
Abstract
Background:
Blood flow restriction training (BFRT) after anterior cruciate ligament reconstruction (ACLR) is rising in popularity because of its benefits in reducing muscle atrophy and mitigating knee strength deficits.
Purpose:
To investigate the impact BFRT has on adolescent knee strength after ACLR at 2 postoperative time points: at 3 months and the time of return to sport (RTS).
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A prospective intervention (BFRT) group was compared to an age-, sex-, and body mass index–matched retrospective control group. Patients aged 12 to 18 years who underwent primary ACLR with a quadriceps tendon autograft were included. Along with a traditional rehabilitation protocol, the BFRT group completed a standardized BFRT protocol (3 BFRT exercises performed twice weekly for the initial 12 weeks postoperatively). Peak torque values for isometric knee extension and flexion strength (at 3 months and RTS) and isokinetic strength at 180 deg/s (at RTS) as well as Pediatric International Knee Documentation Committee (Pedi-IKDC) scores were collected. Differences between the BFRT and control groups were compared with 2-way mixed analysis of variance and 1-way analysis of variance.
Results:
The BFRT group consisted of 16 patients (10 female; mean age, 14.84 ± 1.6 years) who were matched to 16 patients in the control group (10 female; mean age, 15.35 ± 1.3 years). Regardless of the time point, the BFRT group demonstrated significantly higher isometric knee extension torque compared to the control group (2.15 ± 0.12 N·m/kg [95% CI, 1.90-2.39] vs 1.74 ± 0.12 N·m/kg [95% CI, 1.49-1.98], respectively; mean difference, 0.403 N·m/kg; P = .024). The BFRT group also reported significantly better Pedi-IKDC scores compared to the control group at both 3 months (68.91 ± 9.68 vs 66.39 ± 12.18, respectively) and RTS (89.42 ± 7.94 vs 72.79 ± 22.81, respectively) (P = .047).
Conclusion:
In adolescents, the addition of a standardized BFRT protocol to a traditional rehabilitation protocol after ACLR significantly improved knee strength and patient-reported function compared to a traditional rehabilitation program alone.
Adolescent athletes continue to demonstrate an increase in the incidence of anterior cruciate ligament (ACL) injuries and subsequent ACL reconstruction (ACLR).6,14,50,52,53 In adolescents, outcomes after primary ACLR are suboptimal, as many patients fail to reach their previous level of activity 4 or go on to develop chronic knee pain.38,57 Up to a third of patients sustain a secondary ACL injury.13,16,28,56,58 Additionally, restoring knee strength and function is a priority after ACLR, but a concerning number of patients do not achieve recommended knee strength goals before returning to sport.17,18,54 Arthrogenic quadriceps inhibition after an ACL injury continues to be a barrier toward recovery, which makes it essential to investigate other strategies targeting quadriceps strength restoration. 44
Blood flow restriction training (BFRT) includes the application of a pneumatic cuff or tourniquet on a limb to restrict arterial inflow and occlude venous return. Combining this induced hypoxic environment with exercise is thought to promote muscle hypertrophy through altered cell signaling, increased protein synthesis, and stem cell proliferation.21,42 Traditionally, the recommended method to increase muscle strength and muscle mass is through high-load resistance training,2,10 but BFRT with low-load resistance may yield similar improvements. 35 In recent reviews, BFRT demonstrated an increase in strength gains compared to standard low-load resistance training.22,51 This establishes BFRT as an attractive intervention for patients after ACLR, who hold limitations for engaging in heavy-load resistance training during the early rehabilitation phase.
BFRT after ACLR has gained considerable popularity as an attempt to mitigate lower extremity atrophy and knee strength deficits during the postoperative period of relative immobilization. 21 While there is evidence of BFRT being an effective intervention after ACLR, 11 systematic reviews fail to strongly recommend BFRT because of the heterogeneous populations and historically inconsistent implementation parameters used in the literature.9,12,34,39 Recent clinical trials in adults after ACLR have shown positive effects of BFRT using consistent personalized tourniquet systems, limb occlusion pressure (LOP), and repetition schemes.23,26
Although evidence is building in support of BFRT in the adult population, the effectiveness of BFRT in the adolescent population after ACLR has not yet been studied. The purpose of this study was to investigate the impact of BFRT on knee strength and function at 3 months postoperatively and at the time of return to sport (RTS). We hypothesized that a 12-week BFRT protocol would improve knee extension torque, knee extension strength symmetry, and Pediatric International Knee Documentation Committee (Pedi-IKDC) scores both early (3 months) and late (RTS) during the rehabilitation period.
