
Abstract
Background:
The biomechanical properties of the 1.2-mm suture tape have outperformed conventional sutures in previous studies.
Purpose:
To compare the loop and knot security of 2 tape-type and 1 cord-type sutures using different arthroscopic knot techniques.
Study Design:
Controlled laboratory study.
Methods:
The biomechanical characteristics of the 1.2-mm tape, 2.0-mm tape, and 0.5-mm No. 2 suture were compared using 4 different knot types: 2 sliding knots (Samsung Medical Center [SMC] and Tennessee) and 2 nonsliding knots (2-throw surgeon’s and 2-throw square) with 2 and 3 additional reverse half-hitches on alternating posts (RHAPs) in a closed-loop system on a materials testing device. Each configuration was tested for loop security (maximal load applied between 0 and 3 mm of displacement), knot security (ultimate failure load), and failure mode with cyclical loading (30 N load for 20 cycles at 1 cycle per sec until failure). Loop and knot security among the configurations were compared using an analysis of variance.
Results:
With 2 RHAPs, the 2.0-mm tape showed significantly greater loop security than the 1.2-mm tape and suture (P = .001). With 3 RHAPs, the loop security of the suture was significantly superior compared with the 1.2-mm tape (P = .010). Regarding knot security, with 2 RHAPs, the 2.0-mm tape was significantly better than the 1.2-mm tape and suture (P < .001), while with 3 RHAPs, the suture was significantly superior to the 1.2-mm tape (P = .012). Using a square knot with 2 RHAPs, the 2.0-mm tape had significantly greater loop security (P = .001) and better knot security (P = .001) to the 1.2-mm tape and suture. Using the Tennessee knot with 2 RHAPs, the 1.2-mm tape had less loop security (P = .011) and knot security (P = .005) than the suture. Using the SMC knot with 3 RHAPs, the 2.0-mm tape and suture were significantly superior in loop security (P = .001) and knot security (P < .001) to the 1.2-mm tape. There was no significant difference in the failure mode between tapes and sutures with 2 and 3 RHAPs.
Conclusion:
With 2 RHAPs, the 2.0-mm tape demonstrated greater resistance to suture loop displacement and better knot security compared with the 1.2-mm tape and suture. However, with 3 RHAPs, the 1.2-mm tape manifested weaker loop and knot security compared with the suture.
Arthroscopic rotator cuff repair is a widely performed surgery using numerous knot techniques, suture materials, and devices. At the beginning of this century, suture materials included silk, chromic gut, Dacron, cotton, nylon, and stainless steel, among many others. More recently developed sutures include biodegradable polydioxanone, Maxon, Vicryl, Dexon, and polycaprolactone. In contrast, nonabsorbable sutures were predominantly braided polyester, with or without a polybutylate coating, for improved handling (Ethibond versus Mersilene). A core of several ultrahigh molecular weight polyethylene (UHMWPE) sutures surrounded by braided polyester and coated with silicon was introduced as FiberWire by Arthrex and revolutionized suture strength and production. Because of the demand for high-strength UHMWPE materials, other companies have also introduced pure braided UHMWPE sutures under various brand names. A combination of UHMWPE and biodegradable polydioxanone introduced as OrthoCord offered high strength and biodegradable properties. UHMWPE suture with a silicon central core and NaCl was introduced to improve knot security (DynaCord). Tapes and sutures were also made available in different sizes. 9
Suture tape is a braided construction of UHMWPE fiber blended with fibers of 1 or more long-chain synthetic polymers, preferably polyester. Tape sutures are useful in rotator cuff repair cases with the intention to maximize the contact pressure at the footprint and secure tissue.20,25,26 Biomechanical studies have reported better results for the 2.0-mm tape than the No. 2 suture, exhibiting higher failure load1,5,10,12,20 and tendon-to-bone contact pressure.12,20,21 In addition, the No. 2 suture with UHMWPE solid core has a considerably higher incidence rate of glove tears and subsequent finger lacerations. 14 Conversely, tape has a flat core covered in a braided jacket and is less abrasive on tendon fibers than regular form sutures.6,24
Several studies have compared the application of tape and suture using different knot-tying techniques.1,10,19,20 They have used surgeon’s knots 19 and square knots, 1 various stitches (eg, whip stitch, Krackow), 10 and inverted mattress configuration using a knotless suture anchor. 20 In previous studies, the biomechanical properties of the 2.0-mm tape outperformed those of sutures.10,19,20 The superior biomechanical properties of suture tape included higher contact pressure, load to failure, and stiffness and smaller gap formation, as indicated in a systematic review and meta-analysis. 2 However, no biomechanical study has been conducted combining various knots using alternating reverse half-hitches on alternating posts (RHAPs). Many surgeons prefer tape with a smaller width (1.2 mm), as it may have better sliding capability and lesser knot stack height than tapes with broader width. 31
In this study, we aimed to compare loop security (maximal load applied between 0 and 3 mm of displacement) and knot security (ultimate failure load) of 2 tape-type sutures and 1 conventional No. 2 suture using different arthroscopic knot techniques and different RHAPs. We hypothesized that there would be statistically significant differences in the biomechanical properties of the sutures tested.
