
Abstract
Background:
There are little published data on return to sports (RTS) after reverse total shoulder arthroplasty (RTSA).
Purpose:
To (1) determine the rate and timing of RTS after RTSA in an Asian population, (2) analyze predictive factors for RTS, and (3) determine the relationship between RTS after RTSA and clinical/radiological outcomes.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A retrospective review was performed on consecutive patients with diagnosis of irreparable rotator cuff tear (RCT), cuff tear arthropathy (CTA), or degenerative osteoarthritis who underwent RTSA between May 2017 and May 2020. Included were patients who played sports preoperatively in ≤3 years and had ≥2-year follow-up. Patients were divided into 2 groups based on responses to a telephone survey about RTS after RTSA: those who returned to sports (group A) and those who did not (group B). Patient characteristics, pre- and postoperative clinical features and functional scores, and radiologic outcomes (acromial fracture, scapular notching, heterotopic ossification, and loosening of humeral and glenoid component) were compared between the groups.
Results:
Of 59 eligible patients, 44 patients (28 in group A, 16 in group B) were included. The RTS rate after RTSA was 63.6%, and the mean RTS time was 9.1 months (range, 3-36 months). There was a significant group difference in body mass index (BMI) (group A, 24.3 ± 2.1; group B, 27.1 ± 4.4; P = .01) and preoperative diagnosis (CTA/irreparable RCT/degenerative osteoarthritis diagnoses: group A, 13/12/3; group B, 3/6/7; P = .03). Patients in group A showed significantly higher forward flexion (P = .03) and higher Simple Shoulder Test score (P = .02) than group B at final clinical follow-up. No significant difference in radiological outcomes was found between the groups.
Conclusion:
Patients with a low BMI and those diagnosed with CTA or irreparable RCT were found to have better RTS rates after undergoing RTSA, and forward flexion and Simple Shoulder Test scores at final follow-up were significantly higher in the RTS group, with no significant differences in complications.
Reverse total shoulder arthroplasty (RTSA) is a well-established treatment option for patients with rotator cuff–deficient osteoarthritis. 14 Over the past decades, indications for RTSA have been expanded to proximal humeral fracture, irreparable rotator cuff tear (RCT) without glenohumeral osteoarthritis, primary osteoarthritis with glenoid bone loss and intact rotator cuff, and infections.3,19,21,37,38 More RTSA procedures are performed globally as the indications extend to younger patients and the active elderly population.9,36,42 Therefore, clinicians should focus not only on pain or daily activity but also on the ability to resume sports activity after RTSA because the expectation for sports activity after RTSA is increasing. 25 When clinicians advise patients to undergo RTSA in outpatient clinics, patients often ask whether it is possible to resume their sports activities.
Several studies have been published about return-to-sports (RTS) activity after hip arthroplasty, knee arthroplasty, and total shoulder arthroplasty with successful results. § However, there are few studies on RTS activity after RTSA.5,11,25,44,46 From the current studies, it is unclear as to how to predict the probability and appropriate timing of RTS activities after surgery.13,33 Moreover, the types of sports played are likely to be different across different cultures/ethnicities.
The purpose of this study was to (1) assess the rate and timing of RTS after RTSA to provide reliable information for clinicians before the surgery from Asian perspective, (2) analyze factors associated with RTS after RTSA, and (3) determine the relationship between RTS after RTSA and clinical/radiological outcomes.
