
Abstract
Background:
Little is known about the specific risk of knee injuries due to trampoline accidents in adults compared with children.
Purpose:
To investigate the differences in trampoline-related knee injuries between children and adults and identify risk factors and protective strategies to reduce injury incidence.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Data on 229 consecutive patients treated for trampoline-related knee injuries in a single institution were prospectively collected, analyzed, and included. Risk factors, injury patterns, and clinical treatments were compared between skeletally immature and skeletally mature patients. Logistic regression was used to determine the odds ratios for specific risk factors for trampoline-related injuries—including body mass index (BMI), trauma mechanism, patient age, and accident location.
Results:
A total of 229 patients met the inclusion criteria; 118 (52%) patients (women, 54.2%; mean age, 8.5 ± 4.1 years) were skeletally immature at the time of injury, and 111 (48%) patients (women, 72%; mean age, 31.9 ± 13.1 years) had closed physes on initial presentation and were classified as skeletally mature. A total of 63 patients (28%) required surgical treatment for their knee injury. Overall, 50 anterior cruciate ligament (ACL) tears, 46 fractures, 39 meniscal tears, 31 ligamentous tears other than ACL, 22 patellar dislocations, and 38 soft tissue injuries, such as lacerations, were recorded. Skeletally mature patients had 7.8 times higher odds (95% CI, 1.6-46.8; P < .05) and 19.1 increased odds (95% CI, 5.5-74.9; P < .05) of an ACL tear or another ligamentous tear, respectively, compared with skeletally immature patients. Patients who described instability and giving way of the knee as relevant trauma mechanisms had odds of 3.11 (95% CI, 0.9-14.8; P < .05) of an ACL tear compared with other trauma mechanisms. Meniscal tears were observed more frequently in the skeletally mature cohort (P < .05). An elevated BMI was associated with a significantly higher relative risk of an ACL tear, a ligamentous tear other than the ACL, and an injury requiring surgery. A third of surgically treated patients were subject to a delayed diagnosis.
Conclusion:
Adults had a significantly increased risk of ligamentous and meniscal tears and required operative intervention more often than skeletally immature individuals. Elevated BMI, age, and instability events in terms of trauma mechanism conveyed an increased risk of structural damage to the knee.
Recreational trampoline use is gaining popularity, reflected in rising sales of private trampolines and the opening of new trampoline centers. 18 However, trampoline injuries have become a major public health concern in the United States (US). 31 According to the US Centers for Disease Control and Prevention (CDC), 24 more than 1 million people were treated in US emergency rooms for trampoline-related injuries in 2018. Trampoline injuries accounted for more than $1 billion in medical costs and almost 100,000 pediatric emergency visits in the United Kingdom. 33 Most injuries occurred in children aged 6 to 17 (71%) in a nationwide study conducted in the Republic of Korea. 11 This highlights the global scope and implication of the problem.
Using hospital admission data, injury surveillance systems have concluded that trampoline-related injuries lead to more hospitalizations than injuries stemming from other popular sports or recreational activities. 8 In response to the socioeconomic impact of trampoline injuries, the American Academy of Pediatrics, the American Academy of Orthopedic Surgeons, and the Canadian Pediatric Society have issued policy statements advising against the recreational use of home trampolines.4,8 Despite these recommendations and the development of safer trampoline designs, rates of trampoline injuries remain high.5,20
While life-threatening injuries are rare in trampoline jumping, the most common trampoline-related injuries include fractures (35%), strains and sprains (28%), and cuts and lacerations (15%) of the upper and lower extremities. 24 Most accidents occur at home on backyard trampolines, and most injuries sustained do not require hospital treatment or further medical attention, potentially leading to a high rate of underreported injuries.9,27,31 However, injuries that lead to a hospital visit frequently require surgical treatment. 24
The knee is the body part most commonly injured due to collisions, falls, and overuse occurring from sports. 2 However, little is known about trampoline-related knee injuries in skeletally immature and mature patients and possible differences in injury patterns and severity. Although there are some general epidemiological studies of trampoline injuries, none provide a detailed analysis of knee injuries. 18 In this study, we investigated the differences in trampoline-related knee injuries between children and adults. We aimed to identify risk factors and protective strategies to reduce the incidence of injuries. We hypothesized that skeletally mature trampoline users would be more likely to sustain severe knee injuries and undergo surgery more frequently than skeletally immature individuals.
