
Abstract
Background:
Deltoid ligament reconstruction of the ankle can be considered when the ruptured ligament is insufficient for direct repair.
Purpose:
To compare the safety of talar tunnels oriented toward 4 different anatomic landmarks on the lateral malleolus during reconstruction of the deep layer of the deltoid ligament (DDL).
Study Design:
Descriptive laboratory study.
Methods:
A total of 30 computed tomography scans of the ankle joint in healthy adults were collected to generate 3-dimensional models. Virtual talar tunnels with a diameter of 5 mm and with different lengths (20.0, 25.0, and 30.0 mm) were created from the talar insertion of the DDL and were oriented toward the talar neck as well as the most anterior, the most distal, and the most posterior points of the distal fibula. The minimal safe distance (MSD) of a drilling route was calculated for the tunnels, and the safe distance from the end of the tunnel to the bone surface was measured for each tunnel. The nonpaired Student t test was used to detect differences among the safe distances of the 4 different bone tunnels.
Results:
For the 20.0-mm tunnels, the safe distance of the tunnel oriented toward the talar neck (5.90 ± 1.16 mm) did not meet the MSD (6.0 mm). For the 25.0-mm tunnels, the safe distances of the tunnels oriented toward the talar neck (4.53 ± 1.13 mm) and the anterior point of the fibula (5.91 ± 1.52 mm) did not meet the MSD (6.9 mm).
Conclusion:
Tunnels that were 5 mm in diameter and 20.0 and 25.0 mm in length, oriented toward the most distal or most posterior point of the distal fibula, were safe for DDL reconstruction.
Clinical Relevance:
Knowledge of safe talar tunnel placement is important, especially to avoid bone surface penetration during DDL reconstruction.
Ankle sprains are among the most common injuries during sports and recreational activities. 8 Although lateral ligaments are most frequently involved in ankle sprains, epidemiological studies have shown that deltoid ligament injuries are present in 5.1% to 15.8% of ankle sprains.14,24 As imaging technologies and arthroscopic examinations continue to improve, the incidence of deltoid ligament injuries may increase compared with previously reported data. More deltoid ligament injuries are identified as the result of an isolated injury or a concomitant injury of another complex mechanism.10,15 Deltoid ligament tears can result in medial instability or multidirectional instability when associated with other ligament injuries. 28
The deltoid ligament is a complex structure and is the primary medial stabilizer of the ankle joint, limiting valgus tilt and anterior translation of the talus.9,18 Surgical reconstruction needs to be considered for patients who have unsuccessful nonoperative treatment or primary repair with chronic deltoid ligament insufficiency. 20 Deltoid ligament reconstruction is also necessary when the residual deltoid ligament is insufficient for direct repair. 20 Although anatomic studies have identified the insertion at the talus, the bone tunnel can be oriented in different directions. To avoid a fracture or a potential risk of cartilage lesions, the bone tunnel for reconstruction should not penetrate the joint surface. 3 Michels et al 17 analyzed the minimal safe distance (MSD) of different tunnels for reconstructing the anterior talofibular ligament using virtual measurements in 3-dimensional (3D) bone models. A safe bone tunnel orientation would prevent penetration of the joint surface or other soft tissue, which may cause a potential fracture or a higher risk of graft pullout.3,11,12,25
The purpose of this study was to virtually simulate different bone tunnels oriented toward 4 different anatomic landmarks on the lateral malleolus to compare the safe distance that prevents cortical breakthrough during reconstruction of the deep layer of the deltoid ligament (DDL). We hypothesized that a bone tunnel oriented toward the most distal point of the distal fibula would be a safe approach during DDL reconstruction.
Methods
A total of 30 computed tomography (CT) scans of the ankle joint in Han Chinese adults (16 male and 14 female; mean age, 32.7 ± 9.5 years [range, 19-49 years]) who were evaluated between October 2019 and November 2020 were retrieved from the medical image database of our hospital. The inclusion criteria of the study were adults who underwent CT at our institution. The exclusion criteria included patients with ankle deformities, trauma, previous surgical procedures, tumors, and other bony lesions. All the CT scans were obtained at 120 kV and 200 mA with a slice thickness of 0.5 mm by a 64-channel CT scanner (LightSpeed VCT XTe; GE Healthcare), and the scanning time of each slice was 200 milliseconds. The CT scans were used to create a 3D bone model of the ankle joint with Mimics software (Version 18.0; Materialise) for further measurements. The current study was approved by the ethics committee of our hospital, informed consent was obtained for all the patients involved in this study.