Methods
Study Participants
This study was approved by the institutional review board of our institution. The requirement for informed consent was waived because of the retrospective design of the study. We performed a retrospective review of prospectively collected data of 213 consecutive patients who underwent RTSA from May 2017 to May 2020. The study inclusion criteria were (1) diagnosis of cuff tear arthropathy (CTA), degenerative osteoarthritis (DOA), or irreparable RCT and (2) patients who had participated in sports activity in ≤3 years before surgery. Patients who underwent RTSA for fractures, rheumatoid arthritis, and septic arthritis and patients who were undergoing revision RTSA were excluded. A total of 59 patients met the inclusion and exclusion criteria for the study. Among them, 7 patients had a follow-up duration for clinic visits <2 years and were excluded, and 8 patients were excluded during the telephone survey we conducted to assess RTS. Thus, 44 of the 59 patients (74.6%) were ultimately included in the study (Figure 1). For all included patients, we recorded the characteristics (age, sex, diagnosis, site, dominant extremity, body mass index [BMI]) as well as the type of sports they participated in before the surgery.

Flowchart of patient selection. RTSA, reverse total shoulder arthroplasty.
Surgical Techniques and Rehabilitation Protocol
All operations were performed by a single senior orthopaedic surgeon (J.C.Y). All patients in the cohort received a Equinoxe RTSA (Exatech). The RTSA procedures were performed in the beach-chair position using the deltopectoral approach. 24 When cutting the humeral head, 20° of retroversion was applied using the alignment guide supplied with the prosthesis. Posterior and inferior capsules were meticulously released to expose the margin of the glenoid. The subscapularis (SSc) was detached using an SSc peel technique.15,26 The tendinous portion of the SSc was tagged using the Mason-Allen suture method with 3 No. 5 Ethibond strands (Ethicon). The adhesion at the rotator interval and coracoid undersurface was released using a finger or blade with the traction suture tensioned. If possible, the SSc tendon was firmly reattached to the lesser tuberosity with 3 nonabsorbable transosseous sutures (Ethibond; Ethicon). Soft tissue biceps tenodesis was performed when appropriate. A drain was inserted and sutured, and a shoulder abduction brace was applied.
All patients followed a standard postoperative rehabilitation program. 24 They were told to wear an abduction brace for 6 weeks postoperatively. Active elbow motion and handgrip exercises were initiated the day after surgery. Machine-assisted continuous passive motion exercises were allowed the day after the operation. After 6 weeks, braces were removed, and active range of motion (ROM) was allowed. Muscle strengthening exercises were allowed at postoperative week 8. When patients had osteoporosis (T score <–2.5), continuous passive motion exercises were delayed for 2 weeks postoperatively. Resuming sports activity was allowed at 3 months after the surgery for low-demand sports (swimming, fitness, golf, cycling, yoga, jogging, badminton) and 6 months after the surgery for high-demand sports (tennis, table tennis, baseball, basketball).
Clinical and Radiologic Evaluations
Physical examination and functional scores were assessed pre- and postoperatively at every clinic visit. Active ROM, including forward flexion (FF), external rotation with the arm at side, and internal rotation behind the back was assessed. The internal rotation was measured by evaluating the patient's ability to reach the vertebral spinous process with the tip of the thumb (T4-T12, 4-12 points; L1-L5, 13-17 points; buttock, 18 points). 23 Functional scores, including pain visual analog scale (VAS), functional VAS, American Shoulder and Elbow Surgeons (ASES) score, 40 Constant score, 7 and Simple Shoulder Test (SST) 30 were assessed by a trainer with shoulder expertise (S.M.L.).
Plain radiographs were obtained at every follow-up, including shoulder true anteroposterior, axillary lateral, and humeral anteroposterior views. Complications, including acromial fracture, scapular notching, heterotopic ossification, and loosening of the humeral and glenoid component, were recorded. Reoperations during the follow-up period were also recorded. The loosening of the humeral stem was defined as subsidence >5 mm, alignment change >5°, or 2-mm radiolucent lines in ≥3 zones on plain radiographs at final follow-up. 45 Glenoid loosening was defined as a shift of component position or radiographic evidence of central screw failure. 1
Questionnaire of RTS After RTSA
All patients completed a questionnaire regarding RTS after RTSA, adapted from Garcia et al. 11 The questionnaire was conducted by telephone interview in May 2022. Based on their responses, patients were divided into 2 groups according to whether they resumed sports activity, which was defined as participating in sports at least once a week. Group A consisted of patients who resumed sports activities after surgery, and group B included patients who did not participate in sports activities after surgery. For group A, patients were asked about the time between surgery and the start of sports activity as well as frequency and the level of sports activity. For group B, reasons for not participating in sports activities were recorded.
