
Abstract
Background:
Malpositioning of the femoral button is a known technical complication after anterior cruciate ligament (ACL) reconstruction with cortical suspensory fixation. The incidence of malpositioning, as well as the efficacy of methods to prevent malpositioning of cortical suspensory fixation devices, has not been reported.
Purpose:
To determine the rate of malpositioned cortical suspensory fixation devices after ACL reconstruction, investigate which intraoperative technique yields the lowest rate of malpositioning, and determine the return-to-duty rate for active-duty service members with malpositioned buttons and the revision rate for malpositioned buttons.
Study Design:
Case series; Level of evidence, 4.
Methods:
The records of patients who underwent primary ACL reconstruction with a cortical suspensory fixation device between 2008 and 2018 were reviewed at our institution. Postoperative radiographs were reviewed for evidence of malpositioned femoral buttons. Malpositioned buttons were classified as (1) fully positioned in the bone tunnel, (2) partially positioned in the bone tunnel, (3) >2 mm from cortical bone, or (4) deployed over the iliotibial band. Operative reports were reviewed to determine the intraoperative methods undertaken to verify the button position. The rate of malpositioned cases with subjective instability and revision surgery performed were determined. The ability of patients to return to full military duty was reviewed for active-duty personnel.
Results:
A total of 1214 patients met the inclusion criteria. A 3.5% rate (42 cases) of malpositioned cortical suspensory fixation devices (femoral buttons) was identified. For patients with malpositioned buttons, 7 (16.7%) patients underwent revision surgery in the immediate postoperative period. Techniques used to avoid malpositioning included direct arthroscopic visualization, direct open visualization, intraoperative fluoroscopy, and first passing the button through the skin before positioning on the femoral cortex. There was a 4.6% malposition rate using direct arthroscopic visualization and a 5.1% malposition rate using passage of the button through the skin, while no malpositioning occurred with intraoperative fluoroscopy or direct open visualization (P < .05). Overall, 12 (28.6%) patients with malpositioned buttons ultimately underwent revision surgery. Despite having been diagnosed with malpositioned buttons, 21 (63.6%) active-duty members were able to return to full duty.
Conclusion:
Malpositioning of femoral buttons during ACL reconstruction occurred in 3.5% of patients in this series. The techniques of intraoperative fluoroscopy and direct open visualization are encouraged to prevent malpositioning.
There has been significant variability in anterior cruciate ligament (ACL) surgical techniques including graft type, positioning of tunnels, single- or double-bundle reconstruction, and type of graft fixation. 4 Femoral-sided graft fixation during ACL reconstruction can be performed with a myriad of techniques, 1 of which includes cortical suspensory fixation with a suture button. 8 The use of cortical suspensory fixation has the advantage of smaller incisions and maximizing the graft to fill the tunnel. 5 Disadvantages of cortical buttons include malpositioning due to soft tissue interpositioning, button migration, interosseous button deployment, and lateral thigh pain.3,6,7,11 Soft tissue interpositioning with femoral fixation can occur in 2.8% to 25.8% of cases. Femoral-sided fixation has also been reported to be intraosseous in 3.6% of cases.6,12
There are various techniques to verify the appropriate placement of a cortical button used for graft fixation. Direct arthroscopic visualization, marking the femoral tunnel length on the graft, intraoperative fluoroscopy, and direct visualization of the button through a direct lateral incision have all been described.2,8-10,12 Direct arthroscopic visualization is achieved by insertion of the arthroscope through the anteromedial portal, facilitating an unobstructed view of the femoral tunnel as the button is pulled through and out the smaller cortical hole, and by visualization of the button as it exits the tunnel to then be flipped horizontally. Balldin et al 1 described the use of intraoperative fluoroscopy to verify that the button is seated against the lateral femoral cortex. Regardless of the technique used, accurate placement of the cortical button is important to prevent graft loosening and surgical failure secondary to construct laxity.
The primary purpose of this study was to determine the rate of malpositioned cortical suspensory fixation devices after ACL reconstruction. The secondary purpose of this study was to investigate which intraoperative technique yielded the lowest rate of malpositioning. The tertiary purpose was to determine the return-to-duty rate for active-duty service members with malpositioned buttons and the revision rate for malpositioned buttons. We hypothesized that direct visualization or intraoperative fluoroscopy would result in the lowest rate of malpositioning.
