
Abstract
Background:
Superior labral anterior and posterior (SLAP) tears are a common finding in overhead athletes. The original classification system produced by Snyder in 1990 contained 4 types of SLAP tears and was later expanded to 10 types. The classification has been challenging because of inconsistencies between surgeons making diagnoses and treatments based on the diagnosis. Furthermore, patient factors—such as age and sports played—affect the treatment algorithms, even across similarly classified SLAP tears.
Purpose:
To (1) assess the interobserver and intraobserver reliability of the Snyder and expanded SLAP (ESLAP) classification systems and (2) determine the consistency of treatment for a given SLAP tear depending on different clinical scenarios.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 20 arthroscopic surgical videos and magnetic resonance imaging scans of patients with SLAP tears were sent to 20 orthopaedic sports medicine surgeons at various stages of training. Surgeons were asked to identify the type of SLAP tear using the Snyder and ESLAP classifications. Surgeons were then asked to determine the treatment for a SLAP tear using 4 clinical scenarios: (1) in the throwing arm of an 18-year-old pitcher; (2) in the dominant arm of an 18-year-old overhead athlete; (3) a 35-year-old overhead athlete; (4) or a 50-year-old overhead athlete. Responses were recorded, and the cases were shuffled and sent back 6 weeks after the initial responses. Results were then analyzed using the Fleiss kappa coefficient (κ) to determine interobserver and intraobserver degrees of agreement.
Results:
There was moderate intraobserver reliability in both the Snyder and ESLAP classifications (κ = 0.52) and fair interobserver reliability for both classification systems (Snyder, κ = 0.31; ESLAP, κ = 0.30; P < .0001) among all surgeons. Additionally, there was only fair agreement (κ = 0.30; P < .0001) for the treatment modalities chosen by the reviewers for each case.
Conclusion:
This study demonstrated that SLAP tears remain a challenging problem for orthopaedic surgeons in diagnostics and treatment plans. Therefore, care should be taken in the preoperative discussion with the patient to consider all the possible treatment options because this may affect the postoperative recovery period and patient expectations.
Keywords
Superior labral anterior and posterior (SLAP) tears were first described in 1985 by Andrews et al. 4 A SLAP tear indicates a lesion of the superior aspect of the labrum, both anterior and posterior, to the attachment of the long head of the biceps tendon. 14 Clinical suspicion of a SLAP tear can be further investigated with advanced imaging such as a magnetic resonance imaging (MRI) scan or, more specifically, an MR arthrogram.3,13 Direct visualization via a diagnostic shoulder arthroscopy is considered the gold standard for an accurate diagnosis.
The type of SLAP tear is typically classified using the Snyder classification system. The Snyder classification system includes 4 types of SLAP tears denoted by types I through IV. 16 These types include type I, which is fraying of the superior labrum free edge with a stable biceps tendon; type II, which involves the labrum and biceps tendon detaching from the top of the glenoid; type III, which is a bucket-handle tear with an intact biceps tendon; and type IV, which includes a displaced bucket-handle labral tear with extension into the biceps tendon root. 14 The most prevalent type of SLAP tear is type II. 17 Additionally, there have been expansions to the classification system by Morgan et al, 12 Maffet et al, 11 and Powell et al. 14 These inclusions introduced SLAP tear subtypes and combined lesions to the classification system. This is termed the expanded SLAP (ESLAP) classification system, and it ranges from type I to type X to classify specific lesions of the labrum better. Table 1 demonstrates the different types of SLAP tears along with proposed treatments given the type of tear, and Figure 1 illustrates each type of SLAP lesion. Although this expansion has allowed for more diagnostic options, the accuracy of diagnosing these tears remains challenging, and variability among providers still exists when it comes to formulating an accurate diagnosis and treatment plan.

SLAP, superior labral anterior and posterior.

Illustrations of SLAP tear lesions: (A) Type I to type IIc. (B) Type III to type VIII. (C) Type IX and type X. SLAP, superior labral anterior and posterior.