Methods
Participants
This prospective interventional clinical trial (ClinicalTrials.gov registration No. NCT04285879) received institutional review board approval. From January 2020 to August 2021, participants were recruited from a single institution before undergoing ACLR performed by 1 of 2 board-certified orthopaedic sports medicine surgeons (J.L.P. and A.E.C.). All patients who fit the inclusion and exclusion criteria were approached for participation in this study. All included patients or their parents/guardians provided informed consent at their preoperative visit, and the rights of the participants were protected.
All patients were between 12 and 18 years of age; underwent primary ACLR using a quadriceps tendon autograft; had no known history of central or peripheral neurological impairments; and were free of any cardiac, pulmonary, or metabolic conditions. Exclusion criteria comprised previous surgical interventions either on the ipsilateral or contralateral knee or a history of deep vein thrombosis. Patients with concomitant meniscal repair requiring >2 weeks of weightbearing restrictions, multiligamentous injuries, and chondral abnormalities were also excluded.
The prospective intervention group underwent BFRT in addition to standard-of-care rehabilitation. These patients were compared to matched controls from an organizational database consisting of previously collected patients tested with the same methods who underwent ACLR between December 2017 and June 2021. For each patient in the intervention group, a control patient was obtained by filtering for inclusion and exclusion criteria, excluding those who had utilized BFRT postoperatively, and matching, in the following order, by (1) age (within 365 days), (2) sex, and (3) body mass index.
Study Protocols
Patients in both the intervention and control groups were prescribed a postoperative rehabilitation protocol and were advised to attend supervised rehabilitation sessions. The protocol, adapted from Adams et al, 1 initially focused on acute symptom management, restoring range of motion, normalizing gait, and lower extremity strengthening (available in the Appendix). Patients progressed to running, plyometric training, agility exercises, and sport-specific drills according to this time- and criteria-based protocol. The intervention group completed a standardized BFRT protocol in addition to typical rehabilitation for the initial 12 weeks at our institution. The control group underwent standard-of-care rehabilitation at either our institution or a community rehabilitation clinic.
Blood Flow Restriction Application
BFRT was administered using a personalized tourniquet system (Delfi Medical Innovations). At each physical therapy session, a limb protection sleeve, followed by a 4.5 inch–wide contour cuff, was placed on the most proximal portion of the involved limb. LOP, or the minimum pressure required for full arterial occlusion, 43 was calculated automatically with the patient in a supine position. BFRT was initiated at 80% of the patient's LOP,15,36 with a reduction up to 60% of the LOP 24 for fatigue or poor tolerance.
Blood Flow Restriction Exercises
All patients in the intervention group followed a standardized BFRT protocol for 12 weeks postoperatively (Table 1) during their scheduled physical therapy sessions. Patients initiated BFRT at their second postoperative session, which occurred within the first 2 weeks after surgery. This program included 3 exercises per session, with 2 sessions per week. Patients were required to complete a minimum of 90% of scheduled sessions to be included in this study.
BFRT Protocol a

BFRT, blood flow restriction training.
Each BFRT exercise followed a 30-15-15-15 repetition scheme, with 30 seconds of rest between each set. 46 The pneumatic cuff remained inflated for the duration of each exercise (75 repetitions or 8 minutes) but was deflated between each exercise. For all exercises, the rating of perceived exertion of a 1-repetition maximum was estimated with the modified OMNI-RES scale. This was used to determine the initial resistance, which was approximately 20% to 30% of their 1-repetition maximum. 49 Load progression for each exercise was based on the patient's ability to complete the prescribed number of repetitions with a rating of perceived exertion of less than 7 of 10, and patients were monitored for adverse events during and after each session.