Methods
In this study, we evaluated the loop and knot security of 2 tape-type sutures (1.2-mm and 2.0-mm braided UHMWPE sutures) and 1 cord-type suture (0.5-mm No. 2 braided UHMWPE suture) using 4 different widely used knot types: 2 sliding knots (Samsung Medical Center [SMC] 15 and Tennessee 11 ) and 2 nonsliding knots (2-throw surgeon’s 8 and 2-throw square 1 ) (Figure 1). Both threads—XbraidTT (tape-type) and Force Fiber (cord-type)—were pulled from an ICONIX anchor (Stryker). Each of these knots was tied with 2 or 3 RHAPs because knots tested needed at least 2 additional half-hitches. 17 Also, 2 and 3 RHAPs are usually performed in clinical practice.
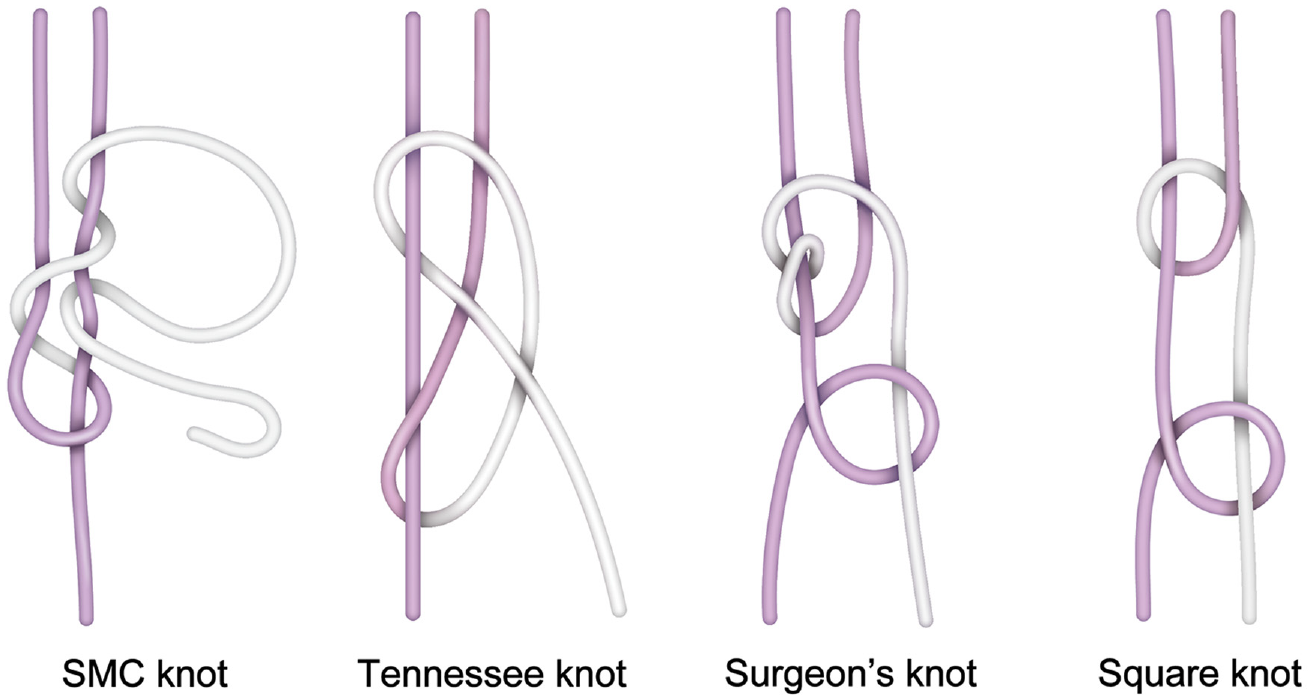
Schematic illustration of the 2 sliding knots (Samsung Medical Center [SMC] and Tennessee) and 2 nonsliding knots (2-throw surgeon’s and 2-throw square) tested.
