
Abstract
Background:
The management of superior labrum anterior and posterior (SLAP) tears remains controversial, with surgical treatment options including SLAP repair, debridement, and open or arthroscopic biceps tenodesis (BT), based on patient factors and the type of tear.
Hypothesis:
We hypothesized that SLAP repair has become less frequently performed over time, while BT is more frequently performed, particularly in patients ≥ 40 years.
Study Design:
Descriptive epidemiology study.
Methods:
A retrospective query was performed using the Humana insurance database from years 2007 to 2016. For the management of a SLAP tear diagnosis (International Classification of Diseases–Ninth Edition [ICD-9] code: 840.7), independent and exclusive cohorts were formed using Current Procedural Terminology (CPT) codes for debridement (29822, 29823), SLAP repair (29807), open or arthroscopic BT (29828, 23430), and SLAP repair combined with BT (29828 OR 23430 AND 29807).
Results:
Of 46,650 diagnoses of a SLAP tear, there were 3347 patients who underwent operative management for an isolated SLAP tear from 2007 to 2016. There was a linear increase of SLAP tear diagnoses per year (r 2 = 0.800, P < .001) during this period. Overall, SLAP repair was performed in 1629 patients (48.7%), debridement was performed in 1076 patients (32.1%), BT was performed in 552 patients (16.5%), and combined SLAP repair and BT was performed in 90 patients (2.7%). There was a 69.3% decrease in isolated SLAP repair from 2007 to 2016 (r 2 = 0.882, P < .001). BT for the diagnosis of an isolated SLAP tear increased by 370.0% over the same period (r 2 = 0.800, P < .001). SLAP repair had an equivalent percentage of being performed in patients both older and younger than 40 years (P = .218). There was a 1500.0% increase in BT performed in patients older than 40 years during the study period. There were no statistical differences in the postoperative incidence of stiffness, surgical site infections, and reoperations between all surgical treatment groups (P > .05).
Conclusion:
An analysis of a large private-payer database revealed that surgical treatment of isolated SLAP tears in the United States has shifted from 2007 to 2016, with an increase in the frequency of BT and a decline in the frequency of SLAP repair, particularly in patients older than 40 years.
Our understanding of superior labrum anterior and posterior (SLAP) tears has grown substantially since their initial description in 1985. 3,34 SLAP tears are common in overhead athletes in which abduction and maximal external rotation motion of the overhead throw result in such tears via the “peel-back” mechanism. 8,9 Several other mechanisms have been proposed, such as traction forces resulting in inferior subluxation of the humeral head, internal impingement of the labrum with the undersurface of the rotator cuff, and altered biomechanics from posterior capsular contracture. 4,7 –9 SLAP tears may also be traumatic or degenerative and represent a common cause of shoulder pain and disability in the general population, with Snyder et al 33,34 reporting a SLAP tear prevalence of 6% in a series of 2375 patients undergoing shoulder procedures. Since their description, there has been considerable interest in SLAP tears and SLAP repair, with a documented increase in the frequency of SLAP repair from database information spanning multiple centers. 28,39,42
SLAP tears often occur with concomitant injuries such as rotator cuff tears, posterior labral tears, and Bankart lesions. 33 Treatment in such cases may be predicated on the most prominent defect, but the optimal treatment for managing a SLAP tear is of significant debate, especially with type 2 SLAP tears. 6 Nonoperative management is the initial treatment, as no injury is believed to be countered with acute surgery. 14,17,24 Classically, repair using suture anchors of the superior labrum has been the treatment of choice. 6,10,19 However, SLAP repair results have been quite variable in the literature, ranging from 40% to 94% good to excellent results and 20% to 94% return-to-play rates. 21 Furthermore, SLAP repair results have been reported to be poor in patients older than 35 to 40 years, in patients with workers’ compensation claims, and in patients involved in overhead-throwing sports. 6,12,16,32 An analysis of type 2 SLAP repair in a military population of 179 participants revealed a 37% failure rate, 28% revision rate, and higher chance of failure for patients older than 36 years. 32
Biceps tenodesis (BT) has been suggested as an alternative treatment for isolated type 2 SLAP tears, with early data showing superior satisfaction and ability to return to sporting activities for BT compared with SLAP repair. 5 Although high-level evidence such as prospective randomized controlled trials is lacking, several other studies of isolated SLAP tears have described similar or superior outcomes for BT compared with SLAP repair, particularly for patients aged between 36 and 40 years. 13,15,22,31 Using a cost-effectiveness model, evidence has even suggested that primary BT was more cost-effective than SLAP repair in a 40-year-old man. 29 Despite the literature from single institutions on the topic in recent years, recent national trends in the United States for the treatment of isolated SLAP tears have not been well described.