Outcome Measures
Outcomes were collected at both early (3 months) and late (RTS) stages of rehabilitation. All patients underwent standardized testing that included range of motion examinations, strength tests, dynamic movement assessments, and patient-reported outcome measures. At early-stage testing, patients completed the Pedi-IKDC form and isometric knee extension and flexion strength tests. These outcomes were collected again at late-stage testing, with the addition of isokinetic knee extension and flexion strength tests at 180 deg/s.
Knee Strength
Peak torque was assessed by an isokinetic dynamometer (HUMAC NORM; CSMi). Patients were strap-stabilized in short sitting at 90° of hip flexion, with the dynamometer arm secured proximal to the ankle joint of the limb being tested. The contralateral/uninvolved limb was measured first for all strength tests, and verbal encouragement was provided throughout testing to encourage maximal effort. All test administrators were trained in CSMi-standardized guidelines for the dynamometer. These methods are reliable in quantifying quadriceps and hamstring peak torque in adults20,55 and children. 27
Isometric knee extension and flexion torque was measured at 60° of flexion. Patients completed 1 practice trial, followed by 3 test trials, with a 5-second rest between each. Knee extension strength was tested first, with patients holding for a 5-second isometric contraction at each trial. Peak torque was normalized to the patient's body weight (N·m/kg).
Isokinetic knee extension and flexion torque was measured from 0° to 90°. Patients completed 3 practice trials at 180 deg/s, followed by a 5-second rest, then 10 test trials. Similar to isometric strength outcomes, isokinetic peak torque values were normalized to body weight (N·m/kg).
Knee Strength Symmetry
Isometric as well as isokinetic knee extension and flexion normalized strength values were represented as a limb symmetry index (LSI), or the ratio between the ACLR and contralateral limbs. The LSI was calculated by dividing the ACLR limb's normalized peak torque value by the contralateral limb's normalized peak torque value and multiplying by 100 to represent symmetry as a percentage.
Patient-Reported Outcomes
The Pedi-IKDC is a 13-item valid and reliable outcome scale measuring knee function.5,25,31 The questionnaire was administered before each testing session.
Statistical Analysis
Descriptive statistics were calculated for all outcomes and were reported as means and standard deviations with 95% confidence intervals. Separate 2-way mixed analyses of variance (ANOVAs) were conducted to determine the effect of BFRT versus standard-of-care rehabilitation on isometric knee strength and patient-reported function over time. In the absence of interaction effects, main effects were assessed. For variables captured only at the RTS time point (ie, isokinetic strength), a single 1-way ANOVA was conducted to determine group differences. Dependent variables included isometric knee extension and flexion strength for the ACLR and contralateral limbs, LSI for isometric knee extension and flexion strength for the ACLR and contralateral limbs, isokinetic knee extension and flexion strength for the ACLR and contralateral limbs, LSI for isokinetic knee extension and flexion strength for the ACLR and contralateral limbs, and Pedi-IKDC scores. All data were normally distributed, and the alpha level was set to <.05.
Results
A total of 35 patients consented to participate in this study. Patients were excluded because of arthrofibrosis/cyclops lesions (n = 4), postoperative weightbearing restrictions (n = 4), no ACL tear (n = 1), and less than 90% of scheduled BFRT sessions completed (n = 10). Thus, the BFRT group of 16 patients (10 female; mean age, 14.84 ± 1.6 years) was age-, sex-, and body mass index–matched to 16 patients in the control group (10 female; mean age, 15.35 ± 1.3 years) (Table 2). The BFRT group had 15 patients who participated in a level 1 sport (jumping, frequent pivoting, hard cutting) 19 versus 14 in the control group (Table 2). The BFRT group had an adherence rate of 94% for their scheduled therapy sessions. The first BFRT session occurred at a mean of 8.4 days postoperatively.
Patient Characteristics a

Data are reported as mean ± SD or n (%). BFRT, blood flow restriction training; RTS, return to sport.
Two-Way Mixed ANOVA for Isometric Knee Strength and Patient-Reported Outcomes
The results of all strength and patient-reported outcome variables at both testing time points can be found in Table 3. There was a significant main effect for time for all variables except the contralateral limb's isometric knee extension strength.