Power analysis (G*Power Software Version 3.1.9.4, Franz Faul, University of Kiel) indicated that a sample size of 12 per knot/suture iteration was required to detect a clinically significant difference in ultimate failure load (a 25% difference in ultimate failure load; alpha error, .05; beta error, 0.2; dropout, 20%) based on previous studies.20,27 Thus, 288 experiments were conducted by tying the 3 types of sutures and the 4 knot-tying methods with the 2 and 3 RHAPs.
To reduce variability, all knots were tied by a single attending surgeon (S.W.C.) with experience in arthroscopic knotting techniques. The surgeon practiced tying each knot over 20 times before creating knot/suture iterations. To effectively simulate arthroscopic conditions, all sutures were moisturized with normal saline to facilitate the technical ease of tying sutures to mitigate friction just before knot tying. All knots were tied around two 10 mm–circumference smooth stainless-steel rods with the standard arthroscopic techniques using a single-hole standard knot pusher (Linvatec) through a cannula. Each knot was tensioned by pastpointing and overpointing to improve knot security and reduce slack between throws. 4
All knots were tested in a closed-loop system on a servohydraulic universal materials testing machine (AGS-X trapezium system; Shimadzu) (Figure 2). Instead of measuring displacement at ultimate failure, 16 loop security was measured by the load to clinical failure (N), defined as the maximal load applied between 0- and 3-mm displacement of the suture, as described in several previous studies.3,27 For knot security, all knots were subject to ultimate failure load (N), defined as the maximal load at which the suture loop maintained a holding capacity before it failed, either by suture breakage or knot slippage. 16 Suture breakage meant material failure, which occurred with the knot intact (ie, the loop holding strength of the knot was stronger than the tensile strength of the suture material), while knot slippage referred to complete slippage of the suture loop (ie, the tensile strength of the suture material was stronger than the loop holding strength of the knot) (see Supplemental Video). 16 Each mode of failure was recorded.

Tested knot on a universal materials testing machine. (A) 1.2-mm tape-type suture was tied around two 10 mm–circumference rods. (B) The complete setting of a tested knot in a closed-loop system.
All sutures were preconditioned with a force of 5 N at a zero-starting point. The suture loop was mounted to 2 testing rods with an even distribution of tension without loosening. Before testing, knot position and slippage were rechecked. After the sutures were preloaded, they were pulled apart by a 30-N load for 20 cycles at the rate of 1 cycle per second until failure. Data from a load-to-failure test were automatically collected with an acquisition system. 18
Statistical Analyses
Data were analyzed using SPSS Version 27 (IBM) with the significance level set at P = .05. One-way analysis of variance (ANOVA) and 2-way ANOVA were used to compare the loop security (the maximal load applied between 0 and 3 mm of displacement) and knot security (the ultimate failure load) according to suture and knot types and to evaluate any possible interactions between these types. Tukey post hoc tests were performed for significant differences. Logistic regression was used to analyze the mode of failure.