The purpose of this study was therefore to provide an updated analysis of trends in the surgical management of SLAP tears in the United States during the years 2007 to 2016 using data from a large private payer database. We hypothesized that for patients with a diagnosis of an isolated SLAP tear, SLAP repair became less frequent over time, whereas BT became more frequent. Furthermore, we hypothesized that age for SLAP repair became younger over time, with BT becoming more common in patients older than 40 years.
Methods
Database
The present study was a retrospective analysis employing the Humana insurance database available on PearlDiver (http://www.pearldiverinc.com). This database employs insurance records to store data on demographics, comorbidities, diagnoses, and procedures performed. These data are organized by International Classification of Diseases–Ninth Revision and –Tenth Revision (ICD-9 and ICD-10, respectively) diagnosis and procedure codes or Current Procedural Terminology (CPT) codes. Independent databases are compiled from Medicare and private insurers. Data obtained from this database are deidentified and were deemed exempt from institutional review board approval.
Population Cohorts
The present study accessed the Humana database from 2007 to 2016 for all diagnoses of a SLAP tear (ICD-9: 840.7; ICD-10: S43.431A, S43.432A, S43.439A). The Humana database’s diagnosis codes for a SLAP tear were combined with CPT procedure codes. Independent and exclusive cohorts were constructed using the following CPT codes: debridement (29822, 29823), SLAP repair (29807), open or arthroscopic BT (29828, 23430), and SLAP repair combined with BT (29828 OR 23430 AND 29807) (Table 1). In all cases, glenohumeral debridement codes (29822, 29823) were allowed in addition to the primary procedure code. Of note, biceps tenotomy is included within the billing code for glenohumeral debridement. Boolean search criteria were used to remove all concomitant shoulder procedures that were coded aside from these. Patient cohorts were adjusted to exclude the following concomitant shoulder procedures: rotator cuff repair (RCR) (29827), Bankart repair (29806), lysis of adhesions (29825), distal clavicle resection (29824), loose body removal (29819), partial synovectomy (29820), subacromial decompression (29826), and complete synovectomy (29821) (Table 1). A separate analysis was performed to analyze the incidence of SLAP repair or BT with concomitant RCR.
Boolean Search Criteria Used to Construct Cohorts of Surgical Management for Isolated SLAP Tears a

a CPT, Current Procedural Terminology; ICD-9/-10, International Classification of Diseases–Ninth Revision/Tenth Revision; SLAP, superior labrum anterior and posterior.
Study Outcomes
The population cohorts were analyzed for demographic differences with respect to age, sex, body mass index, smoking status, history of diabetes, and documented Charlson Comorbidity Index. The incidence of each procedure for the diagnosis of a SLAP tear was trended over the years analyzed within the study. The incidence of each procedure was reported as the number of procedures performed in a given year divided by the total number of SLAP tear diagnoses for that year. Specific complications were queried within the database based off ICD diagnosis codes. Specifically, surgical site infections (ICD-9/ICD-10: 998.51, 998.59, 996.66, 996.67, 730.01, 730.21, 730.81, 730.91, 711.01, 711.81, 711.91, 996.60, 996.69, T81.4XXA, K68.11, T81.4XXA, T85.79XA, T84.50XA, T84.60XA, T84.7XXA, T85.79XA, M86.119, M86.219, M86.619, M86.9, M90.819, M00.019, M01.X19) and stiffness (ICD-9/ICD-10: 719.50, M256.0, M256.11, M256.12, M256.19) were common to all procedures, and the postoperative incidence of either was queried within the database.
Statistical Analysis
Statistical analysis was performed using Stata 13.1 (StataCorp). A comparison of continuous variables was performed using 1-way analysis of variance, while categorical variables were performed using the chi-square test of independence. Linear regression was used to identify trends of each treatment modality.