The expansion of the classification system may have added more detail to the diagnostic ability of the practitioner, although little is known about how reliably a clinician can use them to make the diagnosis. In addition, neither the Snyder nor ESLAP classification systems provide prognostic value to the provider when patient factors such as age and activity level are considered. This leads to a lack of consensus when determining treatment plans for specific subtypes of SLAP tears. Moreover, SLAP tears are difficult to diagnose with MRI or MR arthrography alone and challenging to consistently classify arthroscopically. 15 It was found that MRI and MR arthrography have a reported sensitivity and specificity range of 66% to 98% and 13% to 89%, respectively. 2 Therefore, making a definitive diagnosis on advanced imaging alone may be challenging. This can contribute to the variability between providers when attempting to classify these lesions based on imaging properly.
Surgical management of SLAP tears depends on the type of tear and patient-specific factors. Each type of SLAP tear may be treated using an arthroscopic approach, demonstrated in Table 1. Furthermore, patient factors—such as age, activity level, and the patient’s dominant arm—help guide the treatment plan for different types of SLAP tears. For example, it has been shown that older patients have a higher failure rate when treated with surgical intervention, especially in type II SLAP tears. However, younger patients participating in sports with repetitive overhead motions benefit more from debridement or complete repair of these tears. 6 Therefore, surgical management decisions are multifactorial, and much debate surrounds the appropriate treatment plan for these lesions.
The present study has 2 objectives. First, this study aimed to assess the interobserver and intraobserver variability among fellowship-trained orthopaedic sports medicine surgeons using the Snyder and ESLAP classification systems based on intraoperative arthroscopic video recordings, MRIs, and patient vignettes to investigate the reliability of the Snyder and ESLAP classification systems. The second aim of this study was to determine the agreement among these same surgeons regarding the definitive treatment for each clinical scenario.
Methods
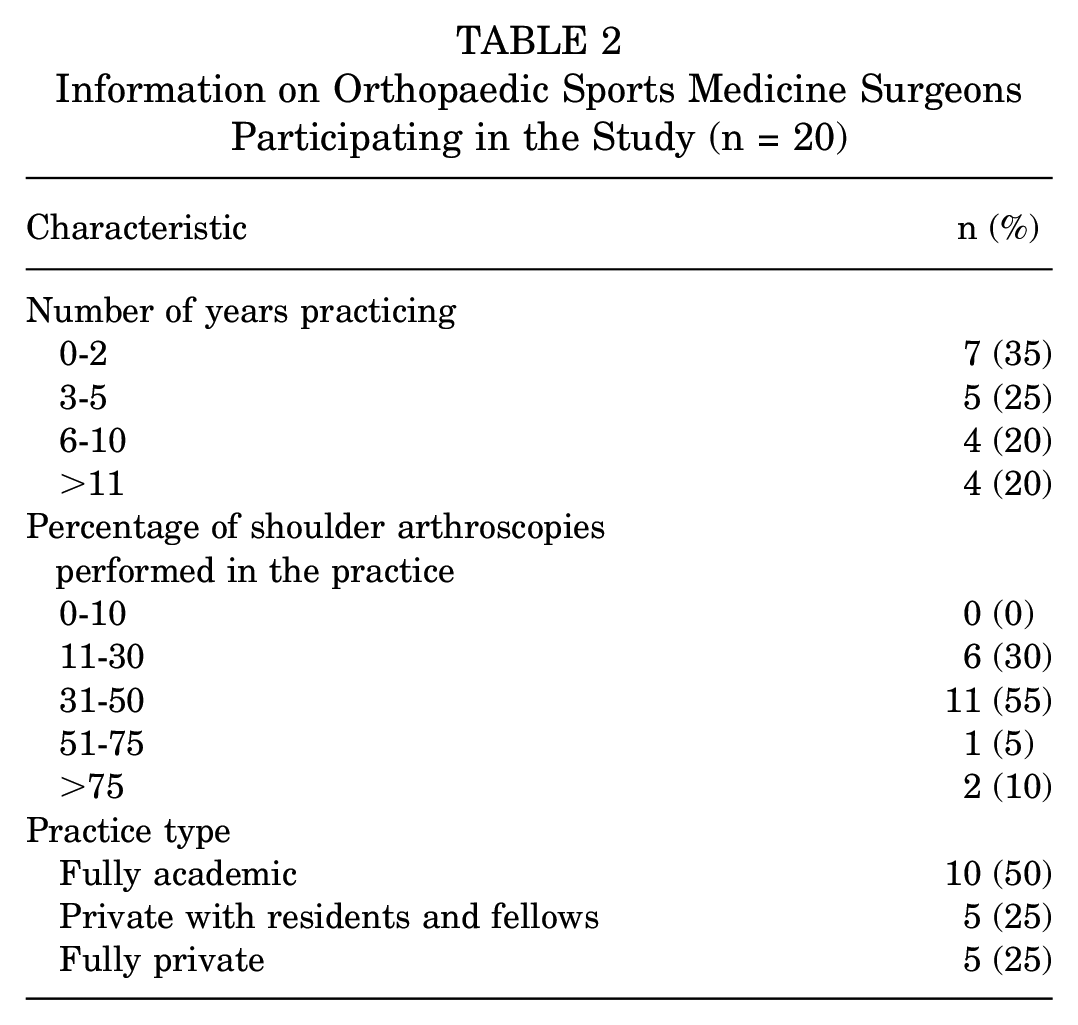