Results
Loop Security
The 2.0-mm tape showed significantly greater loop security than the 1.2-mm tape and suture in cases of 2 RHAPs (P = .001). The suture showed significant superiority with 3 RHAPs than the 1.2-mm tape (P = .010). When comparing knot types, the square knot had better loop security than the surgeon’s knot in cases of 2 RHAPs (P < .001). SMC knots had better security than surgeon’s, Tennessee, and square knots with 3 RHAPs (P < .001). There was a significant interaction between suture and knot types with 2 (P < .001) and 3 RHAPs (P = .003).
Using a square knot with 2 RHAPs, the 2.0-mm tape had significantly greater loop security (P = .001) than the 1.2-mm tape and suture. Using the Tennessee knot with 2 RHAPs, the 1.2-mm tape had lesser loop security (P = .011). Using the SMC knot with 3 RHAPs, the 2.0-mm tape and suture were significantly superior in loop security (P = .001) to the 1.2-mm tape. Using the surgeon’s knot with 3 RHAPs, the 1.2-mm tape was significantly superior in loop security (P = .005) to the 2.0-mm tape and suture (Table 1).
Comparison of Maximal Load (N) Applied Between 0 and 3 mm of Displacement Among Sutures Tested a

Data are presented as mean ± SD. Bold P values indicate statistically significant differences among the groups (P < .05). Dashes indicate areas not relevant. NS, not significant; RHAPs, reversed half-hitches on alternating posts; SMC, Samsung Medical Center.
Knot Security
With 2 RHAPs, the 2.0-mm tape showed significantly greater knot security compared with the 1.2-mm tape and suture (P < .001). With 3 RHAPs, the suture was significantly superior in knot security to the 1.2-mm tape (P = .012). The square knot had better security than the Tennessee knot, and the surgeon’s knot and the SMC knot were better than the surgeon’s knot with 2 RHAPs (P < .001). The SMC knot had better security than the surgeon’s, Tennessee, and square knots with 3 RHAPs (P < .001). There was a significant interaction between suture and knot types with 2 RHAPs (P < .001) and 3 RHAPs (P = .002).
Using square knots, with 2 RHAPs, the 2.0-mm tape had significantly better knot security (P = .001) compared with the 1.2-mm tape and suture. Using the Tennessee knot with 2 RHAPs, the 1.2-mm tape had lesser knot security (P = .005) than the suture. Using the SMC knot with 3 RHAPs, the 2.0-mm tape and suture were significantly superior in knot security (P < .001) to the 1.2-mm tape (Table 2).
Comparison of Ultimate Failure Load (N) Among Sutures Tested a

Data are presented as mean ± SD. Bold P values indicate statistically significant differences among the groups (P < .05). Dashes indicate areas not relevant. RHAPs, reversed half-hitches on alternating posts; SMC, Samsung Medical Center.
Mode of Failure
There was no significant difference in the mode of failure between tapes and sutures with 2 RHAPs (P≥ .999) and 3 RHAPs (P = .856) (Table 3).
Mode of Failure a

Data are presented as n (%). RHAPs, reversed half-hitches on alternating posts; SMC, Samsung Medical Center.
Discussion
The main findings from our study demonstrated that the 2.0-mm tape had better loop (P = .001) and knot (P < .001) security than the 1.2-mm tape and the No. 2 suture when backed up with 2 RHAPs. However, the No. 2 suture demonstrated superior loop (P = .010) and knot (P = .012) security to the 1.2-mm tape in the 3-RHAP groups. Using the SMC knot with 3 RHAPs, the 2.0-mm tape and suture were significantly superior in the loop (2.0 mm: 193.9 ± 42.59 vs suture: 229.16 ± 54.46 vs 1.2 mm: 103.82 ± 20.67; P = .001) and knot security (2.0 mm: 336.83 ± 42.99 vs suture: 284.05 ± 19.04 vs 1.2 mm: 166.88 ± 59.66; P < .001) to the 1.2-mm tape.
Loop security is the tightness of the suture loop. 3 It refers to the integrity of the initial knot at “time zero.” 7 In other words, it is the ability to conserve loop diameter when the knot is being tied. It depends on tensile properties, like failure load, elasticity, or plasticity of the suture material, which are concerned with suture elongation. 22 Previous works have suggested that 3 mm of displacement of a knotted suture loop constituted clinical failure because of a loss of tissue apposition.3,27 Kim et al 16 defined this as a load to clinical failure. This study borrows this concept and measures the maximal load applied between 0- and 3-mm displacement of the suture for loop security.