Results
Between 2007 and 2016, there were 46,650 diagnoses of a SLAP tear based on ICD-9 and ICD-10 diagnosis codes, of which 19,485 underwent surgical management of the biciptal-SLAP complex (41.8%). There was a linear increase of 168.6% in SLAP tear diagnoses (r 2 = 0.800, P < .001) during the study period. After excluding concomitant procedures, there were 3347 cases (7.2%) of surgical treatment for isolated SLAP tears. Overall, SLAP repair was performed in 1629 patients (48.7%), debridement was performed in 1076 patients (32.1%), BT was performed in 552 patients (16.5%), and combined SLAP repair and BT was performed in 90 patients (2.7%).
During the study period, there was a 32.0% decrease in the proportion of SLAP tear diagnoses that underwent operative management with a procedure isolated to the SLAP tear, from 948 to 645 cases per 10,000 diagnoses (r 2 = 0.750, P = .001) (Figure 1). There was a 69.3% decrease in the proportion of SLAP tear diagnoses managed with SLAP repair (r 2 = 0.882, P < .001). There was a 16.6% increase in the proportion of diagnoses managed with isolated debridement (r 2 = 0.105, P = .294) and a 346.7% increase in combined SLAP repair with BT (r 2 = 0.041, P = .574), although neither had a linear correlation. There was a 370.0% increase in the proportion of diagnoses managed with isolated BT (r 2 = 0.800, P < .001).

Trends in the surgical management of superior labrum anterior and posterior (SLAP) tears over time per 10,000 diagnoses of a SLAP tear.
Demographic differences between patients undergoing each operative treatment are summarized in Table 2. Overall, there was a larger percentage of male patients (59.9%) undergoing debridement for SLAP tears versus female patients (40.1%). A pairwise comparison demonstrated that a statistically significantly greater percentage of female patients underwent debridement versus SLAP repair (40.1% vs 29.4%, respectively; P < .001) and combined SLAP repair and BT (40.1% vs 22.2%, respectively; P = .001). A greater percentage of female patients underwent BT versus SLAP repair (36.4% vs 29.4%, respectively; P = .003) and combined SLAP repair and BT (36.4% vs 22.2%, respectively; P = .012).
Demographics in Operative Management of Isolated SLAP Tears a

a Data are reported as n (%) unless otherwise indicated. BT, biceps tenodesis; SLAP, superior labrum anterior and posterior.
There was a statistically greater proportion of patients older than 40 years who underwent debridement versus SLAP repair (85.3% vs 50.7%, respectively; P < .001). A greater proportion of patients who underwent BT were older than 40 years in comparison with debridement (91.1% vs 85.3%, respectively; P = .001), SLAP repair (91.1% vs 50.7%, respectively; P < .001), and combined SLAP repair and BT (91.1% vs 77.8%, respectively; P < .001) (Figure 2). In patients older than 40 years, 40.1% underwent SLAP repair, 37.6% underwent debridement, 19.4% underwent BT, and 2.8% underwent combined SLAP repair and BT. In patients younger than 40 years, 79.2% underwent SLAP repair, 15.2% underwent debridement, 3.8% underwent BT, and 1.8% underwent combined SLAP repair and BT. There was a significantly lesser proportion of patients diagnosed with diabetes in the SLAP repair population compared with all other procedures (P = .017). Last, the Charlson Comorbidity Index was significantly less in the SLAP repair population compared with all other procedures (P < .001).

Distribution of operative treatments for superior labrum anterior and posterior (SLAP) tears in patients (A) younger and (B) ≥ 40 years.
A statistically greater proportion of patients older than 40 years underwent debridement, BT, and combined SLAP repair and BT compared with patients younger than 40 (P < .001). Only SLAP repair had an equivalent percentage of being performed in patients both younger and older than 40 years (P = .218). SLAP repair was the dominant treatment choice for patients aged 10 to 59 years, while debridement was the more common treatment choice patients 60 years and older. The change in age distributions for patients undergoing SLAP repair and BT is shown in Figure 3. Of note, 57.0% of all BT procedures in patients older than 40 years were performed from 2013 to 2016.

Trends in patients undergoing superior labrum anterior and posterior (SLAP) repair and biceps tenodesis stratified by age.
Stiffness was the most common complication with respect to all procedures (4.7% overall). There was no statistical difference between the incidence of stiffness, surgical site infections, and reoperations between the surgical treatment groups for isolated SLAP tears (P > .05 for all) (Table 3).