Institutional review board approval was waived for this study. A total of 20 intraoperative arthroscopic video recordings and MRIs of patients with SLAP tears were sent to 20 fellowship-trained orthopaedic sports medicine surgeons at various stages of their practice. Table 2 shows information about the orthopaedic surgeons involved in the study, including the number of years they have practiced, the percentage of shoulder arthroscopies, and their practice type. The surgeons were asked to diagnose the type of SLAP tear using the Snyder and ESLAP classification systems. Surgeons were then asked to determine the treatment for a SLAP tear using 4 clinical scenarios: (1) in the throwing arm of an 18-year-old pitcher; (2) in the dominant arm of an 18-year-old overhead athlete; (3) a 35-year-old overhead athlete; (4) or a 50-year-old overhead athlete. Treatment options did not include intervention, debridement, SLAP repair, biceps tenodesis, biceps tenotomy, or SLAP repair with biceps tenodesis. The responses were recorded for the surgeon's initial diagnosis and treatment. The cases were then shuffled and sent back 6 weeks after the initial responses and re-evaluated by each surgeon.
Information on Orthopaedic Sports Medicine Surgeons Participating in the Study (n = 20)
Statistical Methods
Interobserver reliability kappa coefficients (κ) were calculated using responses selected by the 20 raters upon 2 distinct reviews of the 20 cases for (1) Snyder classification types I to IV and (2) extended SLAP classification types I to X. Surgeon raters were offered 6 surgical modalities to choose as the preferred treatment for each case reviewed and further instructed to plan treatments based on 4 hypothetical patient conditions for each case (ie, varying ages paired with athleticism/activity levels at the time of injury). Interobserver reliability kappa coefficients (κ) were calculated using all rater responses for the 20 cases and reviewed twice for each of the 4 patient types. Results include unweighted kappa coefficients (κ) to assess the degree of agreement. The paired responses of each of the 20 reviewers were analyzed to evaluate intraobserver reliability and reported as simple kappa coefficients (κ) with standard error and 95% CIs.
Interobserver and intraobserver reliability were reported using the degree of agreement categories (based on kappa coefficient ranges) described by Landis and Koch. 10 A P value is associated with each kappa statistic, and P < .05 indicates that values differed significantly from zero and were not due to chance alone. Counts and percentages were scrutinized for each case scenario from both review sessions to determine consensus and observe trends among surgeon responses for each item. All raters’ responses were generated via independent surgeon reviews of cases during each of the survey sessions, with no communications or interactions with each other nor from the administering team. Analyses were performed in Statistical Analysis Software Version 9.4 (SAS Institute).