Isometric Knee Strength and Patient-Reported Outcomes a
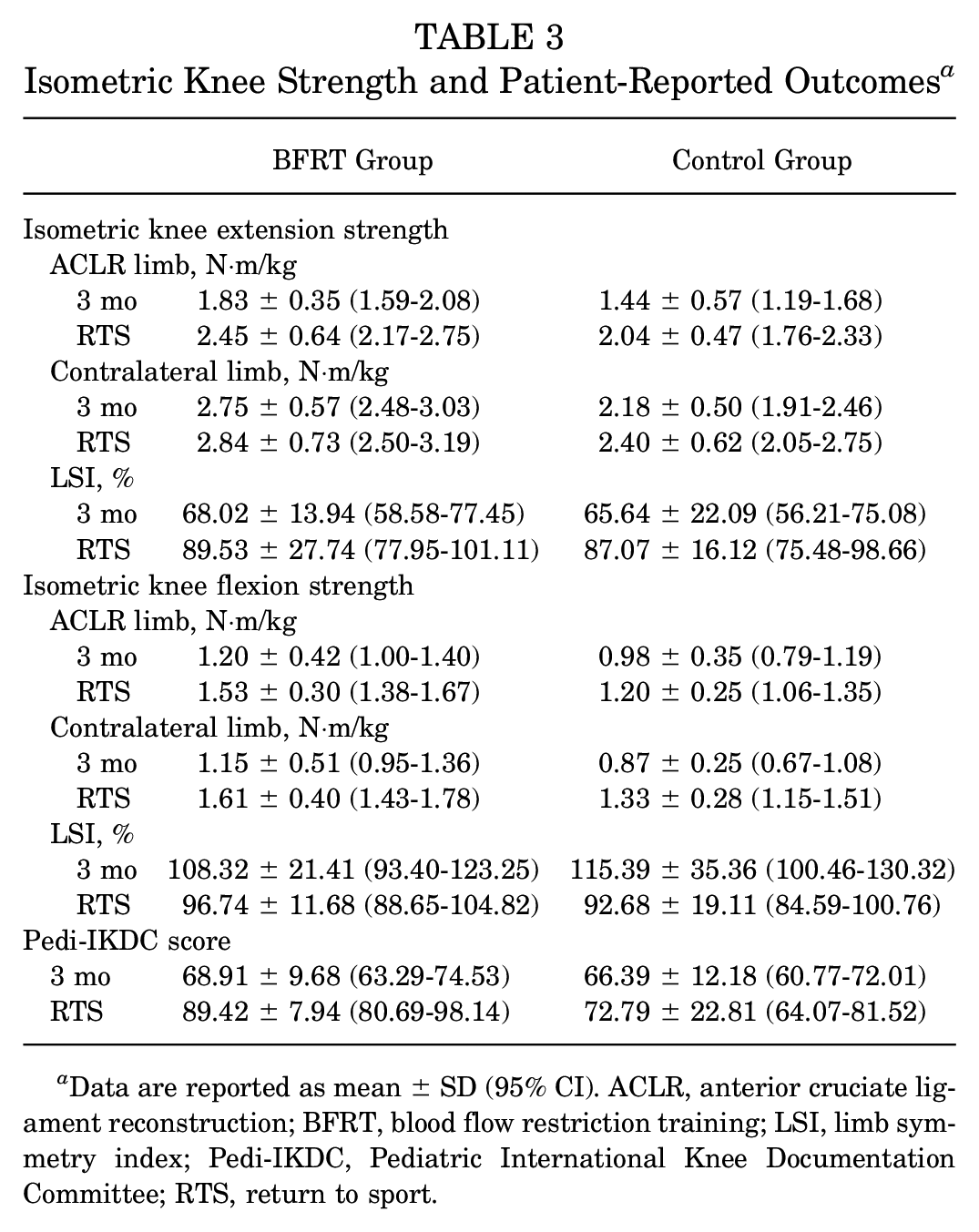
Data are reported as mean ± SD (95% CI). ACLR, anterior cruciate ligament reconstruction; BFRT, blood flow restriction training; LSI, limb symmetry index; Pedi-IKDC, Pediatric International Knee Documentation Committee; RTS, return to sport.
Isometric Knee Extension Strength for ACLR Limb
There was a main effect for group, showing a significant difference in the ACLR limb's isometric knee extension strength between the BFRT and control groups (F(1,30) = 5.648; P = .024; partial η2 = 0.158). The BFRT group demonstrated 0.403-N·m/kg (95% CI, 0.507-0.750) higher isometric strength for the ACLR limb compared to the control group.