Complications Associated With Operative Management of Isolated SLAP Tears a

a Data are reported as n (%). BT, biceps tenodesis; SLAP, superior labrum anterior and posterior.
From a separate analysis of patients with a diagnosis of SLAP tears between 2007 and 2016, there were 14,558 patients who underwent isolated RCR, 1700 patients who underwent RCR and SLAP repair, and 2222 patients who underwent RCR and BT. The incidence of those undergoing isolated RCR increased by 12.8%, those undergoing RCR and SLAP repair decreased by 42.3%, and those undergoing RCR and BT increased by 1417.0% (Figure 4).
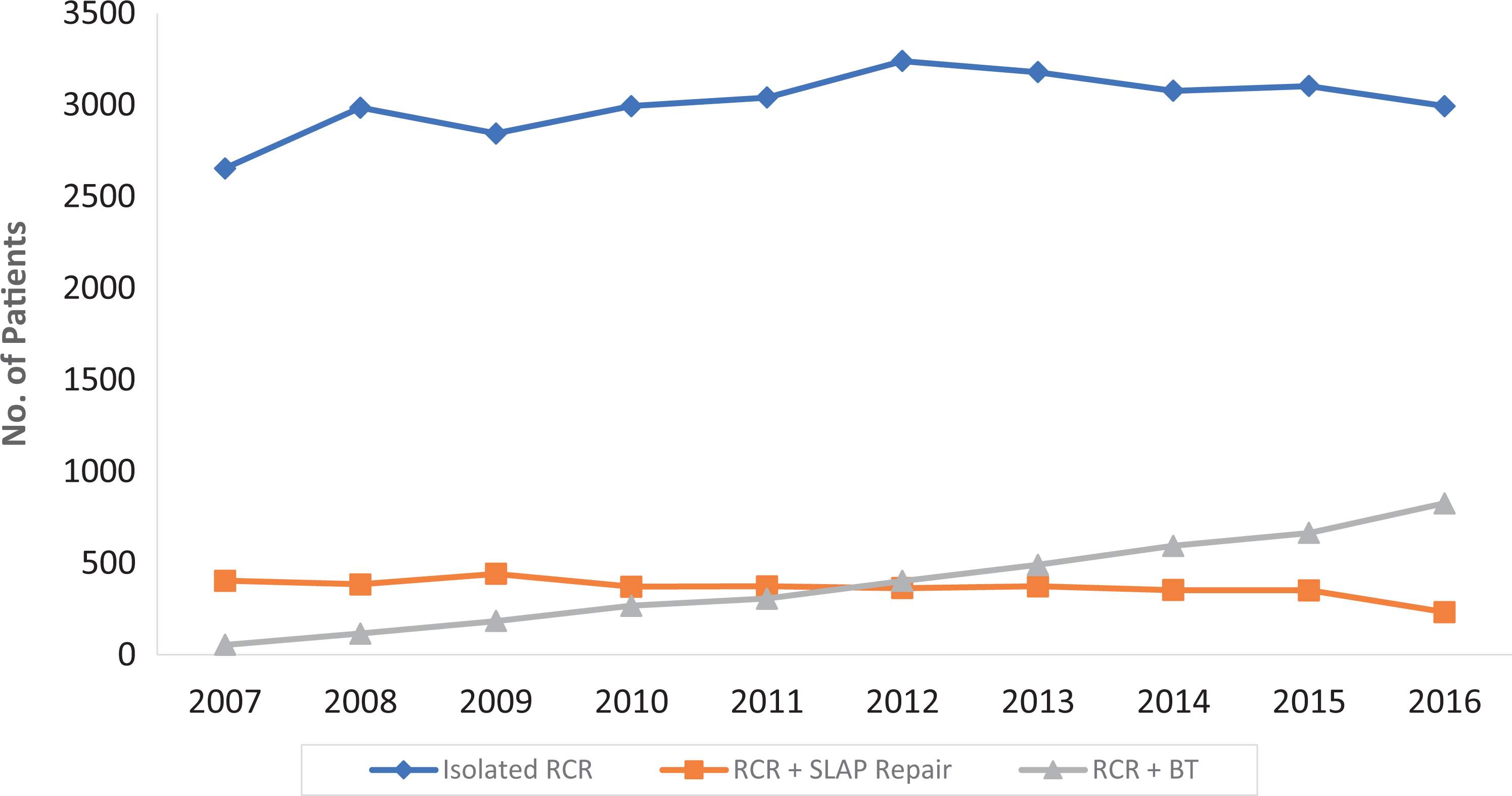
Trends in isolated rotator cuff repair (RCR), RCR with superior labrum anterior and posterior (SLAP) repair, and RCR with biceps tenodesis in the management of patients with diagnosed SLAP tears.