Results
Intraobserver Reliability of the Classification Systems
Most surgeons in this study had moderate intraobserver agreement when using the Snyder and ESLAP classifications (κ = 0.52). Two surgeons in this study had an almost perfect or substantial intraobserver agreement for all survey questions (κ = 0.81 and 0.71, respectively). Table 3 demonstrates the stratification of results based on intraobserver variability among the participating orthopaedic sports medicine surgeons.
Summary of Intraobserver Agreement Between Orthopaedic Sports Medicine Surgeons (n = 20) a

Degree of agreement is defined by the kappa coefficient: poor, ≤0; slight, 0.1-0.2; fair, 0.21-0.40; moderate, 0.41-0.60; substantial, 0.61-0.80; almost perfect, 0.81-0.99; perfect, 1.
Interobserver Reliability of the Classification Systems
Interobserver reliability was fair for both the Snyder and ESLAP classification systems (Snyder, κ = 0.31; ESLAP, κ = 0.30; P < .0001) among all surgeons. Additionally, there was only fair agreement (κ = 0.30; P < .0001) for the treatment modalities the reviewers chose for each case. Table 4 demonstrates the interobserver variability between participating orthopaedic sports medicine surgeons for the Snyder and ESLAP classification systems and treatment options.
Summary of Interobserver Agreement Based on Snyder Classification, Extended SLAP Classification, and Treatment Type a

SLAP, superior labral anterior and posterior.
Defined by the kappa coefficient: poor, ≤0; slight, 0.1-0.2; fair, 0.21-0.40; moderate, 0.41-0.60; substantial, 0.61-0.80; almost perfect, 0.81-0.99; perfect, 1.
Statistically significant (P < .05).
Clinical Scenarios and Treatments
The treatment options the surgeons chose based on the type of SLAP tear they diagnosed are shown in Table 5. The percentages represent the number of surgeons who chose the treatment modality after classifying that tear. Therefore, they are percentages of the total number of surgeons who classified the tear, which could be lower than the expected number of responses.