Methods
A retrospective review was performed on a consecutive series of adult patients, aged 18 to 63 years, who underwent primary ACL reconstruction at a single institution between 2008 and 2018. The study protocol was approved by our institutional review board, and investigators adhered to policies for the protection of human participants as prescribed in Title 45, Part 46 of the Code of Federal Regulations. Informed consent was waived due to this project being retrospective and approved by the IRB. Postoperative radiographs were used to verify that a cortical suspensory fixation device was used for femoral fixation. Revision reconstruction procedures were excluded, as were all cases without radiographs or those that used a different technique for femoral fixation. Radiographs were obtained in the postoperative recovery room. All radiographs were evaluated for the femoral button position with ≥2 radiographic projections. Cases with <2 radiographic projections or inadequate radiographs were excluded.
The radiographs were reviewed by 1 of the authors (J.A.) to identify malpositioned cases. Then, 3 orthopaedic surgeons who were fellowship trained in sports medicine (L.Z., C.R.B., and S.M.G.) reviewed the radiographs of malpositioned cases independently and classified them as 1 of 4 types: (1) fully positioned in the bone tunnel (Figure 1A), (2) partially positioned in the bone tunnel (Figure 1B), (3) >2 mm from cortical bone (Figure 1C), or (4) flipped outside of the iliotibial band (ITB) (Figure 1D). The distance from the closest point of the cortical suspensory fixation device to the femoral cortex was measured. A measurement of ≥10 mm was classified as type 4 (outside of the ITB). Type 4 is a new classification category introduced by Toftoy et al. 12

Malpositioned buttons by classification. (A) Type 1 malpositioning with the cortical button fully positioned in the bone tunnel. (B) Type 2 malpositioning with the cortical button partially positioned in the bone tunnel. (C) Type 3 malpositioning with the cortical button >2 mm from the lateral femoral cortex. (D) Type 4 malpositioning with the cortical button ≥10 mm from the lateral femoral cortex, typically over the iliotibial band.
Operative reports were reviewed to determine what methods were undertaken to verify the button position intraoperatively. Cases from 8 surgeons were obtained and reviewed; 4 of the surgeons were sports fellowship trained. A guide pin was placed using a femoral tunnel guide. A femoral tunnel was created using a retrograde drill device. The graft was passed through the femoral tunnel attached to a TightRope device (Arthrex), used in all cases for femoral-sided fixation. Several techniques were used to verify the button position: (1) direct arthroscopic visualization, (2) direct open visualization, (3) intraoperative fluoroscopy, and (4) pulling the button through the skin and back down to the lateral femoral cortex without direct open visualization (Figure 2).
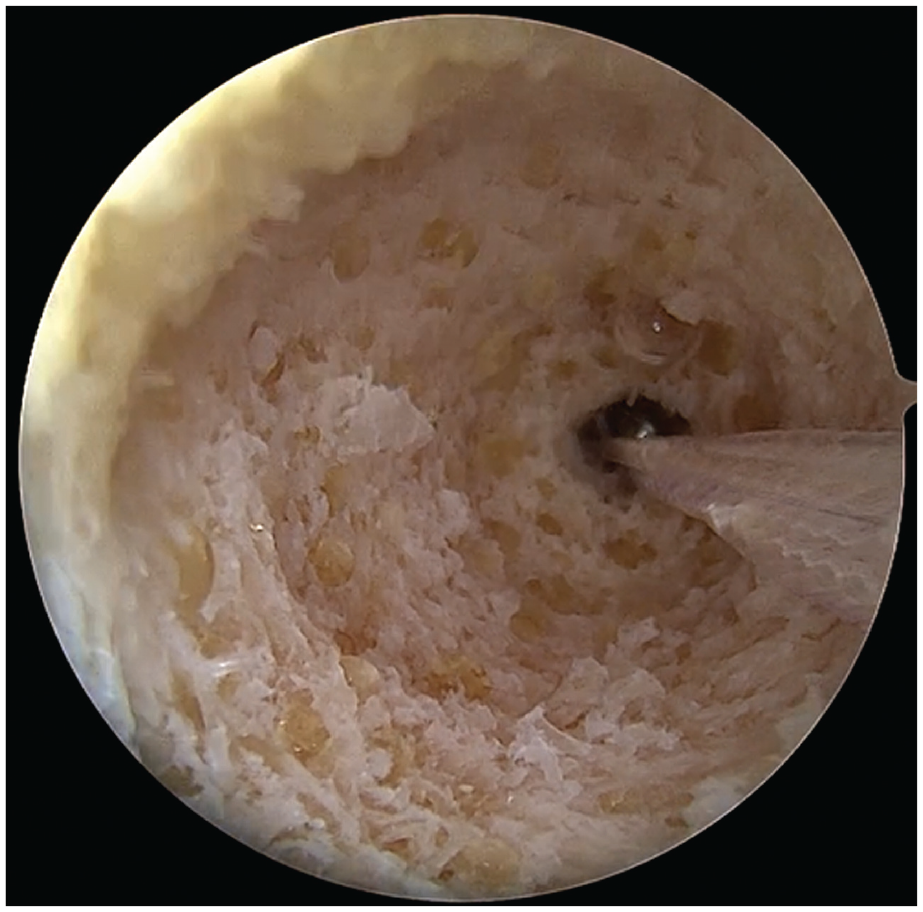
Direct arthroscopic visualization as shown from the anteromedial portal using a standard 30° arthroscope to visualize the deployment of the button on the lateral femoral cortex.
