
Abstract
Background:
Suspensory fixation of anterior cruciate ligament (ACL) reconstruction (ACLR) grafts has emerged as a popular device for femoral graft fixation. However, improper deployment of the suspensory fixation can compromise proper graft tensioning, leading to failure and revision. Also, soft tissue interposition between the button and bone has been associated with graft migration and pain, occasionally requiring revision surgery. Many surgeons rely on manual testing and application of distal tension to the graft to confirm proper button deployment on the lateral cortex of the femur for ACL graft fixation.
Purpose:
To determine the reliability of the manual resistance maneuver when applying distal tension to deploy the suspensory device along the lateral cortex of the femur.
Study Design:
Case series; Level of evidence, 4.
Methods:
All patients undergoing ACLR with a suture button suspensory device for femoral fixation were eligible for enrollment in the study. The surgeries were performed by 3 board-certified, sports medicine fellowship–trained orthopaedic surgeons at a single outpatient surgical center between May 2018 and June 2019. All grafts were passed in a retrograde manner into the femoral tunnel, and a vigorous manual tensioning maneuver in a distal direction was placed on the graft to deploy and secure along the lateral cortex of the femur. Intraoperative mini c-arm fluoroscopy was obtained to demonstrate proper suture button positioning. If interposing tissue or an improperly flipped button was identified, rectifying steps were undertaken and recorded.
Results:
A total of 51 patients with a mean age of 33.3 years were included in the study. Of these patients, 74.5% had normal suture button positioning identified via intraoperative fluoroscopic imaging, while 15.7% had interposed soft tissue and 9.8% had an improperly flipped button. In all cases, the surgeon was able to rectify the malpositioning intraoperatively.
Conclusion:
Despite the manual sensation of proper suspensory button positioning, intraoperative fluoroscopy identified suture button deployment errors in ACLR 25% of the time. Correcting the malpositioning is not technically demanding. These findings advocate for routine intraoperative surveillance to confirm appropriate suture button seating during ACLR.
Suspensory fixation of anterior cruciate ligament (ACL) graft to the femur is a popular technique employed in ACL reconstruction (ACLR). 5,13 –16,36 This technique allows for technical ease and speed 12,18 –20,32 while providing a secure fixation with excellent tensile strength. 1,3,8,9,23,25,32 Clinical data have also demonstrated positive patient-reported outcomes and knee stability with suspensory ACL fixation. 4,27 Alternative graft fixation techniques include the use of interference screw fixation, which has been associated with many drawbacks, including screw divergence, graft laceration, graft advancement within the bone tunnel, and bone plug fractures. 5,11,18
Several studies have reported the complications of suspensory fixation. One of the most common reported complications is improper deployment of the fixation, leading to soft tissue interposition between the button and lateral femoral cortex. Two studies have reported that tissue interposition occurs in 15% and 25.2% of patients as identified by postoperative computed tomography scans and radiographs, respectively. 17,34 Tissue interposition has been reportedly associated with tissue irritation and migration of the button. 10,12,17,20,28,32 Tissue irritation can cause postoperative knee pain 10,12 and has been associated with iliotibial band (ITB) friction with ITB thickening. 12,33,34 Mae et al 17 postulated that the associated button migration causes weakening of the femoral fixation before graft incorporation and thereby leads to neoligament loosening and failure of the reconstruction. Other reported complications associated with improper suture button flipping through the bone tunnel and properly engaging against the bone cortex include loss of graft tension, intra-articular migration, malpositioning within the femoral tunnel, and tunnel enlargement. §
Despite the identified risks associated with suture button malposition, there is currently no gold standard to verify proper suture button positioning during ACLR with suspensory fixation. Some surgeons rely on manual testing of a either a “hard stop” upon application of tension to the graft or sensing the flipping sensation on the graft to ensure proper graft positioning without any confirmatory fluoroscopic imaging. 6,11 Alternatively, some studies have advocated for direct visualization via arthroscopy or a different portal site, but these are associated with prolonged operative time and additional port sites. 10,18,20,24,31,32
The purpose of this study was to determine the reliability of the manual tension method of testing suspensory button fixation on the lateral femoral cortex. In addition, intraoperative fluoroscopic imaging will be used to detect and rectify positioning problems before final graft fixation. The authors hypothesize that the manual tension test is unreliable, and many buttons that feel well-positioned will either demonstrate interposed soft tissue or not be appropriately flipped. Intraoperative fluoroscopy will help identify these problems and allow for immediate rectification.