Most Common Treatment Options Chosen Based on Type of SLAP Tear and Clinical Scenario a
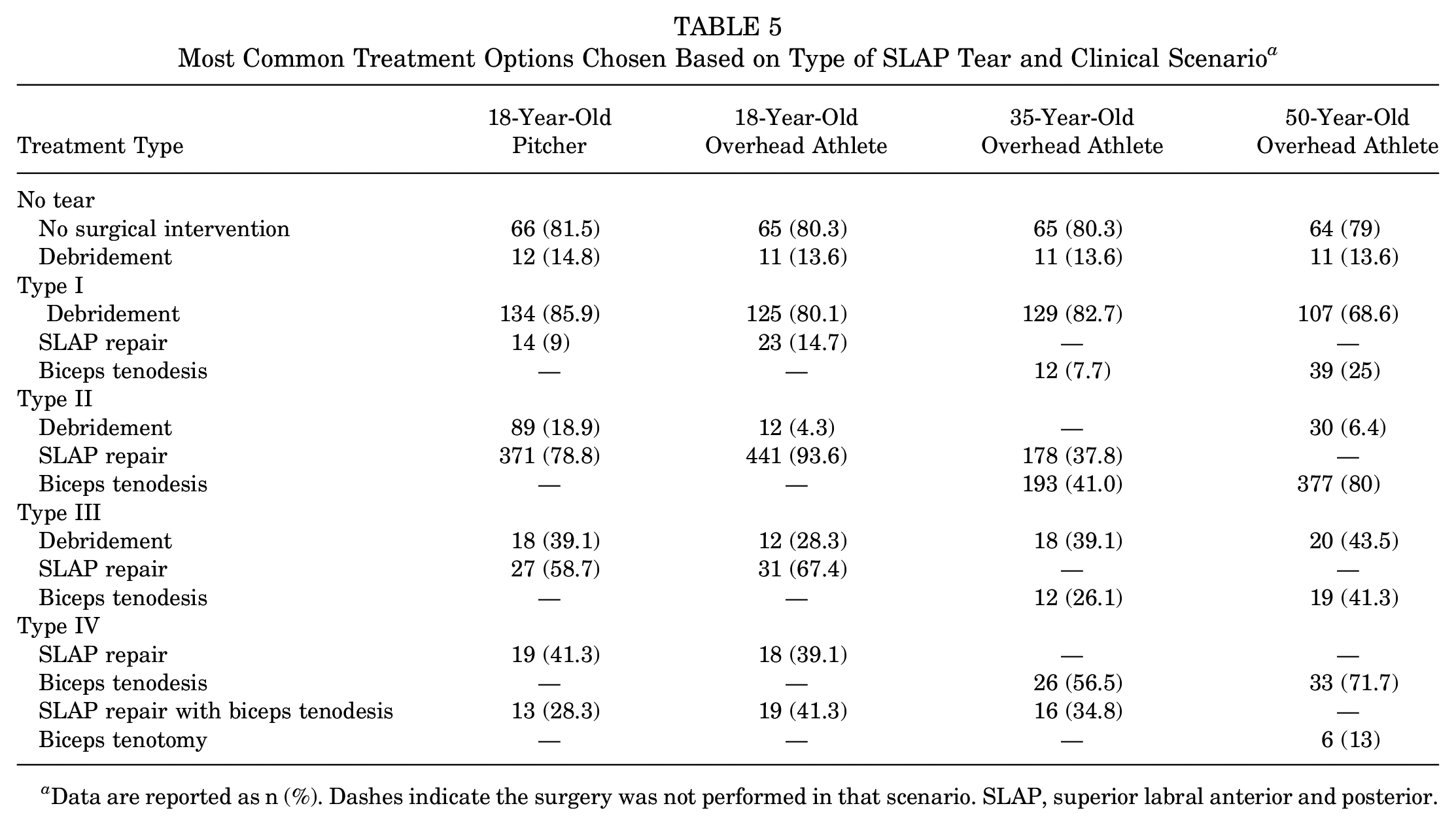
Data are reported as n (%). Dashes indicate the surgery was not performed in that scenario. SLAP, superior labral anterior and posterior.
No Tear/Normal Anatomy. For lesions diagnosed as “No tear,” there were consistent responses to either have no surgical intervention (79%-81.5%) or to perform debridement (13.6%-14.8%) across all clinical scenarios.
Type I Tears. Type I tears had a similar treatment response for the 18-year-old pitcher and the 18-year-old overhead athlete, which was debridement (85.9% and 80.1%, respectively) as a primary option. The second most popular option varied among the surgeons based on the clinical scenario, with SLAP repair (9% and 14.7%, respectively) selected for the 18-year-old pitcher and the 18-year-old overhead athlete. Debridement was the most popular option for older patients, both the 35-year-old and 50-year-old overhead athletes (82.7% and 68.6%, respectively). A biceps tenodesis was the preferred second option (7.7% and 25%, respectively).
Type II Tears. For type II SLAP tears, 93.6% of surgeons chose a SLAP repair in the 18-year-old overhead athlete, but only 78.8% would repair the same lesion in the 18-year-old pitcher. The second most common option for the 18-year-old overhead athlete and the 18-year-old pitcher was debridement (4.3% and 18.9%, respectively). Biceps tenodesis was the primary treatment option chosen for the 35- and 50-year-old overhead athletes (41% and 80%, respectively). The second most common treatment option in this group was either a SLAP repair for the 35-year-old (37.8%) overhead athlete or debridement for the 50-year-old overhead athlete (6.4%).
Type III Tears. In type III lesions, most surgeons chose either a SLAP repair (58.7% and 67.4%) or debridement (28.3% and 39.1%) in the 18-year-old pitcher and the 18-year-old overhead athlete. Most surgeons chose to debride both the 35-year-old (39.1%) and 50-year-old (43.5%) overhead athletes or opt to perform a biceps tenodesis (26.1% and 41.3%, respectively).