Isometric Knee Extension Strength for Contralateral Limb
There was a main effect for group, showing a significant difference in the contralateral limb's isometric knee extension strength between the BFRT and control groups (F(1,30) = 7.255; P = .011; partial η2 = 0.195). The BFRT group demonstrated 0.510-N·m/kg (95% CI, 0.123-0.897) higher isometric strength for the contralateral limb compared to the control group.
LSI for Isometric Knee Extension Strength
There was not a significant main effect for group. The BFRT group demonstrated a 2.41% (95% CI, –10.01% to 14.83%) mean difference in isometric knee extension strength symmetry compared to the control group.
Isometric Knee Flexion Strength for ACLR Limb
There was a main effect for group, showing a significant difference in the ACLR limb's isometric knee flexion strength between the BFRT and control groups (F(1,30) = 7.040; P = .013; partial η2 = 0.190). The BFRT group demonstrated 0.267-N·m/kg (95% CI, 0.062-0.473) higher isometric strength for the ACLR limb compared to the control group.
Isometric Knee Flexion Strength for Contralateral Limb
There was a main effect for group, showing a significant difference in the contralateral limb's isometric knee flexion strength between the BFRT and control groups (F(1,30) = 6.202; P = .019; partial η2 = 0.171). The BFRT group demonstrated 0.275-N·m/kg (95% CI, 0.049-0.500) higher isometric strength for the contralateral limb compared to the control group.
LSI for Isometric Knee Flexion Strength
There was not a significant main effect for group. The BFRT group demonstrated less isometric knee flexion strength symmetry (mean difference [MD], –1.50% [95% CI, –13.07% to 10.70%]) compared to the control group.
Pedi-IDKC Score
There was a significant interaction effect between group and time on patient-reported knee function (F(1,30) = 4.296; P = .047; partial η2 = 0.125). There were also significant main effects for group and time. The BFRT group demonstrated better Pedi-IKDC scores compared to the control group (MD, 9.67 [95% CI, 1.86-17.27]). The main effect for time demonstrated that there was a significant improvement in Pedi-IKDC scores over time (F(1,30) = 15.65; P < .001), with an MD of 13.45 (95% CI, 6.50-20.40) between 3 months and RTS.
One-Way ANOVA for Isokinetic Knee Strength
Regarding isokinetic testing at the time of RTS, the BFRT group demonstrated significantly higher knee extension strength at 180 deg/s for the ACLR limb (F(1,30) = 5.034; P = .032; ω2 = 0.112) and higher knee flexion strength at 180 deg/s for the ACLR limb (F(1,30) = 10.618; P = .003; ω2 = 0.121) compared to the control group (Table 4). There was also a significant difference between the BFRT and control groups in the LSI for knee flexion strength at 180 deg/s (101.43% vs 90.19%, respectively; P = .027).