A retrospective chart review was performed for all patients with a malpositioned button to report the rate of revision surgery, rate of subjective instability and the return-to-duty rate for active-duty personnel. Cases were evaluated with a target of 3 months from the index procedure. The time from the index procedure to the first revision procedure was determined. The time between additional revision procedures was not recorded.
Statistical Analysis
Standard descriptive statistics were calculated to summarize background characteristics and malposition rates for the patients. The chi-square test and Fisher exact test were used to assess unadjusted associations between categorical variables, and the nonparametric Kruskal-Wallis test and Wilcoxon rank-sum test were used to evaluate differences in the median surgery duration among techniques. The Pearson chi-square test was used to compare malposition rates among techniques. A 95% confidence interval for the malposition rate was based on the exact binomial distribution. Interobserver reliability of the malposition type was calculated using the Fleiss kappa. All analyses were conducted using SAS statistical software (Version 9.4; SAS Institute) with an alpha cut off of 0.05 for significance.
Results
There were 2056 ACL reconstruction procedures performed between 2008 and 2018, of which 466 did not use femoral-sided suspensory fixation and were therefore excluded. Additionally, 190 cases had inadequate or no postoperative imaging to evaluate for malpositioning. A review of records determined that 109 were revision cases, 8 were duplicate records, and 69 had incomplete medical records, and all were therefore excluded. Thus, we had 1214 ACL reconstruction procedures that were performed with femoral-sided suspensory fixation (Figure 3).
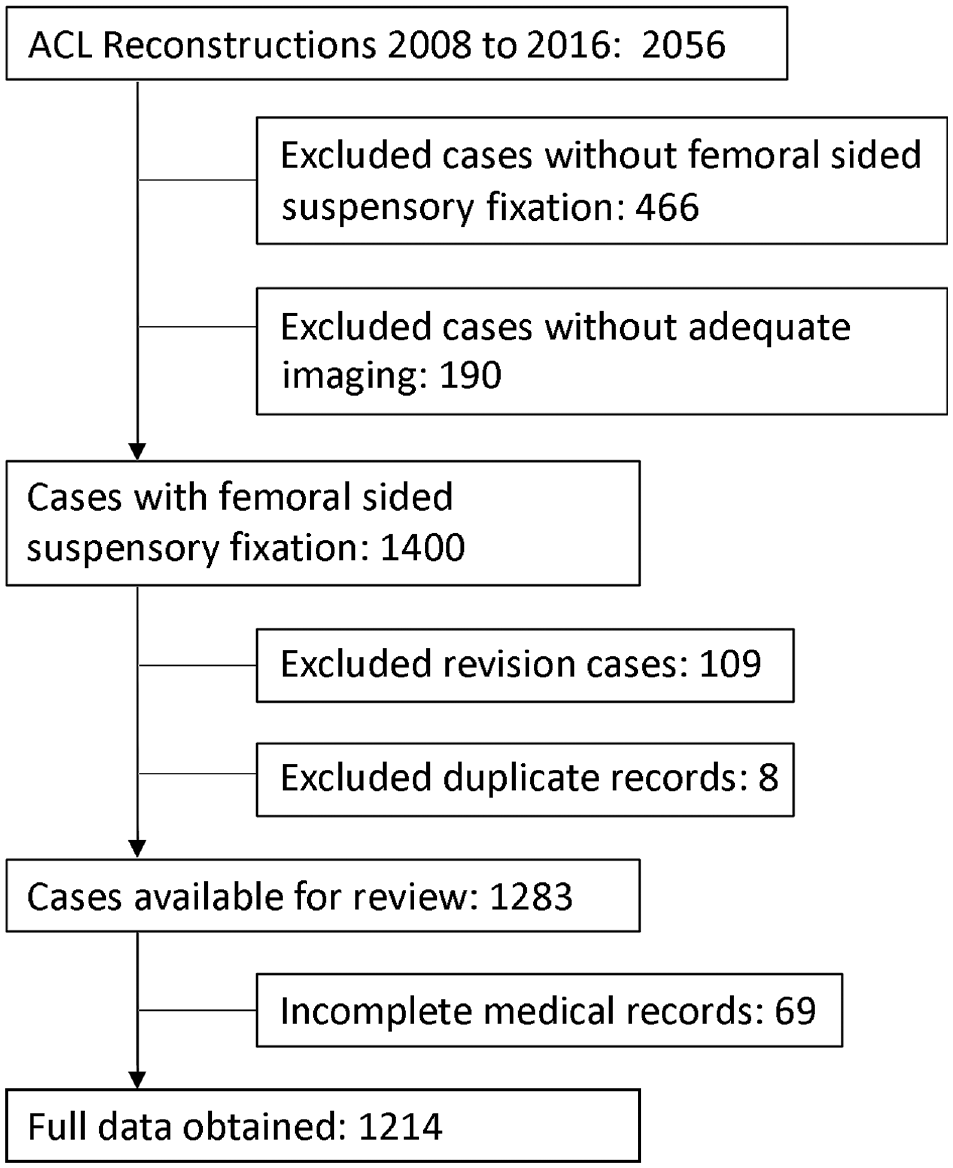
The number of anterior cruciate ligament (ACL) reconstruction cases obtained from 2008 to 2018 and the breakdown of cases excluded and included in the current study.
The mean age of the 1214 study patients was 29.4 ± 7.3 years; there were 1007 male (82.9%) and 207 female (17.1%) patients. The mean surgical time was 102.0 ± 60.4 minutes. We identified 42 (3.5%) cases of malpositioned buttons. Of these, we noted 38 cases with a 4.6% malposition rate for direct arthroscopic visualization and 4 cases with a 5.1% malposition rate for the technique of button passage through the skin. There were no malpositioned cases using direct open visualization or intraoperative fluoroscopy. There was a statistically significant difference in the malposition rate among techniques (P = .002) (Table 1).