Type IV Tears. In type IV SLAP tears, most surgeons would attempt a SLAP repair in the 18-year-old pitcher (41.3%) or perform a SLAP repair with biceps tenodesis in the 18-year-old overhead athlete (41.3%). The second most common treatment option was a SLAP repair with biceps tenodesis in the 18-year-old pitcher (28.3%) and SLAP repair in the 18-year-old overhead athlete (39.1%). For the 35- and 50-year-old overhead athletes, most surgeons chose to do a biceps tenodesis (56.5% and 71.7%, respectively). The second most common option was a SLAP repair with biceps tenodesis for the 35-year-old overhead athlete (34.8%) and a biceps tenotomy for the 50-year-old overhead athlete (13%).
Discussion
The present study is unique in that we not only examined the interobserver and intraobserver reliability of the original Snyder and expanded SLAP classification systems, but we also asked the surgeon to develop a treatment plan based on 4 controversial clinical scenarios once they had made the diagnosis. Interobserver and intraobserver reliability for both diagnoses based on classification and treatment plans were seen to be less than optimal, highlighting a potential need to simplify classifications of these tears as expressed in Jia et al. 9 Previous studies, such as the studies by Wang et al 16 and Wolf et al, 19 also explored these lesions and the lack of reliability between visualizing and classifying them. Therefore, the differences and lack of consistency between our study and previous literature should help persuade the adoption of a simplified classification system described in a study by Jia et al 9 or a new classification system to diagnose SLAP tears.
Reliability of Classification Systems
The reliability of the Snyder classification system in diagnosing SLAP tears has been a popular research topic among sports medicine orthopaedic surgeons because of inconsistency in diagnosis, likely because of the difficulty with diagnostic imaging and intraoperative limitations. Jia et al 9 and Gobezie et al 8 analyzed the reliability and reproducibility of the Snyder classification system while diagnosing SLAP tears. Jia et al 9 found “moderate” to “substantial” intraobserver agreement and near “total agreement” for interobserver agreement while using the original Snyder classification system. Additionally, Gobezie et al 8 found that the intraobserver agreement was “moderate for both diagnosis and treatment.” The present study demonstrated some inconsistencies between surgeons when determining intraobserver and interobserver reliability. There was mainly “moderate” agreement when testing for intraobserver reliability. Moreover, the interobserver reliability was “fair” when analyzing both the Snyder and Expanded SLAP classification systems. These differences between studies are likely because of the larger cohort of orthopaedic surgeons used in this study compared with the studies by Jia et al 9 and Gobezie et al. 8 Additionally, the composition of physicians included in these studies differs as well, contributing to discrepancies in the reliability of data collected. Conversely, lower rates of reliability could be impacted by fair to good visualization of the superior labrum when using arthroscopic videos to assess labral tears, as demonstrated by Wolf et al. 19 Therefore, showing the current system in place still poses challenges to sports medicine orthopaedic surgeons in their decision-making process.
Treatment Based on SLAP Tear Type
Patient-specific factors strongly influence the difficulty of formulating a treatment plan for SLAP lesions. Specifically, age, activity level, and type of tear seem to contribute the most to formulating a treatment plan. 14 However, as demonstrated in this study, age seemed to be the most significant factor in treatment choice by surgeons. For example, for type I tears, debridement was the most common option for the younger and older population, allowing the surgeon to clean frayed fibers and restore a stable base. However, for type I tears, biceps tenodesis was the second most common choice in the older population when compared with SLAP repair in the younger population. This is because for patients aged 40 to 60 years, biceps tenodesis was hypothesized to assist with better cosmetic outcomes for patients and possible biceps tendinopathy. However, Aflatooni et al 1 showed no perceived cosmetic deformity for patients undergoing a biceps tenodesis compared with tenotomy. In the younger patient cohort, SLAP repair has been shown to contribute to good clinical outcomes and is accepted as the most common treatment option. Also, higher revision rates exist in older patients (>40 years) who undergo a SLAP repair. 5 Type II lesions followed a similar trend where patient age determined the treatment option chosen. For the younger population, a SLAP repair was the most common treatment chosen, and a biceps tenodesis was the most common treatment for the older population. Therefore, for each diagnosed SLAP tear, the patient's age in the clinical scenarios largely dictated the decision to proceed with a certain treatment.