Isokinetic Knee Strength at RTS a
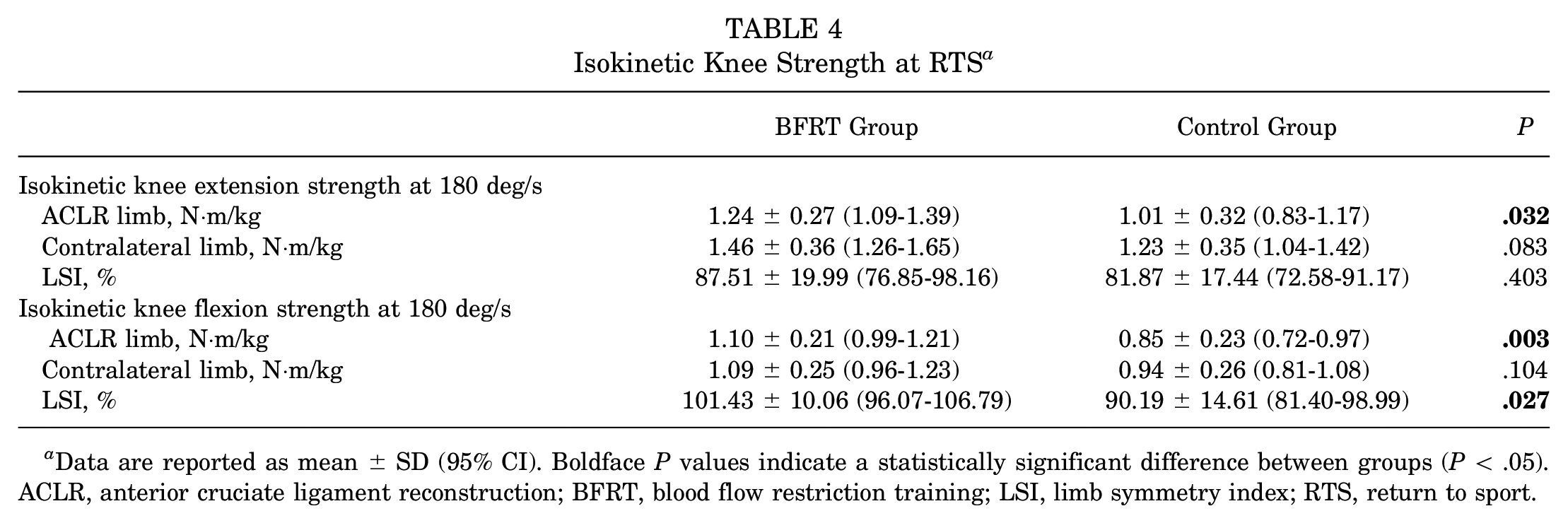
Data are reported as mean ± SD (95% CI). Boldface P values indicate a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; BFRT, blood flow restriction training; LSI, limb symmetry index; RTS, return to sport.
Discussion
The overall aim of this study was to investigate the impact of BFRT on knee strength after ACLR at 3 months and the time of RTS. There is mounting evidence to suggest that early restoration of knee extension strength can lead to improved knee function later in rehabilitation.8,29 We hypothesized that a 12-week BFRT protocol would improve knee extension strength, strength symmetry, and patient-reported function at both early (3 months) and late (RTS) stages of rehabilitation. Despite not observing a significant interaction effect between group and time, the results of our study suggest that BFRT was a viable intervention to address isometric knee extension peak torque in the ACLR limb and the contralateral limb after ACLR.
Regardless of the time point, patients who received BFRT demonstrated 0.403-N·m/kg higher isometric knee extension peak torque in the ACLR limb compared to patients in the control group (Table 3). Additionally, regardless of time, the BFRT group also showed 0.510-N·m/kg higher isometric knee extension peak torque in the contralateral limb compared to the control group (Table 3). Previous literature has suggested that BFRT may induce a systemic effect on strength gains in the contralateral extremity. 7 This was consistent with our results, as both the ACLR limb and the contralateral limb demonstrated improved isometric knee extension strength. Together, these data suggest that BFRT during the early phases of rehabilitation can demonstrate strength improvements that are retained at both 3 months and RTS in patients after ACLR. This is notable, as Toole et al 54 reported on young patients at the time of RTS after ACLR, stating that only 44% met recommended knee extension strength goals. Our results show a clinically relevant difference of 20% greater isometric knee extension peak torque and 23% greater isokinetic knee extension peak torque in the BFRT group's ACLR limb compared to the control group. These strength benefits appear similar to those seen in adults. Our findings corroborate previous work that reported that 86% of adults who completed BFRT after knee surgery demonstrated a 20% increase in isometric knee extension torque. 45
Although commonly assessed, knee extension strength symmetry should not be used as a stand-alone metric for RTS clearance. 59 The contralateral limb is known to be deconditioned during recovery after ACLR, resulting in a more symmetrical LSI and potentially misguiding clinicians on the patient's true baseline strength. 32 The findings of our study show a comparable knee extension strength improvement in both the ACLR limb and the contralateral limb in the BFRT group, with no difference in the LSI between groups. Assessing strength by normalizing peak torque to the patient's body weight may be better than the LSI in predicting the restoration of function after ACLR 47 and provides clinicians with an additional metric besides the LSI to assess strength recovery.