The sample size calculation was based on estimates of the mean and standard deviation distance from the tunnel to the surface in a previous study 17 (6.9 and 0.8 mm, respectively). To achieve 80% power to detect a significant difference with an alpha of .05, a total of 21 ankles were required in the current study.
The anatomic footprint of the deltoid ligament on the talus is located at the superior portion of the medial talar body, immediately inferior to the articular cartilage of the trochlea, and is best seen in the middle of the sagittal plane.2,20,27 On the lateral side, 4 palpable anatomic landmarks on the lateral malleolus were located. A tunnel was oriented toward the midlevel of the talar neck, which was the deepest point between the talar head and talar body. 17 The most anterior point was located at the anterior border of the distal fibula. The most distal point was located at the tip of the distal fibula. Finally, the posterior point was identified at the posterior border of the distal fibula. Virtual bone tunnels, all with a diameter of 5 mm and with different lengths (20.0, 25.0, and 30.0 mm), were created, originating from the talar insertion to the different landmarks on the lateral side (Figure 1).

(A) Coronal view and (B) axial view of virtual bone tunnels showing the deltoid ligament insertion on the talus oriented toward different landmarks: *bone tunnel oriented toward the most anterior point of the distal fibula, #bone tunnel oriented toward the most distal point of the distal fibula, ▴bone tunnel oriented toward the most posterior point of the distal fibula, and +bone tunnel oriented toward the talar neck.
The primary study outcome was the shortest distance between the end of the tunnel and the joint surface. To prevent penetration of the joint surface, the shortest distance between the end of the tunnel and the joint surface, for tunnel lengths of 20.0, 25.0, and 30.0 mm and a diameter of 5 mm, was measured using a sphere at the end of the created tunnel (Figure 2). The shortest distance was determined as the largest possible sphere (in 0.1-mm increments) that did not penetrate the bone surface. Tunnels in the 4 different directions were measured for each patient.
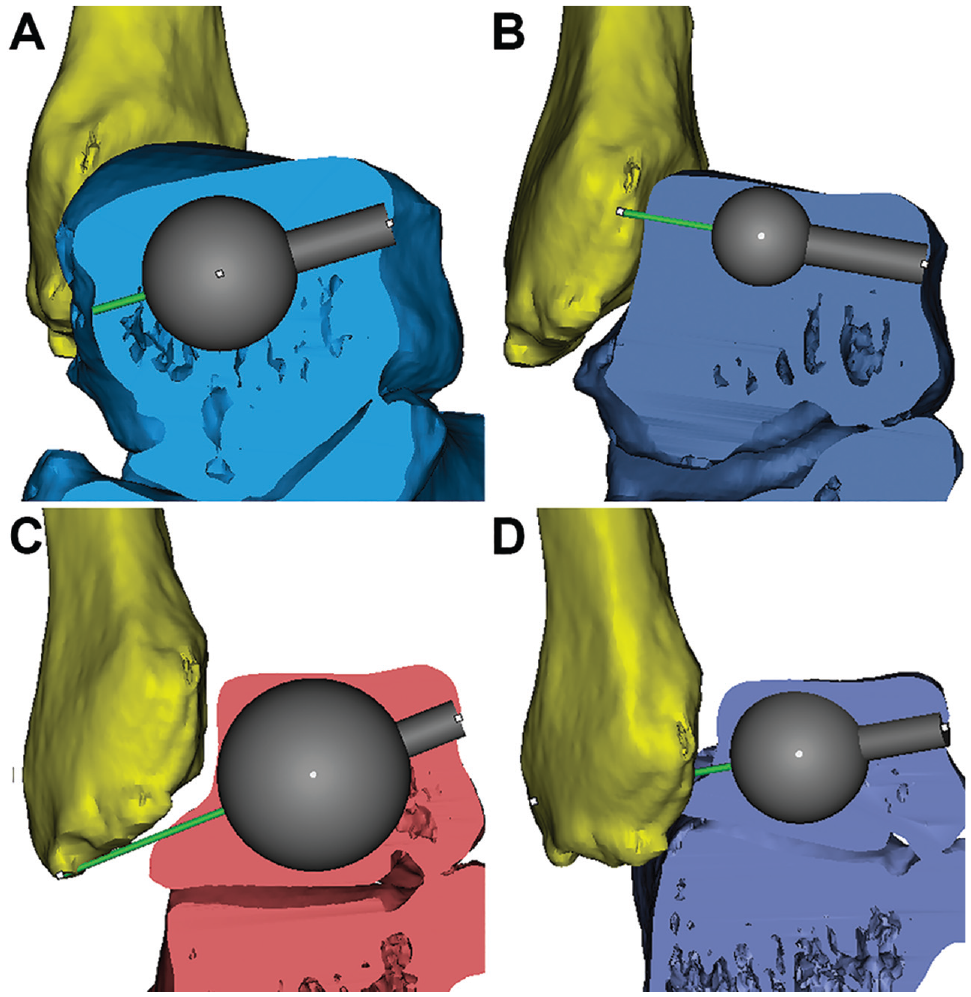
The shortest distance between the end of the tunnel and the joint surface was measured using a sphere at the end of the created tunnel: (A) the tunnel oriented toward the talar neck, (B) the tunnel oriented toward the most anterior point of the distal fibula, (C) the tunnel oriented toward the most distal point of the distal fibula, and (D) the tunnel oriented toward the most posterior point of the distal fibula.