Treatment options differ in overhead athletes and pitchers to return to previous activity because there are mixed results on the optimal treatment plan. For example, careful attention is taken when treating pitchers because of the force they produce on the labrum in the arm cocking phase of a pitch. 6 In this study, the 18-year-old overhead athlete and the 18-year-old pitcher had different treatment plans for each type of SLAP tear. Previous studies have laid the groundwork for return to play and return to prior performance in pitchers and position players participating in baseball.6,7 They suggest that surgical debridement of SLAP tears for pitchers may be more effective than complete repair, especially in type II lesions. 6 The findings in a study by Fedoriw et al 6 reflect the data of a higher rate of debridement for type II SLAP tears in the 18-year-old pitcher found in the present study when compared with the 18-year-old overhead athlete. Therefore, it showed an overall lower rate of repair and a higher rate of debridement in the pitcher when compared with the overhead athlete.
The treatment of type IV SLAP tears was also controversial in the present study between primary and secondary treatment options. The primary and secondary treatment options were almost split between the 18-year-old pitcher (41.3% vs 28.3%) and the 18-year-old overhead athlete (41.3% vs 39.1%). Additionally, the 35-year-old athlete also had a relatively split decision in treatment option choice (56.5% vs 34.8%). A reason for a split decision on the treatment option chosen may be the lack of visualization of the tear. For type IV lesions, the treatment algorithm is chosen based on the size of the biceps tendon tear. The surgeon can excise the detached fragments and repair the labrum if the tear is < 50% of the biceps tendon diameter. If the tear is >50% of the biceps tendon diameter, a tenotomy or tenodesis of the long head of the biceps is needed. 5 Possible discrepancies in treatment modalities chosen could be due to the lack of proper visualization. However, managing type IV SLAP tears in this study points to surgeons treating these tears more based on age, with younger patients being treated with a SLAP repair and tenodesis, while older patients are being treated with only a tenodesis. This is consistent with the current literature. Wang et al 18 also concluded in their study of the evaluation and treatment of SLAP lesions that age played a significant role in both performing a SLAP repair and biceps tenodesis.
Strengths and Limitations
The strengths of this study include the diversity of orthopaedic sports medicine surgeons involved in the study. Previous studies only included experienced surgeons and did not consider newly practicing surgeons (0-2 years in practice). In this study, 2 of the participants were newly practicing surgeons who had the highest intraobserver agreement (agreement of substantial or almost perfect). Furthermore, the surgeons in this study represented a diverse population of orthopaedic sports medicine surgeons who trained at multiple institutions. Additionally, this study analyzed responses from surgeons in different practice types, which allows for a more accurate translation to the general population of surgeons who may see these injuries.
The limitations of this study include the orthopaedic surgeons’ inability to evaluate the videotapes to determine whether they were of a high enough quality and resolution to allow them to make a confident diagnosis. A previous study required orthopaedic surgeons to rate the quality of the videotape and their confidence in making the diagnosis on an analog scale, and they found a positive correlation between the quality of the tape and the confidence in making the diagnosis. 9 Therefore, requiring the surgeons to do the same in this study could have served as both a quality control assessment and assurance in diagnosis. In addition, increasing the sample size of surgeons involved would have increased the power of the study. Although this study has a larger sample size than previous studies, studies by Jia et al 9 and Gobezie et al, 8 increasing the number of surgeons would have strengthened the results. Moreover, there is a possibility that the MRI did not give a complete visualization of the SLAP lesion. Since MRI produces images in predefined cuts, there is a chance the labrum was not optimally recognized for a proper diagnosis. Last, the actual diagnosis of the SLAP tear was unknown; therefore, the response of each provider was compared with the other responses. To strengthen the study, there should have been criteria set to properly diagnose each lesion before sending out the videotapes; this would have increased the validity of the responses.