Discussion
The management of SLAP tears is noted to have changed significantly over the past decade. The operative management of isolated SLAP tears has decreased over time, while the number of diagnoses has increased. It is unclear whether this finding is a result of the increased number of diagnoses, a shift in management toward conservative treatment, or reluctance to operate without concomitant defects. However, in our relatively homogeneous population of isolated SLAP tear diagnoses, it is clear that the proportion of patients managed with BT has increased in frequency, whereas SLAP repair has decreased in frequency. A further analysis for age demonstrated a large increase in patients older than 40 years undergoing BT for this diagnosis over time. SLAP repair was still the predominant treatment in patients younger than 60 years. An analysis of trends in a national private-payer database of 46,650 SLAP tear diagnoses and 3347 procedures specifically for this abnormality demonstrated significant trends that reflect research regarding this defect.
Andrews et al 3 and Snyder et al 34 popularized SLAP tears as prevalent injuries in the overhead athlete. Yet, treatment options are challenging because of poor vascularity of the superior labrum, which decreases with age, 11,40 and the high functional demand of the athletic populations that sustain this injury. Repair of the superior labrum with suture anchors is the traditional mode of management. In isolated management of this injury in baseball players, Gilliam et al 20 reported improvement in functional outcomes, but pitchers had worse return-to-play rates than nonpitchers (59% vs 76%, respectively). BT has been discussed as an alternative procedure that is able to remove a significant pain generator within the glenohumeral joint and limit the peel back of the superior labrum. Werner et al 41 initially suggested this as a salvage procedure for failed SLAP repair, reporting improved functional outcomes and range of motion at 2-year follow-up after previous SLAP repair. BT has also been suggested as a reasonable primary procedure in middle-aged patients because of the reduced vascularity of the superior labrum in older patients and an increased risk of stiffness postoperatively. 23,25,27,38,40
Boileau et al 5 were the first to compare BT with SLAP repair in a heterogeneous population and found that a greater proportion of patients after BT were satisfied than after SLAP repair. A recent systematic review has demonstrated superior rates of patient satisfaction and return to sport in patients after BT when compared with SLAP repair, with moderate overall heterogeneity of articles. 23 A cost-effectiveness analysis between these 2 procedures for SLAP tears in middle-aged patients also revealed that BT is a more cost-effective strategy; however, this study assumed equal utilities gained from either procedure and can attribute these results primarily to the lower failure rate reported in the literature of BT. 29
The literature addressing modes of management regarding this topic has escalated within the past 10 years to provide appropriate indications for the management of all types of SLAP tears. 2 This is most appreciable by the finding that patients older than 40 years have the fastest rising incidence of BT. SLAP repair still remains the preferred option for younger patients, but it is important to note the decreasing incidence of this procedure for isolated tears. Provencher et al 32 have demonstrated up to 40% failure after SLAP repair in young active patients with a confirmed SLAP tear, while Waterman et al 36 reported that lower occupational demands and combined injury patterns were associated with improved outcomes in a military subset. These studies may suggest that clinicians are more sensitive to the high incidence of failure, which would cause some reluctance in performing this procedure without exhausting conservative measures. Additionally, numerous prospective studies have reported inferior outcomes for RCR when combined with SLAP repair over biceps tenotomy and glenohumeral debridement. 1,18,26 The present study’s finding that RCR with SLAP repair is decreasing relative to RCR with BT is substantiated by these studies.
Three studies demonstrated the rising incidence of SLAP repair performed in the United States during 2002-2010, 2004-2009, and 2002-2009 using the Statewide Planning and Research Cooperative System database from the New York State Department of Health, 28 the PearlDiver database, 42 and the Defense Medical Epidemiology Database, 37 respectively. These epidemiological studies demonstrate the increasing incidence of SLAP repair in their respective populations but lack a comparison of procedures, which may limit the conclusions that may be drawn toward surgeon decision making. This trend was not appreciated within the included years of our search; however, the search performed within this study excluded any concomitant procedures performed so that we could analyze a relatively homogeneous population. Furthermore, only Waterman et al 37 considered the rate of diagnosis of SLAP tears, which would increase the pool of patients who are eligible for operative management.