Methods
Study Population and Design
This cohort study explored knee injuries sustained on a trampoline among skeletally immature and mature patients. Institutional review board approval was obtained before starting the study. Data on all trampoline-related knee injuries treated at a single institution (Mayo Clinic) from 1997 to 2022 were analyzed. The Mayo Clinic is the only Level I/II trauma center in Olmsted County Minnesota, US, and the 6 adjacent counties in Southeastern Minnesota, where the majority of patients come from. On average, 20% of patients seen in the emergency department (ED) are children. The Mayo Clinic serves Olmsted County, with a population of 163,436 in 2021, including about 40,000 persons <18 years. The ED at our quaternary care academic institution has a volume of approximately 77,000 annual patient visits. 19 A search of the institutional medical records database was performed to identify all patients treated for trampoline-related knee injuries. Inpatient and outpatient data were collected from the hospital and the ED. Patients were included if they had a documented trampoline accident with a consecutive knee injury as the reason for the hospital presentation. Accordingly, 229 of 403 patients were enrolled in this study. A total of 174 patients were excluded because of a nontrampoline-related trauma mechanism (Figure 1).

Flowchart displaying patient selection for the study.
Patient and clinical information was gathered from medical records and charts. The body mass index (BMI) was adjusted by age. For patients <20 years, the BMI Calculator for Children and Teens provided by the CDC was used to calculate the BMI. For patients ≥20 years, the Adult BMI Calculator was used. 17 Skeletal maturity was assessed using preoperative magnetic resonance imaging (MRI) based on the status of the growth plate closure. Patients with open growth plates and closing but not closed growth plates were considered skeletally immature. Patients with closed growth plates were considered skeletally mature. MRI was available in all patients with documented ligamentous and meniscal injuries. If no MRI was available, a conventional radiograph was used to assess skeletal maturity. A fellowship-trained orthopaedic surgeon (M.H.) reviewed all radiographic studies.
Injury Injury documentation included the patient’s age, sex, localization, and diagnosis. Personal data on each patient, accident circumstances, time of admission to the hospital, body part injured, treatment, and number of days in the hospital were recorded prospectively. The precise documentation of the knee injury included lesions of the lateral collateral ligament, medial collateral ligament, anterior cruciate ligament (ACL), posterior cruciate ligament (PCL), lateral meniscus, and medial meniscus. All injured knees were clinically examined regarding pain, swelling, range of motion, stability, and meniscus pathology. The clinical examination followed a radiographic evaluation (anteroposterior, lateral, and merchant view) regarding joint deformation and fractures of the femur, patella, and tibia. If the clinical findings remained doubtful or required further investigation, patients were transferred for an MRI examination of the knee. Skeletal maturity was assessed by analysis of radiographic studies from the timepoint of injury and initial presentation.
Statistical Analysis
Descriptive statistics—including mean, standard deviation, and range—were used to characterize results with continuous values, while percentages were used for proportions. Demographic characteristics and surgery details were compared between groups using the Wilcoxon rank-sum test for continuous variables (age, BMI, lesion size, number of implants) and the Fisher exact test for categorical variables (sex, skeletal maturity, treatment type, trauma mechanism, location of accident). A univariate logistic regression model was used to analyze the risk for ACL tears, other ligamentous tears, meniscal tears, and surgical treatment conveyed by patient-specific and procedural parameters. The model equation used for univariate logistic regression was as follows: logit(p) = b0+b1×x, where:
logit(p) is the natural logarithm of the odds of the binary response variable being equal to 1, given the value of the predictor variable (ie, the independent variable).
b 0 is the intercept term or constant, representing the log odds of the binary response variable being equal to 1 when the predictor variable is equal to 0.
b 1 is the coefficient or slope, representing the change in log odds of the binary response variable being equal to 1 for a 1-unit increase in the predictor variable.
x is the predictor variable.