The secondary study outcome was the MSD of a drilling route. To estimate common errors when drilling a pin to a desired landmark, we referred to the study by Michels et al. 17 In their study, the average error angle between the actual drilling route and the planned drilling route was recorded for 10 orthopaedic surgeons, each of whom made 3 attempts. The study found that 60% of the attempts were within 5° of the ideal, while the other 40% were within 10°. 17 Thus, the MSD of a drilling route was calculated by the length of the tunnel, the radius of the tunnel, and a surgical drilling error of 10° (Figure 3).

A diagram illustrating the minimal safe distance (MSD) of a drilling route calculated by the length of the tunnel, the radius of the tunnel, and a surgical drilling error of 10°.
For statistical analysis, the data were expressed as mean ± standard deviation. The nonpaired Student t test was used to detect differences among the safe distances of the 4 different bone tunnels. Differences with a P value <.05 were considered statistically significant. Statistical analyses were processed with SPSS software (SPSS Inc.)
Results
The age, height, and body mass index of the 30 included patients (30 ankles) are compared according to sex in Table 1. There were significant differences between the male and female patients in terms of height (P = .04) and body mass index (P = .01). The MSDs for a tunnel diameter of 5.0 mm, different tunnel lengths, and a surgical drilling error of 10° are shown in Table 2.
Characteristics of Patients According to Sex (n = 30) a

Data are presented as mean ± SD. Boldface P values indicate a statistically significant difference between male and female patients (P < .05).
Minimal Safe Distance for 5 mm–Diameter Tunnel With Different Lengths

For the 20.0 mm–long tunnel, none of the tunnels penetrated the bone surface of the talus. The MSD for a 20.0 mm–long × 5 mm–diameter tunnel was 6.0 mm. The safe distance of the tunnel oriented toward the talar neck (5.90 ± 1.16 mm) did not meet the MSD (Figure 4). The tunnel oriented toward the distal point of the fibula had the longest safe distance compared with the other directions (P < .05).

Comparison of distances for 20.0 mm–long tunnels with respect to the direction of the 4 landmarks. The dashed line indicates the minimal safe distance for a 20.0 mm–long × 5 mm–diameter tunnel (6.0 mm). Error bars indicate standard deviations. *P < .001.
For the 25.0 mm–long tunnel, none of the tunnels penetrated the bone surface of the talus. The MSD for a 25.0 mm–long × 5 mm–diameter tunnel was 6.9 mm. The safe distances of tunnels oriented toward the talar neck (4.53 ± 1.13 mm) and the anterior point of the fibula (5.91 ± 1.52 mm) did not meet the MSD (Figure 5). The tunnel oriented toward the distal point of the fibula had the longest safe distance compared with the other directions (P < .05).