Methods
This was a prospective study approved by the institutional review board. All patients with ACL deficiency who were indicated for primary or revision reconstruction in which suspensory fixation was the preferred method of femoral fixation but did not have multiligament injuries were eligible for the study. All patients were identified and gave consent preoperatively. Prospective data were then collected from all ACLRs performed using an adjustable loop suture button suspensory fixation (Arthrex Tightrope RT or Mitek Rigid Loop) by 3 board-certified orthopaedic surgeons (R.A.A., K.C., C.E.) at a single outpatient surgical center between May 2018 and June 2019. Collected data included patient age and sex, surgeon’s name, graft type, button type, primary or revision procedure, and concomitant procedures.
In each case, the prepared ACL graft was secured to the femoral suspensory button in the manner described by each respective company at the femoral end of the graft and then passed through the tibial tunnel into the knee joint using a passing suture. The arthroscope was then placed into the anteromedial portal. The graft and suspensory button construct was pulled into the intercondylar notch, and the button was felt to toggle as it exited first the femoral socket and then lateral femur. Next, the button was flipped in standard fashion. After the button was felt to be flipped by the surgeon, tension was applied to the suture on the tibial aspect of the graft. When the graft was manually tensioned to a firm endpoint at 90° of knee flexion, the surgeon considered the button adequately flipped and appropriately positioned. The surgeon then obtained fluoroscopic images with a small c-arm intraoperatively. These included both anteroposterior (AP) and oblique AP views to verify the position of the button relative to the lateral cortex. Imaging was interpreted to demonstrate whether the button was properly engaged against the cortex (Figure 1A), interposing soft tissue was present between the button and the cortex (Figure 1B), or the button was improperly flipped (Figure 1C).

(A) Appropriately flipped button seated on the lateral femoral condyle. (B) Interposing soft tissue between flipped button and lateral femoral condyle. (C) Button partially flipped within femoral bone tunnel.
If an error was detected on the radiograph, information on any rectifying steps and follow-up imaging were recorded. The interposing soft tissue was speculated to be vastus lateralis or ITB depending on the distance from the condyle. In cases of interposed soft tissue, the button was unflipped and the sutures pulled and spun in an alternating fashion from the femoral and tibial ends of the graft while cycling the knee in an attempt to bypass the interposed tissue. Then, a second attempt was made to flip the button against the cortex, and a fluoroscopic image was taken. If the button was still incorrectly positioned, a small skin incision was made over the lateral distal femur and ITB, and the soft tissues were bluntly dissected around the button to remove interposed soft tissue. Tension was applied to the graft from the tibial side to seat the button on the lateral cortex. The characterization of interposed tissue was confirmed if directly visualized during this additional exposure. When the button was found to be partially flipped in the bone tunnel, the button was unflipped and redeployed.