Statistical Analysis
RStudio (Version 2022.02.4+500.pro1; PBC) was used for data analysis. Statistical significance was set at P < .05. A significant difference in the variables of group A and group B was determined using the Student t test or Mann-Whitney U test for continuous variables and the chi-square test or Fisher exact test for the categorical variables.
Results
Demographic Findings
Of the 44 included patients, 28 patients (63.6%) were included in group A (returned to sports) and 16 patients (36.4%) were included in group B (did not RTS). Comparison between groups showed that the mean BMI was significantly lower in group A (24.3 vs 27.1; P = .01). Preoperative diagnosis also significantly differed between groups A and B (CTA/irreparable RCT/DOA diagnoses: 13/12/3 vs 3/6/7; P = .03). Patient characteristics are summarized in Table 1.
Patient Demographics (N = 44) a
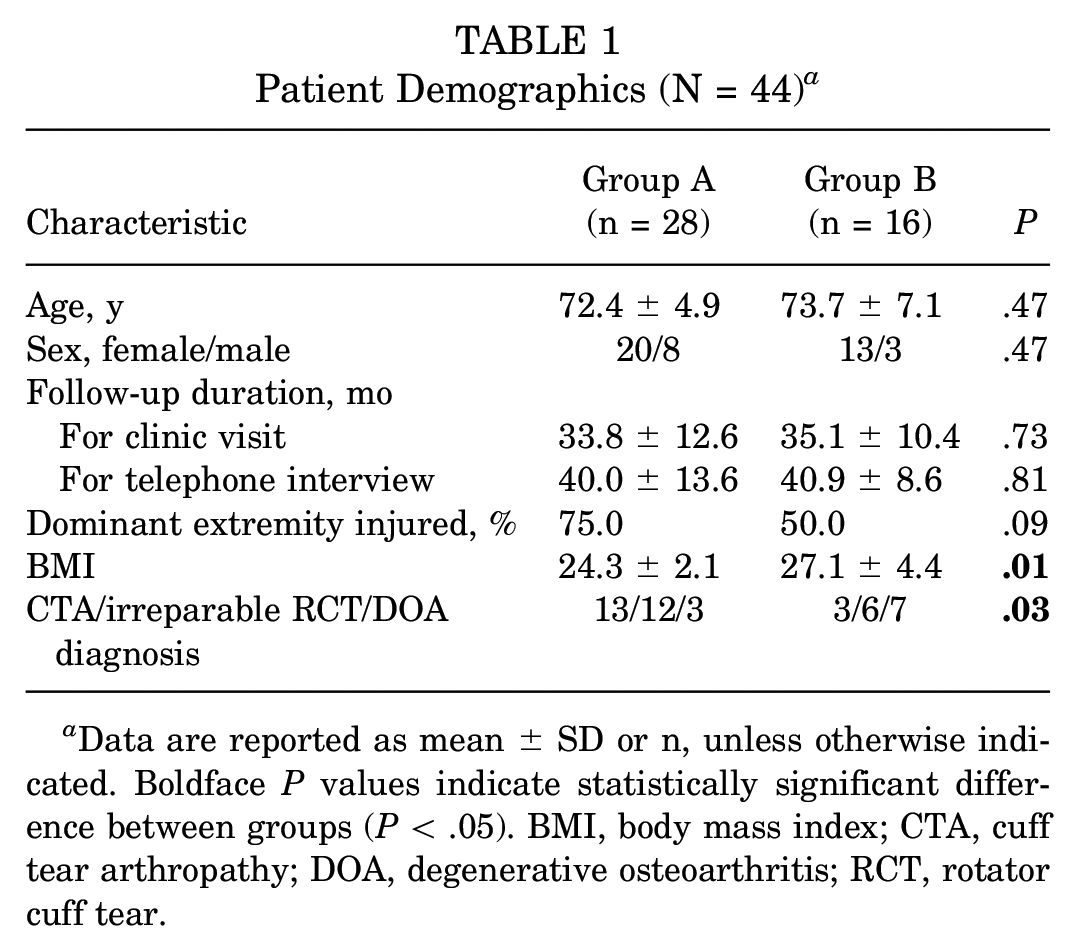
Data are reported as mean ± SD or n, unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). BMI, body mass index; CTA, cuff tear arthropathy; DOA, degenerative osteoarthritis; RCT, rotator cuff tear.