Within each group, other risk factors for the above endpoints were assessed using odds ratios (ORs), the Fisher exact test for dichotomous variables, and nominal logistic fit models for continuous or ordinal variables. A Pearson product-moment correlation analysis was used to measure the linear correlation between skeletal maturity and ligamentous tears. Coefficient (r) values can range from +1 to −1, where +1 indicates a perfect positive relationship, –1 indicates a perfect negative relationship, and 0 indicates no relationship. P < .05 was defined as significant. All statistical analyses were performed using SPSS Statistics for Windows Version 28.0 (IBM). Graphics were designed with SPSS Statistics for Windows Version 28.0) and Excel Version 2021 (Microsoft).
Results
Patients
In the present study, we included 229 patients with a mean age of 19.9 ± 15.1 years at the time of injury. There were 118 skeletally immature and 111 skeletally mature patients. Also, 15% were <6 years, 27% were aged between 6 and 12 years, and 21% were between 12 and 18 years at the time of injury (Figure 2). The age range was 1 to 68 years. The cohort comprised 84 male (36.7%) and 145 female (63.3%) patients (Table 1).

Age distribution of included patients. Most patients were between 7 and 12 years, followed by patients ≥37 years.
Patient Characteristics (N = 229) a
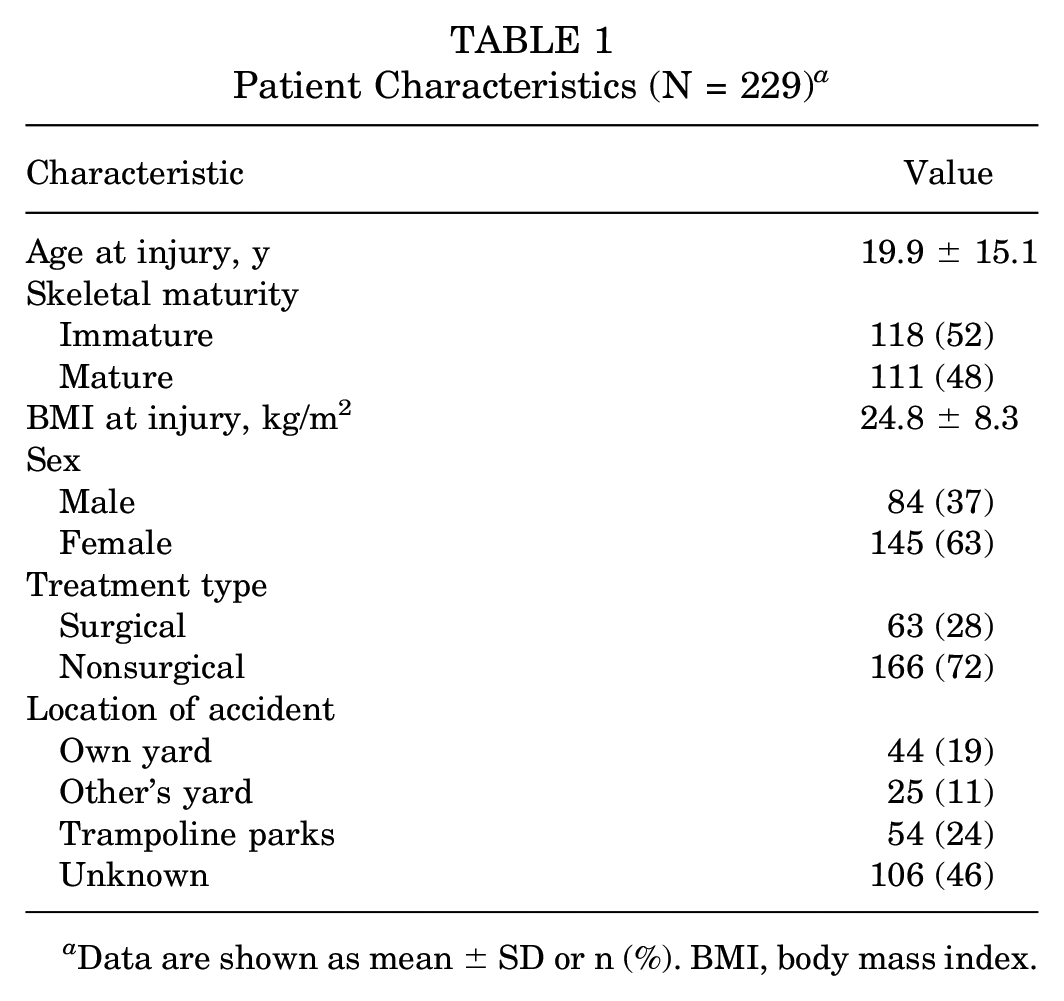
Data are shown as mean ± SD or n (%). BMI, body mass index.