Malposition Rate by Intraoperative Technique

There were no significant differences in the malposition rate by patient age, patient sex, duration of surgery, or year of surgery (Table 2). There was also no significant difference in the malposition rate over time when the same surgical technique was used and no difference in the rate of malpositioning between the 8 surgeons involved (P = .46).
Malposition Rate by Patient and Surgeon Characteristics

Upon a review of postoperative imaging, there were 8 type 1, 11 type 2, and 19 type 3 malpositioned cases. The type 3 cases identified had a mean distance between the button and bone of 4.8 ± 1.7 mm. There were 4 patients with type 4 malpositioning, with a mean distance of 13.8 ± 1.1 mm (Table 3).
Distance From Bone and Revision by Malposition Type

The interobserver reliability using the malposition classification system was good, with a kappa value of 0.861. Of the 42 patients, 3 were lost to follow-up. Of these 3, there was 1 each identified with type 1, type 2, and type 3. The remaining patients had a mean follow-up of 6.6 ± 5.7 months. The median follow-up was 4.8 months (range, 0.9-30.3 months).
In cases of button malpositioning identified postoperatively, the indication for revision surgery was based on surgeon preference. In the immediate postoperative period (≤30 days), 1 type 1, 2 type 3, and 4 type 4 cases underwent revision. All type 4 malposition cases that underwent immediate revision were reported to have been verified intraoperatively with direct arthroscopic visualization without fluoroscopy.
Delayed revision occurred for 1 type 1 case after 15 months from initial surgery because of a repeat injury. The remaining type 1 cases reported a subjectively stable knee at follow-up. Revision surgery was performed for 2 type 2 cases. A case underwent revision because of a retear, and the other case had continued instability. An additional type 2 case reported having an unstable knee but did not undergo revision surgery. Delayed revision was performed for 2 type 3 cases: one at 14 months and the other at 2 years postoperatively because of a retear and instability. The remaining type 3 cases reported a stable knee.