Clinical and Radiological Outcomes
There were no significant differences in ROM and functional scores between the 2 groups preoperatively. However, at the final clinical follow-up after surgery, patients in group A showed significantly higher FF (P = .03) and higher SST score (P = .02) than those in group B (Table 2).
Clinical Outcomes of the Study Groups Pre- and Postoperatively a

Data are reported as mean ± SD. Boldface P values indicate statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; ER, external rotation; FF, forward flexion; fVAS, visual analogue scale for function; IR, internal rotation; pVAS, visual analog scale for pain; SST, Simple Shoulder Test.
T1-T12 = 1-12 points; L1-L5 = 13-17 points; buttock = 18 points.
There were no significant differences in postoperative complications between the 2 groups. One patient (3.6%) in group A and 2 patients (12.5%) in group B had acromial fracture without trauma events, and all of them were treated conservatively. Two patients (7.1%) in group A and 2 patients (12.5%) in group B had subsidence of the humeral component >5 mm, and all of them were treated conservatively. Dislocation occurred in 1 patient from group B at postoperative 2 years, and revision surgery involving liner change was done.
Questionnaire of RTS After RTSA
Table 3 shows the sports activities performed after RTSA. In group A, cycling (100%) had the highest RTS rate after RTSA, followed by fitness (87.5%), golf (85.7%), jogging (75.0%), and yoga (71.4%).
Participation in Sports Activities After RTSA a

Data are reported as n (%). RTSA, reverse total shoulder arthroplasty.
The time between surgery and RTS was 9.1 months (range, 3-36 months), frequency of sports activity was 3.7 times per week (range, 1-7). Out of the 28 patients surveyed, 13 (46.4%) reported an improvement in their level of sports activity compared with their preoperative status. Six patients (21.4%) reported being at the same level, and 9 patients (32.1%) were worse. Regarding the reason for not resuming sports activity, the most common reason was the concern for postoperative complications without any discomfort (n = 6; 37.5%) (Table 4).
Reasons for Not Returning to Sports After RTSA at Final Follow-up a
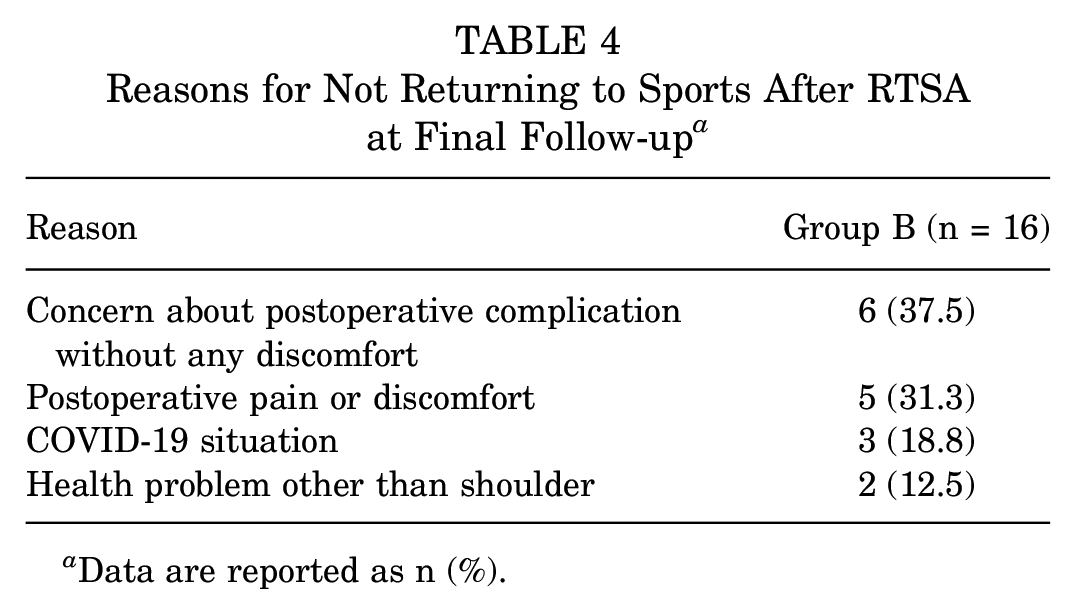
Data are reported as n (%).