Study Groups
The skeletally immature cohort had a mean age of 9 ± 4 years and comprised 118 patients. The mean BMI was 19.4 ± 4.7 kg/m2, and there were 64 female and 54 male patients. The skeletally mature cohort included 111 patients, with a mean age of 30 ± 13 years at the time of injury. The BMI was significantly higher than in their immature counterparts (30.6 ± 7.4 kg/m2), and there was a higher percentage of women (73%) (Table 2).
Characteristics of the Study Groups a

Data are presented as mean ± SD or n (%). BMI, body mass index; NS, not significant.
Comparison between yards and trampoline parks.
Accident Location
The accident location differed significantly between the groups. Most accidents in the skeletally immature cohort occurred on a trampoline in the patient's backyard. Skeletally mature patients sustained injuries in commercial trampoline parks in almost one-third of cases (P < .05). The rate of accidents in a neighbor's yard did not differ between the groups. In 46.3% of cases, the exact location of the trampoline accident remained unknown.
Time of Accident
The first trampoline-related knee injury was noted in 1997. There were between 0 and 5 incidents registered annually until 2017 when 16 knee injuries were treated. The number of injuries increased in the following years, reaching a temporary peak in 2021, with 49 incidents (Figure 3).
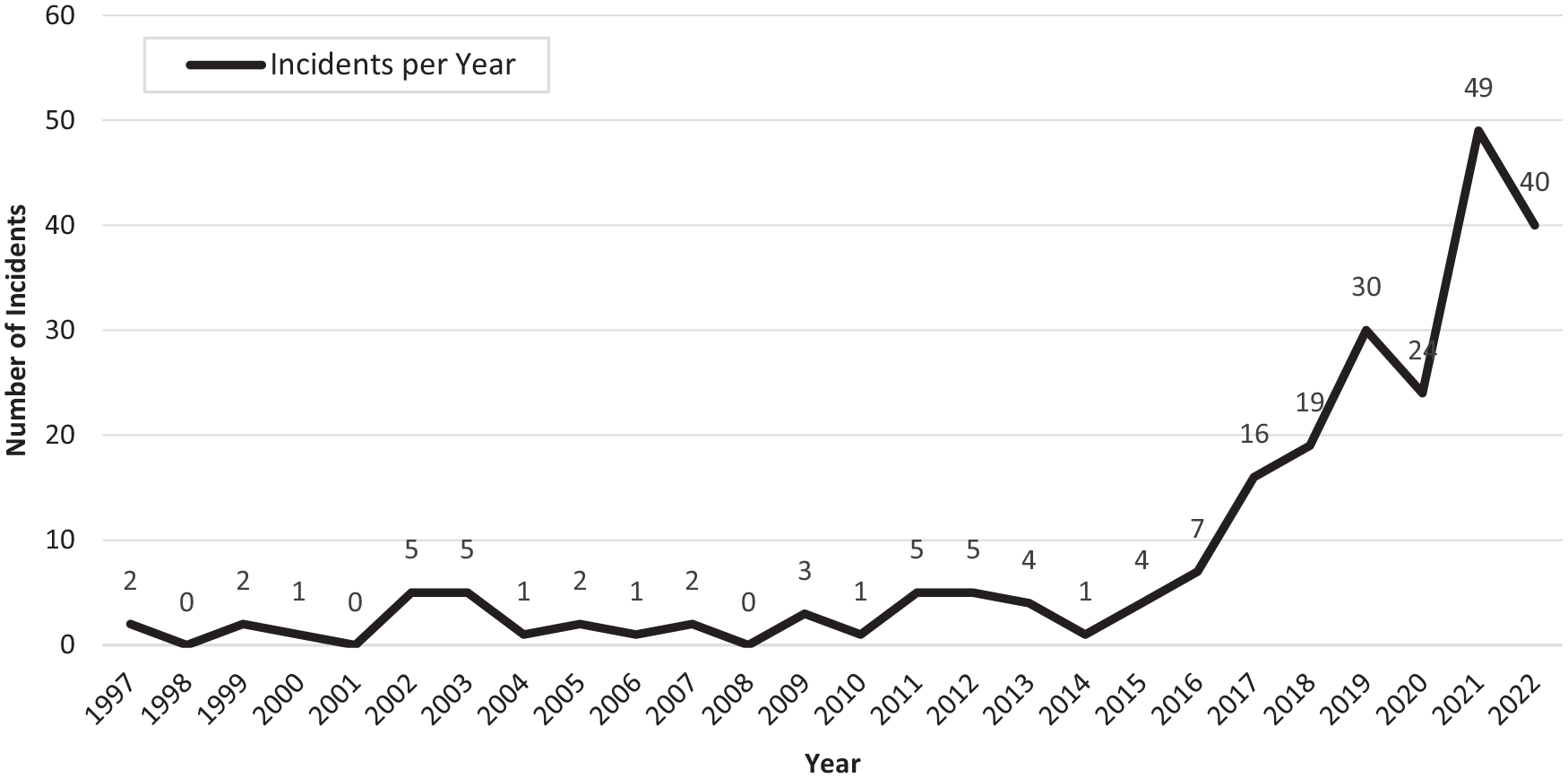
Incidence of trampoline-related knee injuries per year. While there were few injuries from 1997 to 2016, the incidence rose substantially beginning in 2017 and has continued to rise.