Results
A total of 64 consecutive patients met the inclusion criteria for the study. Twelve were excluded from the study because they received medication by anesthesia before study personnel met the patient. One patient declined participation. A total of 51 patients (53% female) with a mean age of 33.3 years (±11.5) were enrolled in the study. Table 1 summarizes the surgical details collected for the study cohort.
Surgical Details of Study Cohort a
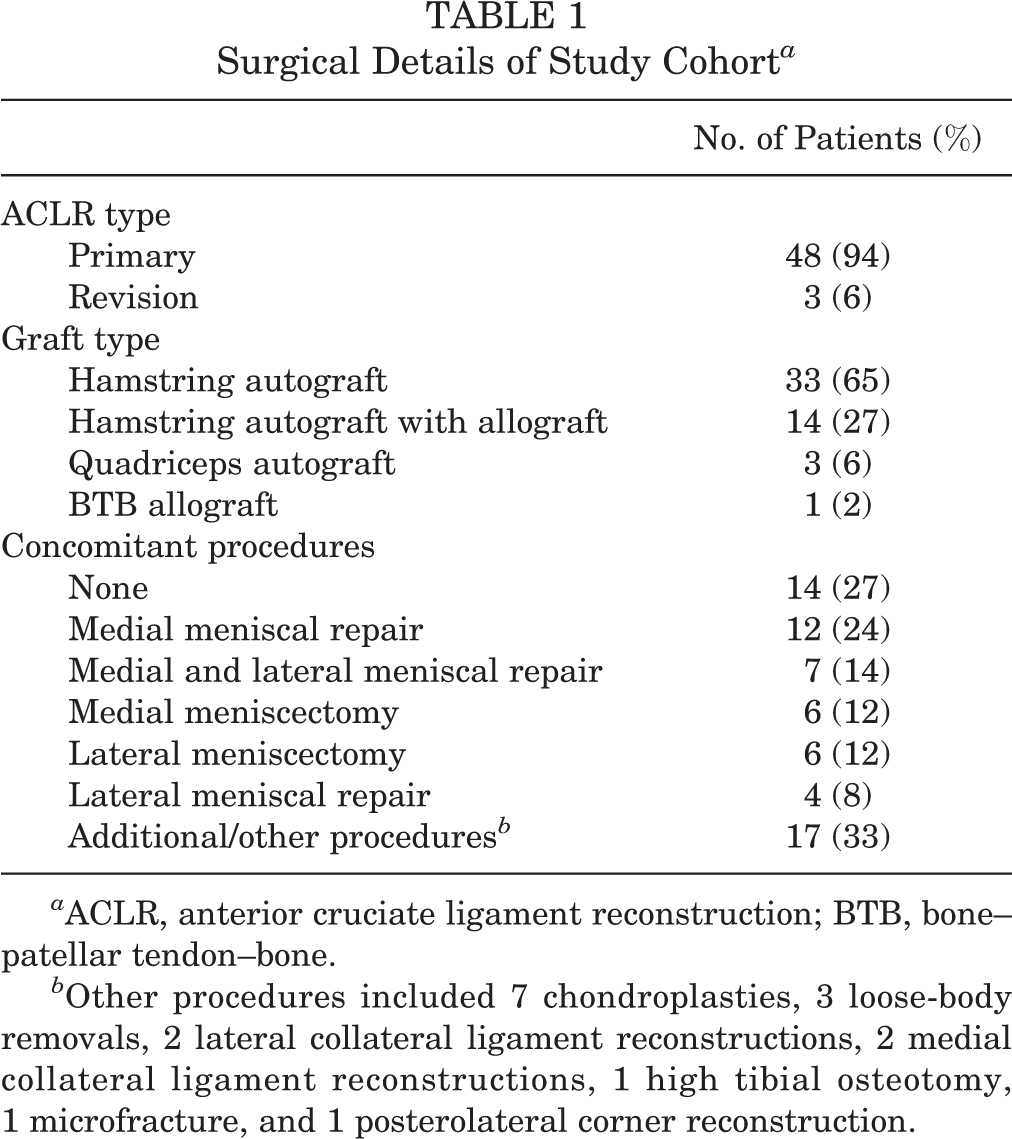
a ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone.
b Other procedures included 7 chondroplasties, 3 loose-body removals, 2 lateral collateral ligament reconstructions, 2 medial collateral ligament reconstructions, 1 high tibial osteotomy, 1 microfracture, and 1 posterolateral corner reconstruction.
Intraoperative fluoroscopy indicated a properly engaged suture button on the lateral cortex in 38 knees, representing proper positioning in 74.5% of cases. All knees with an improperly engaged suture button were a primary ACLR. Of the remaining quarter of patients, fluoroscopic imaging revealed interposed soft tissue in 8 patients (15.7%). In 5 of these patients, the button was flipped within the muscle of the vastus lateralis. In the other 3 patients, the button was flipped superficial to the ITB. In 3 patients, pulling on the suture or cycling the knee rectified the problem. For the 5 patients with persistent interposed soft tissue, an incision was made to dissect down to the button and clear the tissue. The interposed soft tissue was identified at this time as ITB in 2 cases and vastus lateralis in 3 cases.
In an additional 5 patients (9.8%), the button was incompletely flipped. Four buttons were partially flipped within the femoral bone tunnel. These were unflipped, pulled through the tunnel, reflipped, and found to be in appropriate position. In 1 case, the button was flipped on the lateral cortex but on the posterior-most aspect of the condyle. There was concern for impending cortical breakthrough as the posterolateral position of the femoral tunnel aperture resulted in a thin posterior wall. Thus, the button was pulled through a lateral incision and removed from the suture. The suture was then wrapped around a screw and washer, which were placed into the lateral condyle anterior and proximal to the bone tunnel. In all cases of identification of improper suture button positioning, the surgeon was able to rectify the malpositioning intraoperatively. Tables 2 and 3 summarize the characteristics and fluoroscopic findings of improperly engaged sutures.
Characteristics of Improperly Engaged Suture a

a ACLR, anterior cruciate ligament reconstruction; BTB, bone–patellar tendon–bone.
Fluoroscopy Findings of Improperly Engaged Suture Button a

a ITB, iliotibial band; NA, not applicable.