The ability to return to full active duty was recorded for military members. Active-duty members were able to return to duty at a rate of 63.6% (21/33) with malpositioned buttons from the index procedure. All type 1 malpositioned cases were able to return to full duty and final follow-up. Further, 78% of type 2, 80% of type 3, and 100% of type 4 cases returned to full duty. There were 2 type 3 cases that did not undergo revision surgery and were unable to return to full duty. Additionally, 7 cases underwent revision surgery and were able to return to full duty. There were 3 cases, 2 type 2 and 1 type 3, that underwent revision surgery but were unable to return to duty.
Discussion
In our study of 1214 cases, our goal was to better define and classify malpositioning of the cortical button and quantify the rate of malpositioning by technique with a large sample size in a young, active patient population. There was good interobserver reliability of the malposition classification (κ = 0.861). We found a 4.6% rate of malpositioning when direct arthroscopic visualization was performed and a 5.1% malposition rate with first passing the button through the skin. There were no cases of malpositioning when fluoroscopic confirmation was performed intraoperatively or when an open lateral approach was used to directly visualize button placement on the lateral femoral cortex.
A previous study performed by Balldin et al 1 found a 10% rate of button malpositioning in 100 consecutive cases. There were no cases of malpositioning when fluoroscopy was used for 60 cases. 1 In comparison to the current study, their sample size was smaller, did not evaluate for malpositioning partially or fully in the tunnel, and did not evaluate direct open visualization or pulling the button through the skin.
Complications other than graft laxity have been reported with button malpositioning. Taketomi et al 11 described 2 cases that developed ITB irritation from the placement of an EndoButton (Smith & Nephew) close to the lateral epicondyle. Kawaguchi et al 3 reported 3 similar cases of lateral knee pain from using a TightRope device close to the lateral epicondyle with ITB irritation. Mae et al 6 reviewed 101 cases of double-bundle ACL reconstruction with EndoButton femoral fixation. There were 51 cases with tissue interpositioning (50.5%) and 71 cases of migration (70.3%). There were no reported clinical differences between cases with or without tissue interpositioning or EndoButton migration using KT-1000 arthrometer side-to-side differences or patient-reported Lysholm scores. 6 Nag and Gupta 7 reported a case of a TightRope device becoming stuck at the lateral edge of the femoral tunnel. This may result in a false impression that the cortical button has flipped. The button can then be pulled within the femoral tunnel, resulting in graft loosening. When pulling the button out of the skin and placing it from outside in, the vastus lateralis can become trapped between the button and cortical bone. 7
Intraoperative fluoroscopy is a fast and effective way to confirm proper positioning of the cortical button on the lateral femoral cortex by finding the radiographic projection orthogonal to the femoral tunnel. Fluoroscopy is also more accurate compared to postoperative plain films, which may not capture an orthogonal view and may misrepresent the actual button position. An open lateral dissection can also be performed and is understandably very successful in ensuring the button position; however, the operating surgeon may desire a faster and less invasive alternative to verify the button position.
Limitations
The limitations of our study include its retrospective nature, lack of patient-reported outcomes, lack of patient-reported scoring metrics, and loss to follow-up. There were no patient-reported outcomes at follow-up, and a short-term follow-up was another limitation. Another limitation of this study is the absence of consistently scored Lachman grades and KT-1000 arthrometer testing. There were 3 cases of malpositioning that were lost to follow-up within the military medical system. Future prospective studies can further evaluate the incidence of ITB irritation, patient-reported outcomes, and the incidence of knee instability due to malpositioned buttons.
Conclusion
In the current study, there was a 4.6% rate of cortical button malpositioning when direct arthroscopic visualization was performed and a 5.1% malposition rate when first passing the button through the skin. No cases of malpositioning occurred with intraoperative fluoroscopy or the open lateral approach for visualization. Also, 28.6% of patients with malpositioned buttons underwent revision surgery. To avoid malpositioning of a cortical suspensory fixation device, intraoperative fluoroscopy or direct open visualization should be utilized.
Footnotes
Final revision submitted May 10, 2023; accepted May 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.A. has received education payments from ImpactOrtho. L.Z. has received grant support from Arthrex and hospitality payments from Stryker. C.R.B. has received education payments from Arthrex, nonconsulting fees from Arthrex, and honoraria from MTF Biologics. S.M.G. has received education payments from Supreme Orthopedic Systems and Sea Pearl and grant support from Arthrex. The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the Department of the Army, the Department of Defense, or the United States government. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Tripler Army Medical Center (TAMC 19R10).