Comparison of distances for 25.0 mm–long tunnels with respect to the direction of the 4 landmarks. The dashed line indicates the minimal safe distance for a 25.0 mm–long × 5 mm–diameter tunnel (6.9 mm). Error bars indicate standard deviations. *P < .001.
For the 30.0 mm–long tunnel, bone cortex penetration was seen in tunnels oriented toward the talar neck (14/30 cases), the anterior point of the fibula (8/30 cases), and the posterior point of the fibula (1/30 cases). The MSD for a 30.0 mm–long × 5 mm–diameter tunnel was 7.8 mm. The tunnel oriented toward the distal point of the fibula had a significantly longer safe distance compared with the other directions (6.77 ± 2.11 mm) (P < .05), but it did not meet the MSD (Figure 6).

Comparison of distances for 30.0 mm–long tunnels with respect to the direction of the 4 landmarks. The dashed line indicates the minimal safe distance for a 30.0 mm–long × 5 mm–diameter tunnel (7.8 mm). Error bars indicate standard deviations. *P < .001.
Discussion
In the current study, we investigated safe landmarks for drilling a bone tunnel at the talar insertion of the DDL. For each bone tunnel, the safe distance to 4 landmarks (the talar neck and the anterior, distal, and posterior points of the distal fibula) was measured to find a relatively safe pathway to create a talar tunnel for DDL reconstruction. Talar tunnels of 20.0 mm in length and 5 mm in diameter, oriented toward the most anterior point (tunnel length: 7.27 ± 1.50 mm), the most distal point (tunnel length: 11.64 ± 1.16 mm), and the most posterior point (tunnel length: 10.16 ± 1.10 mm) of the distal fibula, were safe for DDL reconstruction. Talar tunnels of 25.0 mm in length, oriented toward the most distal point (tunnel length: 8.99 ± 1.94 mm) and the most posterior point (tunnel length: 7.57 ± 1.82 mm) of the distal fibula, were safe for DDL reconstruction. Bone cortex penetration was found in 30.0 mm–long tunnels oriented in all 3 directions.
The deltoid ligament is a complex structure that spans from the medial malleolus to the navicular, talus, and calcaneus. 2 It is the primary medial stabilizer of the ankle joint and limits valgus tilt and anterior translation of the talus.9,18 The deltoid ligament is separated into superficial and deep layers by a fat pad.4,6 The superficial layer has 4 components: the tibionavicular ligament, the tibiospring ligament, the tibiocalcaneal ligament, and the superficial posterior tibiotalar ligament. 2 The deep layer consists of 2 parts: the anterior tibiotalar ligament (not always present) 27 and the deep posterior tibiotalar ligament (always present). 2 The deep posterior tibiotalar ligament is larger and thicker than the other 5 structures of the deltoid ligament. 2 Biomechanical studies have demonstrated that the loss of the DDL would result in excessive external rotation and lateral shift of the talus.13,16 These changes in biomechanics may lead to overloading of the lateral tibiotalar joint and subsequent cartilage lesions. 7
Some case series and case reports have been published regarding reconstruction of the DDL by drilling a bone tunnel at the talar insertion.1,5,12,19 The tunnels used in previous reports were aimed in various directions, including toward the talar neck, or were parallel to the dome of the talus. To our knowledge, no publications have evaluated the safety of the bone tunnel at the talus or measured the MSD of bone tunnels. Safe bone tunnels can avoid potential fractures, cartilage lesions, graft loosening, or other soft tissue injuries.3,21,25 A bone tunnel oriented toward the talar neck poses a risk of talar neck fractures. 23 An orientation toward the most anterior point of the distal fibula increases the risk of damaging the sinus tarsi. A bone tunnel oriented toward the most posterior point of the distal fibula poses a higher risk of damage to the neurovascular bundle and the peroneus longus tendon. 22 The diameter of tunnels ranged from 4.5 to 6 mm and the depth from 15 to 20 mm. Different sizes of the bone tunnel may cause potential risks of penetrating the joint surface or talar bone cortex. Higashiyama et al 12 used autologous hamstring tendons with diameters from 4.5 to 5.5 mm to reconstruct the anterior tibiotalar ligament. A talar tunnel was created at the talar footprint, which was located inferior to the articular cartilage of the talar trochlea. The tunnel was aimed toward the lateral side of the talar neck, which was confirmed by intraoperative fluoroscopy. A more anterior footprint position at the anteromedial corner of the trochlea may provide stronger control for anterior drawer stress and external rotation stress. In a patient series of chronically failed deltoid ligaments, Deland et al 5 used autologous peroneus longus tendons to reconstruct the DDL. The direction of the tunnel was parallel to the dome of the talus, angled slightly plantar to dorsal from the lateroinferior talar neck to the center of rotation in the talus medially. In a case report of autologous DDL reconstruction, Pisanu et al 19 drilled a 5 mm–diameter tunnel in the medial nonarticulating portion of the talus at the native footprint of the anterior tibiotalar ligament, and the free tendon was fixed with a 4.75-mm interference screw.