Trauma Mechanism
Overall, 38% of skeletally immature patients reported a direct collision with a hard object such as exposed trampoline springs or an item brought onto the trampoline as cause of injury. A crash with another person within the trampoline was responsible for injury in 9% of cases. Skeletally mature patients reported a sudden pivoting or cutting maneuver in 65% of cases with a flexed knee that resulted in giving way and an instability of the knee. An ejection from the mat with a consequent fall on the ground was reported in 5.1% and 11.7% of cases, respectively (Table 2).
Type of Injury and Treatment
There were 128 injuries in the skeletally immature cohort. The most frequent type of injury was a fracture diagnosed in 31% of skeletally immature patients, followed by muscle strains (25%), soft tissue injuries, such as lacerations (21%), and patellar dislocations (14%). ACL tears (2.5%), PCL tears (2.5%), and meniscal tears (6%) were less frequent in the young cohort. The injury frequencies in the skeletally mature cohort differed significantly. ACL tears were diagnosed in 47 patients (42%), followed by muscle strains (30%), meniscal tears (29%), and ligamentous tears other than the ACL and PCL (20%) (Table 3).
Incidence of Injury a

Data are shown as n (%). Percentage values exceed 100% because of patients who sustained ≥2 injuries. ACL, anterior cruciate ligament; NS, not significant; PCL, posterior cruciate ligament.