Patterson et al 30 performed a similar trend analysis using the American Board of Orthopaedic Surgery Certification Examination Database on both isolated SLAP lesions and those with concomitant RCR. Similar to the findings of the present study, this group found a decrease in the rate of SLAP repair and an increase in the incidence of BT performed for both isolated SLAP lesions and those with concomitant RCR. However, this database has high selection bias because it is constructed from case logs of candidate orthopaedic surgeons sitting for the Part II examination. 30 Using the PearlDiver database, Taylor et al 35 found that age older than 40 years was a risk factor for revision surgery, along with female sex, obesity, smoking, and a concomitant diagnosis of biceps tendinitis at or before the time of surgery.
The trends of the present study provide a valuable update to previous reports by incorporating the proportion of patients who undergo each procedure. The inadequacy of SLAP repair for patients above the age of 40 years is reflected by the large increase in BT performed in this age group. Authors have suggested lowering the age threshold for the performance of BT because of inferior outcomes in SLAP repair beyond the age of 36 years. 32 Postoperative stiffness is also a concern after these surgical procedures. The proportions of this complication did not significantly differ based on surgery and ranged between 3.6% and 6.0%. However, the demographics of patients undergoing each procedure are different, which may have confounded the rates of postoperative stiffness. For example, patients undergoing debridement may have the highest rate of stiffness because they were also the oldest.
Limitations of this study relate primarily to the limitations of using a national private-payer insurance database. Although the use of the Humana database allowed us to determine broad trends in the treatment of isolated SLAP tears in the United States over the study period, the database also comes with multiple limitations. This includes potential limitations in the quality of data and accuracy of diagnosis and procedure coding. Biceps tenotomy, for example, is not routinely coded after procedures; rather, it is often grouped within debridement codes. Therefore, it is potentially confounding whether patients are truly undergoing tenotomy versus debridement. The data are limited to the United States and may not extrapolate to trends elsewhere in the world. The Humana database also has an increased concentration of patients specifically in the northeastern United States compared with other regions. Furthermore, the database consists of patients from a single private payer insurance company and may not extrapolate to other privately or publicly insured patients in the United States.
Additionally, we could determine intraoperative findings regarding the type and nature of the SLAP tear as well as associated defects to the biceps tendon or elsewhere in the shoulder. We did attempt as best as possible to achieve a series of patients with a SLAP tear diagnosis who underwent isolated surgical treatment by limiting our search to patients with a diagnosis code for a SLAP tear and excluding a range of concomitant shoulder surgical CPT codes that are not isolated SLAP tear treatment options. Also because of the database limitations, we were unable to determine an array of patient preoperative factors that influence surgical treatment decisions, such as nonoperative treatment, duration of symptoms, nature of patient symptoms, physical examination and radiographic findings, workers’ compensation status, and sports participation such as overhead athletes. We were similarly limited postoperatively, as the database lacked postoperative radiographic or physical examination findings, lacked patient-reported outcomes, and did not indicate if patients returned to their recreational and occupational demands.
Conclusion
An analysis of a large private-payer database revealed that the surgical treatment of isolated SLAP tears in the United States shifted from 2007 to 2016, with an increase in the frequency of BT and a decline in the frequency of SLAP repair, particularly in patients older than 40 years.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: G.L.C. has received research and educational support from Arthrex, Medwest Associates, and Smith & Nephew and has received hospitality payments from DJO and Zimmer Biomet. B.F. has received research support from Stryker and hospitality payments from Medwest Associates. A.A.R. has received research support from Arthrex, DJO Surgical, Smith & Nephew, and Ossur; is a paid consultant and paid speaker for Arthrex; and receives royalties from Arthrex and Saunders/Mosby-Elsevier. N.N.V. has received consulting fees from Medacta and Smith & Nephew, speaking fees from Pacira Pharmaceuticals, educational support from Medwest Associates, receives royalties from Smith & Nephew, has stock or stock options in CyMedica Orthopedics, and has received hospitality payments from Arthrex, Stryker, and Wright Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by the Rush University Medical Center Institutional Review Board.