Conclusion
This study demonstrated difficulty utilizing the Snyder and ESLAP classification systems when diagnosing SLAP tears and formulating a treatment plan because these lesions are difficult to diagnose with MRI and intraoperative visualization. The lack of preoperative confidence in diagnosing these lesions—as demonstrated by the intraobserver and interobserver variability in this study—with imaging alone can lead to a different treatment plan. Therefore, discussing all the options with the patient preoperatively is important to guide their postoperative expectations accordingly.
Authors
Alexander K. Hahn, MD, MS (Department of Orthopaedic Surgery, University of Connecticut, Farmington, Connecticut, USA); Kyle Holmberg, DO (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Jon E. Hammarstedt, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Frances Philp, MS (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Patrick DeMeo, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Vince J. Lai, MD (Department of Orthopedic Surgery, Mercy, Saint Louis, Missouri, USA); Michael Christopher Kindya, MD (Total Orthopaedic Care, Lauderdale Lakes, Florida, USA); James Michael Paci, MD (Orlin & Cohen Orthopedic Group, Smithtown, New York, USA); Lutul D. Farrow, MD (Department of Orthopaedic Surgery, Cleveland Clinic, Cleveland, Ohio, USA); Nicolas Vardiabasis, DO (ARC Orthopedic Group, West Hills, California, USA); Darin Nye, MD (Mercy Health-Tiffin Hospital, Tiffin, Ohio, USA); Steven Frey, MD (Reconstructive Orthopedics, Cherry Hill, New Jersey, USA); Vasilios Moutzouros, MD (Henry Ford Health, Detroit, Michigan, USA); Gregory J. Purnell, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Patrick Wang, MD (MidJersey Orthopaedics, Flemington, New Jersey, USA); Michael Vaccariello, MD (Sparrow Health System, Ionia, Michigan, USA); Scott K. Schweizer, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Dennis J. Phillips, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); Darren A. Frank, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA); and Sam Akhavan, MD (Department of Orthopaedic Surgery, Allegheny General Hospital, Pittsburgh, Pennsylvania, USA).
Footnotes
Final revision submitted May 15, 2023; accepted May 22, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: K.H. has received education payments from Mid-Atlantic Surgical Systems. V.J.L. has received grant support and education payments from Arthrex. M.C.K. has received education payments from Southern Edge Orthopaedics. J.M.P. has received nonconsulting fees from Arthrex; royalty or license from Arthrex; consulting fees from Arthrex, Endo Pharmaceuticals, Xiros, and Zimmer Biomet; education payments from Gotham Surgical and Endo Pharmaceuticals; hospitality payments from Smith & Nephew; and stock or stock options from Core Sports/Motus Global and OrthoCor. L.D.F. has received hospitality payments from DJO. N.V. has received hospitality payments from Stryker; education payments from Arthrex; and grant support from Arthrex. V.M. has received education payments from Arthrex and Pinnacle; consulting fees from Pacira Pharmaceuticals and Vericel; and hospitality payments from Smith & Nephew and Stryker. G.J.P has received consulting fees from Vericel. P.W. has received grant support from Arthrex; and hospitality payments from Smith & Nephew, Exactech, and Zimmer Biomet. M.V. has received education payments from Medwest. S.K.S. has received hospitality payments from Arthrex. D.J.P. has received education payments from Mid-Atlantic Surgical Systems; honoraria from Wright Medical; and research support from Arthrex. D.A.F. has received nonconsulting fees from Arthrex; consulting fees from Arthrex; education payments from Mid-Atlantic Surgical; and research support from Arthrex. S.A. has received nonconsulting fees from Arthrex; consulting fees from Arthrex; education payments from Mid-Atlantic Surgical; and royalty or license from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Allegheny Health Network.