Of the skeletally immature patients, 14 (11.9%) underwent surgery as a consequence of their trampoline-related knee injury, while 49 (44.1%) patients were treated surgically in the mature cohort (P < .05). Children were primarily subject to open/closed reduction and internal fixation of a fracture. Of note, only 10% of registered fractures had to be treated surgically. An ACL reconstruction was performed in 3 skeletally immature cases, while 38 skeletally mature (34%) patients underwent ACL reconstruction (P < .05). Meniscal tears were repaired in 2 children and 12 mature patients (P < .05) (Table 4). The hospitalization rate was low, and only 1 patient in the present study was admitted as an in-patient. He was treated for a complete bilateral patellar tendon rupture and could not ambulate on his own because of the bilateral nature of his injury.
Incidence of Surgery a

Data are shown as n (%). ACL, anterior cruciate ligament; MCL, medial collateral ligament; MPFL, medial patellofemoral ligament; NS, not significant; OCA, osteochondral allograft transplantation; PCL, posterior cruciate ligament.
Time From Accident to Surgical Treatment
The mean time from injury to surgical treatment was 192 ± 387 days. Also, 16 patients (25.4%) of the surgical cohort attempted nonsurgical treatment and were later converted to surgical treatment because of persisting symptoms. Nine patients sustained an ACL tear that was initially treated conservatively but converted to ACL reconstruction after a mean of 10.3 months. Seven patients with a meniscal tear were initially treated nonoperatively but experienced prolonged pain and were therefore converted to surgical treatment. All of these patients were skeletally mature at the time of diagnosis.
Risk Analysis
Skeletal maturity was associated with an increased ORs of 7.8 (95% CI, 1.6-46.8; P < .05) for an ACL tear, of 19 (95% CI, 5.4-74.9; P < .05) for a ligamentous tear, and of 4.6 (95% CI, 1.5-14.5; P < .05) for an injury that required surgery. Skeletal immaturity was associated with increased odds of 3.9 (95% CI, 1.79-8.38; P < .05) for a fracture. A BMI ≥30 kg/m2 was associated with significantly increased odds for an ACL tear (OR, 3.81 [95% CI, 2.53-4.95]; P < .05), a ligamentous tear (OR, 5.48 [95% CI, 0.09-8.59]; P < .05), a meniscal tear (OR, 4.01 [95% CI, 2.84-5.79]; P < .05), and for surgery (OR, 4.69 [95% CI, 3.19-7.14]; P < .05) in the general cohort. A reported trauma mechanism of pivoting and resulting giving way and instability carried increased odds for an ACL tear (OR, 3.11 [95% CI, 0.9-14.8]; P < .05), another ligamentous tear (OR, 7.46 [95% CI, 2.41-28.66]; P < .05), and surgery (OR, 3.62 [95% CI, 1.4-10.65]; P < .05) when compared with other trauma mechanisms combined (Table 5). The results of the correlation analysis showed a positive correlation between skeletal maturity and ligamentous tears, with an r value of 0.52 (OR, 0.52 [95% CI, 0.42-0.61]; P < .05).
Results of Univariate Regression for Clinically Relevant Outcomes based on Patient-Specific Variables a

Bold P values indicate significance. ACL, anterior cruciate ligament; BMI, body mass index; OR, odds ratio.
Discussion
Trampolines are a popular recreational activity and a significant source of injury, particularly to the knee. We assessed trampoline-related knee injuries among skeletally immature and mature patients in the present study. The main finding of this study was discovering a significant correlation between skeletal maturity and ligamentous and meniscal tears. Older patients had an increased risk of ligamentous, meniscal, and bony injuries.
These findings support the initial hypothesis that there would be an increased incidence of fractures in the pediatric population and an increased incidence of ligamentous and meniscal injuries among skeletally mature patients with trampoline injuries. They further highlight the importance of considering the differences in musculoskeletal development between skeletally immature and mature patients when treating trampoline-related knee injuries.