Several studies have been published to investigate the biomechanics of DDL reconstruction.11,26 Haddad et al 11 found similar eversion and external rotation stability with DDL reconstruction using either the anterior tibial tendon or an intact deltoid ligament. A bone tunnel was created in the center of the DDL footprint, from medial to lateral within the body of the talus. Tunnels were created 1 mm greater than the graft size for ease of graft passage. In a finite element analysis for the biomechanical evaluation of deltoid ligament reconstruction, Xu et al 26 compared external rotation and talar tilt using different reconstruction techniques (including the Wiltberger, Deland, Kitaoka, and Hintermann techniques). That study showed that the Deland technique (tendon graft from the medial talus to the tip of the medial malleolus) and the Kitaoka technique (tendon graft from the medial cuneiform to the medial malleolus) resulted in better rotational stability and less ligament stress compared to the other methods.
In the current study, we measured tunnels with different lengths (20.0, 25.0, and 30.0 mm). The tunnel oriented toward the talar neck had the highest risk of bone perforation for different tunnel lengths from 20.0 to 30.0 mm and thus should not be considered a potential option. The tunnels with lengths of 20.0 and 25.0 mm, oriented toward the most posterior point or the most distal point of the distal fibula, had safe distances greater than the MSD. However, the orientation toward the most posterior point of the distal fibula ran close to the peroneal tendons, which may be injured when inserting a guide pin. Based on the above findings, we recommend using a 20.0 mm– or 25.0 mm–long bone tunnel oriented toward the most distal point of the distal fibula at the talar footprint of the DDL. All the 30.0 mm–long tunnels carried a significant risk of perforation in 3 different directions. Such a long bone tunnel should be avoided in DDL reconstruction. Thus, we suggest a safe orientation toward the most distal point of the distal fibula for bone tunnel creation and screw insertion in DDL reconstruction. Tunnels oriented toward the other 3 landmarks pose a higher risk of damaging the talar neck, the sinus tarsi, the neurovascular bundle, and the peroneus longus tendon.
Limitations
This study is not without limitations. First, all the CT scans were from a Han Chinese population. Differences might exist in other populations regarding bone size or bone morphology. Second, the sample size of 30 might not be large enough to eliminate selection bias. In an anatomic study of the anterior talofibular ligament, a sample size of 12 patients was used to evaluate the safety of created tunnels 17 . Finally, the 3D measurements did not consider soft tissue, including the neurovascular bundle, ligaments, or cartilage, among others. Further studies including bone tissue and soft tissue would provide more accurate conclusions for safe tunnels. Future studies with a larger sample size are needed to provide more solid results.
Conclusion
The findings of the current study indicate that talar tunnels of 20.0 and 25.0 mm in length and 5 mm in diameter, oriented toward the most distal point or the most posterior point of the distal fibula, were safe for DDL reconstruction. We recommend a shorter and blind-ended tunnel oriented toward the most distal point, which has a lower risk of irritating surrounding soft tissue. Tunnels of 30.0 mm in length should be avoided in any situation.
Footnotes
Final revision submitted May 19, 2023; accepted June 6, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Huashan Hospital (No. KY2020-1299).