Discussion
This current study reports a high incidence of improper suture button deployment in ACLR despite intraoperative manual testing for a hard stop while applying tension to the graft. Specifically, 15.7% had interposed soft tissue between the suture button and bone cortex, a percentage comparable with previously reported postoperative rates of tissue interposition of 15% 34 and 25.2%. 17 Further, an additional 9.8% of patients had improperly flipped suture buttons. Together, this suggests that without additional evaluation, 25% of patients would have an undiagnosed improper suture button positioning.
Identification of improperly placed suture buttons is important because previous studies have shown that tissue interposition and improperly flipped suture buttons are associated with complications, including postoperative pain and suture button migration. 10,12,17,20,28,32 –34 In this study, identifying these errors intraoperatively allowed the surgeon to take steps to rectify the problem prior to final graft fixation in all of the cases. Surgeons were able to achieve the correct suture button position without interposing tissue by manipulating the device, rotating the knee, or extending the incision over the ITB.
Despite the high rate of suture button improper positioning and the associated complications, there is no agreed upon technique to rule out deployment errors. Many surgeons rely on only manual graft testing, while previous studies have advocated for alternative intraoperative techniques to minimize the complication occurrence. Sonnery-Cottet et al 32 recommended arthroscopically visualizing the button deployment using a scope, followed by postoperative confirmatory radiographs. Mistovich et al 18 and Nag and Gupta 20 both recommended creating an additional portal to directly visualize the correct button seating. Direct visualization is more invasive and increases soft tissue or cartilaginous damage to verify suture button placement for all patients. 18,20 In contrast, only 6 patients (11.7%) in this study required an additional lateral incision to rectify an improperly deployed suture button initially identified via fluoroscopy. Further, direct visualization does not prevent radiation exposure as postoperative imaging to confirm button positioning may still be required. 32 Instead, this study supports the use of intraoperative fluoroscopy to verify the position of the suture button after button flipping. Previous studies have also championed the use of intraoperative fluoroscopy in this role, 2,17,24,28,33,34 but this study adds to the literature by demonstrating that intraoperative fluoroscopic imaging is an effective method to both identify and rectify the malpositioning.
Despite the identified advantages, the benefit of intraoperative fluoroscopy must be balanced against the associated risks. Intraoperative fluoroscopy is associated with radiation exposure, increased procedure length, and the need for the mini c-arm during the procedure. Intraoperative radiation exposure is dependent on length of use, distance from radiation source, energy required to penetrate the body part, and lead shielding utilized. 7,29 Radiation exposure to the surgeon during hand surgery with the mini c-arm over a 5-month period has been reported to account for less than 3% of the annual recommended maximum exposure for the epigastric region, thyroid, and hands. 35 Of note, the use of a mini c-arm as opposed to a large c-arm does not result in decreased radiation exposure to the surgeon, and in fact, the mini c-arm has been shown to be associated with increased radiation scatter. 7,30 Given the limited time required for confirmation of suture button placement and the surgeon’s ability to keep his or her hands outside the direct radiation, the radiation exposure associated with the addition of intraoperative fluoroscopy for suture button confirmation may be lower than that reported for hand surgery.
Among the several strengths of this study are that it was a prospective study involving experienced sports medicine–trained orthopaedic surgeons well-versed in using suspensory fixation for femoral fixation in ACL surgery. The deployment of the button was performed according to industry standards and capitalized on the experience of the surgeons involved. A shortcoming of this study is that it did not evaluate whether there are changes between intraoperative fluoroscopic images and any postoperative radiographs. Doing so would allow for evaluation of whether the steps taken to rectify the deployment errors resulted in permanent correct suture button positioning. Additionally, the 3 orthopaedic surgeons in this study were aware of the study hypothesis, introducing a potential source for bias.
Overall, this study demonstrates a high rate of incorrectly positioned suture buttons and indicates that the manual method is not completely reliable. Intraoperative fluoroscopic imaging is shown to be an effective method to both identify the malposition and allow the surgeon to rectify the problem before the final graft fixation. These results advocate for the routine verification of proper adjustable loop suspensory device positioning on the lateral femoral cortex. In our study, intraoperative fluoroscopy was used to identify and rectify suture button deployment errors in suspensory fixation of ACLR.
Footnotes
Notes
Final revision submitted August 16, 2020; accepted September 14, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: C.E. has received education payments from Arthrex, consulting fees from DePuy/Medical Device Business Services, and honoraria from Musculoskeletal Transplant Foundation. K.C. has received consulting fees from Arthrex, Johnson & Johnson, and DePuy. R.A.A. has received research support from Arthrex, education payments from DePuy, consulting fees from Biorez, and honoraria from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Connecticut (ref No. 011192).