Knot security refers to the ability to resist breakage and slippage. 29 It is also a critical component in maintaining the integrity of suture ties. Several factors—including initial knot configuration, slack between throws, coefficient of friction, internal interference, suture pliability, and backup RHAPs—affect the tightness and the knot-slip resistance under tensile force.7,19,23 This study is conducted based on these concepts, and the results show that the 2.0-mm tape has better loop and knot security than the suture in the 2 RHAPs, and the suture has superior security compared with the 1.2-mm tape in the 3 RHAPs.
Nonsliding knots have better mechanical performance than sliding hand-tied knots when using absorbable filament suture.29,30 However, recent studies7,28 reported that arthroscopic sliding knots have comparable or better loop and knot security. With respect to loop security, arthroscopic sliding knots are considered to be better than nonsliding knots because sliding knots with an internal locking mechanism avoid significant gaps in additional locking half-hitches. 28 Regarding knot security, the initial slip knot of SMC 15 and Tennessee 11 is fastened inside the joint, which allows better sliding capability because of the lower coefficient of friction. Also, with nonsliding knots, it is often difficult to make a secure tendon approximation in arthroscopic surgery using a knot pusher. 16 In this experiment, the SMC knot demonstrated better knot and loop security than other knots with 3 RHAPs. Moreover, the 2.0-mm suture tape showed increased security using the square knot with 2 RHAPs and the SMC knot with 3 RHAPs. Using the Tennessee knot, the 1.2-mm tape had significantly lesser loop security and lower knot security than the suture. Considering that the 2.0-mm tape is thicker than other sutures, it makes sense that the intrinsic unraveling tendency of the 2.0-mm tape may have influenced the optimized configurations for arthroscopic knots. 13
Previous studies concluded that having at least 1 RHAP was essential to prevent slippage and improve loop and knot security.17,23 There was a consensus that arthroscopic knot should be backed up with at least 3 additional half-hitches for optimal security.7,17,18,27 In this study, every suture using an SMC knot with 3 RHAPs exceeded 100 N, similar to a previous study. 17 Also, significant interactions between suture and knot types were found in both loop and knot security with 2 and 3 RHAPs. These findings indicate that the optimized security for sutures requires proper arthroscopic knot techniques with secure additional half-hitch combinations.
No difference was found in the failure mode between suture types. Kim et al 17 found that the failure mode changed from knot slippage to suture breakage as additional half-hitches were added. This is partially consistent with our study. Suture breakage increased with the increase in the number of RHAPs when making SMC knots with the 2.0-mm tape and when making SMC and square knots with sutures. These findings may help surgeons to select proper arthroscopic knot techniques depending on the type of sutures.
Limitations
This study has several limitations. First and foremost, loop security tests used the worst-case scenario in the previous study, 18 resulting in an indirect measurement without evaluating the elongation 3 after 5 N preload. However, this study considered possible clinical loop failure in arthroscopic surgery. Second, one experienced attending surgeon makes the entire knot. However, the surgeon practiced tying each knot over 20 times before creating knot/suture iterations, and 1 experimenter can reduce variability. Third, this study compared only 2 sutures from the same company. However, this study aimed to evaluate the inherent biomechanical performance of suture materials in various knot techniques. Fourth, although cyclic tests can resemble clinical conditions, no biomechanical study can ever have an in vivo effect. When the tissue has healed, the suture might not be needed; this is true “time zero.”
Conclusion
With 2 RHAPs, the 2.0-mm tape demonstrated greater resistance to suture loop displacement and better knot security than the 1.2-mm tape and the No. 2 suture. However, with 3 RHAPs, the 1.2-mm tape demonstrated weaker loop and knot security than the suture.
Footnotes
Acknowledgements
The authors appreciate So Jung Shin and Son Donghee, MS, for their support with data analysis. Stryker provided threads from the ICONIX anchor used in this study.
Final revision submitted May 1, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This paper was supported by Konkuk University in 2023. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.