Patient-reported function is a common RTS criterion that young adolescents often do not adequately achieve after ACLR. 54 The BFRT group in our study demonstrated improved self-reported function (Pedi-IKDC) compared to the control group and significant improvements in Pedi-IKDC scores over time. These results highlight BFRT as a potential intervention early in rehabilitation that can lead to improved subjective outcomes throughout the course of rehabilitation, such as decreased symptoms, increased activity, and improved knee function.
Young adolescents have the highest risk for secondary ACL injuries, 33 resulting in a call for increased efforts toward pediatric- and adolescent-specific ACL research. 3 BFRT in adults after ACLR has gained significant popularity in recent literature. 30 Although BFRT has been utilized in healthy adolescents, 40 no previous studies have investigated BFRT and clinical outcomes in adolescents after ACLR. The results of this study are consistent with those of previous literature that has highlighted the positive influence of BFRT on knee extension strength in adults after ACLR. 23
A consensus regarding the effectiveness of BFRT on knee strength after ACLR has not been established, as recent reviews recommend future studies to prioritize patient homogeneity, utilize long-term subjective outcomes, and standardize BFRT parameters.12,30,39 This study adds to the current body of evidence as the first trial investigating the impact of BFRT on outcomes in adolescents after ACLR using a reproducible BFRT protocol and including late-stage RTS subjective and objective data. Our protocol replicated the personalized tourniquet systems, LOP, and repetition schemes that have demonstrated a positive effect in adults after ACLR.23,26 These results provide further guidance to clinicians when making clinical decisions regarding the appropriate dosage and parameters of BFRT.
Although there is only scarce literature available on the safety of and tolerance to BFRT in the adolescent population, 48 it is worthwhile to note the absence of any significant adverse events in our study. BFRT was started acutely (mean, 8.4 days) after ACLR and tolerated by patients ranging in age from 12 to 18 years. This aligns with relatively good tolerance to BFRT reported in the adult population,37,41,60 which should not be considered a barrier to further investigations on the efficacy of BFRT in young adolescents.
Limitations
The main limitation of this study was the lack of a prospective control group. Originally designed as a 2-arm trial, a significant number of enrolled controls were lost to follow-up, as this study occurred during the height of the COVID-19 pandemic. Although there was no difference in sport levels between groups, a possibility of recruitment bias exists, as we did not record the number of eligible patients who declined to participate in our intervention group. Additionally, only patients who successfully completed 90% of scheduled BFRT sessions were included in this analysis, potentially excluding patients from the intervention group who were inconsistent with formal rehabilitation or sustained postsurgical complications. Physical therapy initiation and compliance were not accounted for in our control group. No claims can be made regarding the effect of BFRT on skeletally immature patients, as only chronological age was recorded and not bone age.
Conclusion
In adolescents, the addition of a standardized 12-week BFRT protocol to a traditional rehabilitation protocol after ACLR improved isometric and isokinetic knee extension strength throughout recovery compared to a control group. Adolescents undergoing ACLR may benefit from BFRT in the early phases of rehabilitation to address both short- and long-term knee strength deficits and improve subjective knee function. Continued investigation in this high-risk adolescent population is needed to further determine the efficacy of BFRT on knee strength. Future randomized trials should examine the optimal frequency and duration of BFRT after ACLR in this population to assist with clinical integration and utility.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671231213034 – Supplemental material for Early- and Late-Stage Benefits of Blood Flow Restriction Training on Knee Strength in Adolescents After Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-pdf-1-ojs-10.1177_23259671231213034 for Early- and Late-Stage Benefits of Blood Flow Restriction Training on Knee Strength in Adolescents After Anterior Cruciate Ligament Reconstruction by Dylan P. Roman, Julie P. Burland, Arthur Fredericks, Nicholas Giampetruzzi, Jennifer Prue, Adel Lolic, J. Lee Pace, Allison E. Crepeau and Adam P. Weaver in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted June 6, 2023; accepted June 20, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Two Delfi Medical Innovations BFRT units were provided by Owens Recovery Science. J.L.P. has received education payments from Kairos Surgical, has received consulting fees from Arthrex and JRF Ortho, has received nonconsulting fees from Arthrex, and has stock in OutcomeMD. A.E.C. has received education payments from Fortis Surgical and Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Connecticut Children's Medical Center (No. 19-168).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.