Discussion
This study assessed the rate and time of RTS after RTSA in an Asian population and compared baseline and postoperative characteristics between the RTS group and the no RTS group. This study showed that 63.6% of active patients could resume sports activity after RTSA and that the mean time to RTS was 9.1 months. Comparison between the RTS group and the no RTS group showed that BMI and preoperative diagnosis were significant factors associated with RTS after RTSA, and FF and SST scores at final follow-up were significantly higher in the RTS group.
Previous studies reported RTS rates after RTSA between 60% and ~93%, which is consistent with this study.5,8,11,25,31,44,46 However, these data must be interpreted with caution because there were several confounding factors. In reviewing the literature, the definition of the assessment time of preoperative sports participation was different. The definition used, such as “at the time of operation,”“during life,” or “during a presymptomatic phase,” has a considerable impact on the reported RTS rate. 16 Furthermore, in a meta-analysis by Magan et al, 32 the RTS rate was 18.7% 3 months after total knee arthroplasty. However, the RTS rate increased to 75.9% after 9 months and 84.0% after 12 months. In this study, patients who had played sports 3 years before surgery were recruited, and a survey of RTS was conducted ≥24 months after surgery. A precise definition of RTS should be described in future investigations.
Despite promising results of RTS after RTSA, clinicians often hesitate to allow patients to participate in sports activities after RTSA. According to a survey for the American Shoulder and Elbow Surgeons, >75% of surgeons answered that they allow patients to participate in all types of sports for total shoulder arthroplasty (TSA) and hemiarthroplasty (HA). However, only 45.2% of surgeons allow patients to participate in all sports for RTSA and 17.9% for contact sports. 13 This concern mainly comes from the biomechanics of RTSA prosthesis. Simovitch et al 44 argued that the RTSA prosthesis is a semiconstrained joint that encounters unique forces at the prosthetic joint in contrast to the anatomic TSA and HA. Therefore, implant loosening, increased polyethylene wear, late instability, and deltoid fatigue or failure are major concerns for athletic patients.22,44 A comparative study by Geyer et al 12 reported that when compared with nonathletic patients, the athletic group showed significantly better clinical outcomes after RTSA without a greater risk of implant loosening and scapular notching. However, in the athletic group, incomplete radiolucency around the humeral component was observed more frequently. A large multicenter study by Levigne et al 27 showed that the incidence of scapular notching after RTSA was higher in more active patients. In a comparison study of RTSA and HA by Liu et al, 31 patients who underwent RTSA had significantly higher RTS rate, higher satisfaction with their ability to play sports, and fewer postoperative complaints than patients who underwent HA. In our study, clinical outcomes, including FF and SST scores, were significantly higher in the RTS group compared with the no RTS group and there was no difference in radiologic outcome and complications. Considering all this evidence, patients in the RTS group seem to have had better clinical outcomes compared with those who did not RTS, but the safety of sports activity after RTSA seems unclear. Further studies with long-term follow-up will be needed to assess the safety of returning to sports after RTSA.