Recreational trampoline jumping has gained popularity not only in the US but also around the world. Trampoline-related injuries were studied in Asia, Australia, France, and Austria, reporting similar trends in injury presentation, with extremity injuries being the most prevalent.6,12,15,25,29 A recent study reported an incidence of lower extremity injuries of 34% among all trampoline injuries, without discriminating specific injury characteristics or anatomic regions such as ankle, knee, or hip. 29
In this study, most injuries among skeletally mature patients were sustained in trampoline parks, while skeletally immature patients were most often injured on backyard trampolines. This finding correlates with the results of a recent meta-analysis. 18 Additionally, the characteristics of injuries differed between those sustained on backyard trampolines and those sustained in trampoline parks, suggesting a different pattern of injuries in these 2 settings, particularly among the skeletally mature population. This may relate to structural differences between the trampoline mats used in home trampolines and those used in trampoline centers. 18 The increased tensile strength used in commercial trampoline center mats may produce a more energetic bounce, amplifying the loading in bones, ligaments, and menisci.3,20,23 Moreover, it is not uncommon for multiple individuals to use the same mat in trampoline parks, resulting in high-energy collisions. 3 This observation was validated by computational biomechanical modeling simulating 2 simultaneous trampoline users and showing kinetic energy transfer from the larger to the smaller mass, especially when bouncing was out of phase. 14 This increased energy transfer and impact might contribute to the increased severity of injuries sustained in a trampoline park.
While the number of trampoline-related knee injuries increased constantly from 2014, a significant peak was noted in 2021 with a jump in incident numbers of >100%. It can be assumed that the COVID-19 pandemic contributed to this peak. 28 With restrictions on social gatherings, the closure of gyms and playgrounds, and limited outdoor options, many people turned to home-based activities for entertainment and exercise. 7 Trampolines became an increasingly popular choice when people were encouraged to stay home to reduce the spread of the virus. 28 This led to reduced opportunities for physical activity, particularly for children and adolescents. Trampolines offered an attractive alternative that allowed individuals to engage in active play and exercise within the confines of their homes. 21 However, the lack of structured supervision and safety protocols in professional settings like gyms or supervised playgrounds likely increased the risk of injuries. The demand for trampolines surged and resulted in a significant increase in trampoline ownership and an influx of new jumpers who were not accustomed to trampolines or were not properly trained, potentially leading to increased injuries. 28 Moreover, extended periods of lockdowns and reduced physical activities resulted in a decline in overall physical fitness and conditioning. 21 When individuals, particularly children, suddenly engage in vigorous physical activities like jumping on a trampoline without adequate preparation, their bodies may be more susceptible to injuries. 21 Weak muscles, decreased coordination, and reduced flexibility can increase the likelihood of accidents and lead to more severe injuries. 10
Skeletal injuries are common among different age groups, but the specific weak links within the musculoskeletal system can vary. In skeletally immature and skeletally mature patients, the weak link refers to the structure most susceptible to injury. In skeletally immature patients, the physis is the primary weak link because of its unique anatomic and physiological properties. It is susceptible to injury because it is the weakest part of the long bone structure. During periods of rapid growth, the physis is particularly vulnerable to shearing, compression, and avulsion forces, which can result in physeal injuries such as fractures or disruptions. In contrast to skeletally immature patients, skeletally mature individuals have fully developed growth plates, making the physis less susceptible to injury. Instead, the weak link in this population often shifts to the ACL, which is susceptible to injury during activities involving rapid changes in direction, deceleration, or direct trauma.
Across all age groups, there was a mean time from trampoline accident to surgical treatment of 192 days. This prolonged time was partly because of patients initially opting for nonsurgical treatment and later being converted to surgical intervention because of persisting symptoms. However, one-third of surgical patients were subject to a delayed surgically relevant diagnosis, extending the time to treatment and possibly facilitating further joint damage. This high rate of overlooked injuries can be attributed to the status of the study center as a Level I trauma center and center of expertise, in many cases consulted by patients to seek a second opinion.26,32
The risk of sustaining trampoline-related knee injuries increased with age. Older children, adolescents, and adults were at greater risk for injuries requiring surgery. As previously reported, this might be due to a higher appetite for risky behavior in preteens and teenagers.1,16 An additional possible influential parameter is the increasing BMI with age, which is associated with increased kinematic energy impact on bones and joints, leading to an increased injury rate. 22 Increased body mass of patients remains a risk factor for ligamentous knee injuries. In agreement with the current literature, the present study also found that obese individuals were significantly more likely to have an ACL tear caused by pivoting mechanisms versus those with a BMI <25 kg/m2 (P < .05). A total of 30 patients had a BMI ≥35 kg/m2, and 16 patients of this subgroup (accounting for 53.3%) required surgical treatment for 14 ACL tears, 12 meniscal tears, and 3 fractures, among other indications.
