; and stock from COVR Medical. P.A.S. has received research support from Arthrex; education payments from United Orthopedics and Elite Orthopedics; consulting fees from Arthrex; nonconsulting fees from Arthrex, Kairos Surgical, United Orthopedics, Medical Device Business Services, Elite Orthopedics, and Alpha Orthopedic systems; royalties from Arthrex; and stock options from Spinal Simplicity. A.J.K. has received research support from Aesculap, B. Braun, Ceterix, Arthritis Foundation, Histogenics, and Arthrex; a grant from DJO; consulting fees from Arthrex, Vericel, JRF Ortho, and Responsive Arthroscopy; nonconsulting fees from Arthrex; royalties from Arthrex and Responsive Arthroscopy; honoraria from JRF Ortho, MTF Biologics, and Responsive Arthroscopy; and hospitality payments from Gemini Mountain Medical and Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Mayo Clinic (reference No. PR15-000601-09).