The results of this study showed that BMI and preoperative diagnosis were significant predictive factors for RTS. Li et al 28 found that obese and overweight patients had a lower physical function after anatomic TSA. Garcia et al 11 reported that age <70 years was a significant predictor of a higher rate of RTS. In contrast to the current study, high BMI was not a significant predictor. There are conflicting results on the clinical outcome of RTSA depending on the preoperative diagnosis.29,41,47 A large cohort study by Saini et al 41 showed that patients with a preoperative diagnosis of glenohumeral osteoarthritis (GHOA) demonstrated significantly better postoperative active FF, ER, ASES, Single Assessment Numeric Evaluation, and VAS scores. They suggested that an intact rotator cuff in patients with GHOA provides balanced force coupling, explaining better functional outcomes. However, Werner et al 48 reported that patients with an intact rotator cuff correlated with poor postoperative improvements after RTSA. Boileau et al 2 further demonstrated that RTSA in patients with >90° of active forward elevation preoperatively was a risk factor for lower patient satisfaction scores. Both studies suggested that higher preoperative function limits the potential to achieve postoperative satisfaction after RTSA. Therefore, we hypothesize that patients with GHOA showed a lower RTS rate due to lower satisfaction after RTSA. Further studies with larger sample sizes will be needed to clarify the correlation.
Successful RTS after RTSA mostly depends on goals, motivation, type of sports, and pain tolerance. Among them, the types of sports patients play are most likely different across different cultures and ethnicities. Golf was the most popular sport for US patients, and while hiking was most popular for Swiss patients.5,11,25,31 In the current study, all the patients were Asian, and the results showed that swimming was the most popular sport. Moreover, although an RTS rate was low, patients in the US and European countries played high-load sports before the surgery such as tennis and skiing. However, only 1 patient (2.3%) played tennis before the surgery. According to a national survey done by the South Korean government, only 6.4% of elderly people have participated in high-demand sports activities. In this survey, reasons for low participation in moderate- to high-demand sports mostly came from a cultural belief that the elderly could not play such high-demand sports. 35 This is consistent with the result of this study that half of the patients did not resume sports activity solely due to a concern about complications or discomfort that has not happened yet. Moreover, a substantial proportion of the elderly population in rural areas works in agriculture. Further studies will be needed to assess the return to work after RTSA.
Limitations
There are several limitations to this study. First, as previously discussed, most patients in this study population group did not participate in sports activities in old age. Because of that reason, the sample size of this study was small. Further studies might be needed with a larger sample size. Second, the final follow-up was done with a telephone survey. Even though this study only included patients who underwent surgery ≥5 years of the survey date, there is a chance of recall bias because most of the patients were of old age. Third, because of the COVID-19 pandemic, most of the sports centers shut down from 2020 to 2022. This acted as a barrier to RTS activities. especially indoor sports such as swimming. Fourth, this study defined the time of RTS as the day initiating sports activity after surgery. Assessing the time of RTS in full recovery could also give more information to clinicians and patients. Fifth, since a single implant with a modern lateralized type was used in this study, we could not analyze the effect of implant type on the RTS rate. Finally, due to the retrospective study design, it was impossible to tell whether better functional outcomes in the RTS group were the result after patients returned to sports or the reason why they were able to RTS.
Conclusion
The RTS rate after RTSA was 63.6%, and the time to RTS was 9.1 months. Patients with a low BMI and those diagnosed with CTA or irreparable RCT were found to have better RTS rates after undergoing RTSA. FF and SST scores at final follow-up were significantly higher in the RTS group, with no significant differences in complications.
Footnotes
Final revision submitted May 23, 2023; accepted June 7, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Samsung Medical Center institutional review board (No. SMC 2022-08-016-001).