Furthermore, this study highlights the need for improved safety measures to prevent trampoline-related knee injuries. The high frequency and often severe nature of these injuries underscore the need for better education and awareness among trampoline users and parents of young children. Furthermore, developing and using safer trampoline designs may help reduce the incidence of injuries due to direct collisions with hard objects. Last, the presented data suggest that older individuals with an elevated BMI should use caution when engaging in recreational trampoline activities. 30
Trampoline-related knee injuries are a significant hazard for knee injuries among both children and adults. Proper supervision and safety measures, including adequate preparation and training before jumping activity, are essential to prevent injuries and reduce their incidence. 13
Limitations
There are limitations to this study, including its retrospective design, which is subject to selection bias. Consequently, only patients with knee injuries from trampoline-jumping were included, and no controls were available. Therefore, we reviewed all trampoline-related injuries treated at our institution, including all cases involving the knee, without excluding any knee injuries. However, this is a single-center study conducted at a Level I trauma and referral center, and the results may not apply to the broader population and therefore may not be generalizable. Further, because of the retrospective nature of the study, patient records may have been incomplete.
A second limitation of the present study is that it relies on the quality and completeness of the data and records used. If the data are incomplete or inaccurate, it can affect the reliability and validity of the study's results. We addressed this issue by following up with patients by phone interviews in case of missing relevant information.
Third, this study was designed as a cross-sectional study; thus, no follow-up patient data can be provided. As a result, it remains to be investigated what the mid- and long-term consequences of trampoline-related knee injuries are for patients, health care systems, and society. These limitations should be considered when interpreting the results of the present study.
Conclusion
Trampoline accidents frequently lead to injuries to the knee that often require surgical treatment. Adults have a significantly increased risk of ligamentous and meniscal tears and require operative intervention more often than skeletally immature individuals. Elevated BMI, age, and instability events in terms of trauma mechanism convey an increased risk for structural damage of the knee. Orthopaedic surgeons and staff in the ED should be aware of the high rate of severe knee injuries after trampoline accidents to lower the number of initially overlooked injuries.
Footnotes
Final revision submitted May 31, 2023; accepted June 7, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Foderaro-Quattrone Musculoskeletal-Orthopaedic Surgery Research Innovation Fund. M.H. has received funding from the Deutsche Forschungsgemeinschaft (466023693). M.J.S. has received royalties from Arthrex, nonconsulting fees from Arthrex, consulting fees from Arthrex; and research support from Stryker. T.M. has received consulting fees from OrthoPediatrics, Medtronic, and Zimmer Biomet Holdings. B.A.L. has received nonconsulting fees from Arthrex, consulting fees from Arthrex, and royalties from Arthrex. A.J.K. has received consulting fees from Arthrex, JRF Ortho, Vericel, and Responsive Arthroscopy; nonconsulting fees from Arthrex; hospitality payments from Gemini Mountain Medical and Smith & Nephew; royalties from Arthrex and Responsive Arthroscopy; research support from DJO, Arthrex, Arthritis Foundation, Ceterix, Histogenics, and Aesculap; honoraria from JRF Ortho, Vericel, and MTF Biologics; and is a board or committee member of MTF Biologics. D.B.F.S. has received consulting fees from Smith & Nephew and research support from JRF Ortho. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Mayo Clinic (No. PR15-000601-06).