
Abstract
Background:
Humeral head reconstruction with fresh osteochondral allografts (OCA) serves as a potential treatment option for anatomic reconstruction. More specifically, talus OCA is a promising graft source because of its high congruency with a dense cartilaginous surface.
Purpose:
To analyze the surface geometry of the talus OCA plug augmentation for the management of shoulder instability with varying sizes of Hill-Sachs lesions (HSLs).
Study Design:
Controlled laboratory study.
Methods:
Seven fresh-frozen cadaveric shoulders were tested in this study. The humeral heads were analyzed using actual patients’ computed tomography scans. Surface laser scan analysis was performed on 7 testing states: (1) native state; (2) small HSL; (3) talus OCA augmentation for small HSL; (4) medium HSL; (5) talus OCA augmentation for medium HSL; (6) large HSL; and (7) talus OCA augmentation for large HSL. OCA plugs were harvested from the talus allograft and placed in the most medial and superior aspect of each HSL lesion. Surface congruency was calculated as the mean absolute error and the root mean squared error in the distance. A 1-way repeated-measures analysis of variance was performed to evaluate the effects of the difference in the HSL size and associated talus OCA plugs on surface congruency and the HSL surface area.
Results:
The surface area analysis of the humeral head with the large (1469 ± 75 mm2), medium (1391 ± 81 mm2), and small (1230 ± 54 mm2) HSLs exhibited significantly higher surface areas than the native state (1007 ± 88 mm2; P < .001 for all sizes). The native state exhibited significantly lower surface areas as compared with after talus OCA augmentation for large HSLs (1235 ± 63 mm2; P < .001) but not for small or medium HSLs. Talus OCA augmentation yielded improved surface areas and congruency after treatment in small, medium, and large HSLs (P < .001).
Conclusion:
Talus OCA plug augmentation restored surface area and congruency across all tested HSLs, and the surface area was best improved with the most common HSLs—small and medium.
Clinical Relevance:
Talus OCA plugs may provide a viable option for restoring congruity of the shoulder in patients with recurrent anterior glenohumeral instability and an HSL.
Keywords
Recurrent anterior glenohumeral instability remains a growing concern, largely because of its complex pathology of osseous defects. Hill-Sachs lesions (HSLs) are posterior superolateral humeral head compression fractures that tend to be associated with anterior shoulder instability or dislocation. Although previous reports suggest that 40% to 90% of patients who present with anterior shoulder instability have HSL, its incidence is not known with certainty. For patients with recurrent anterior shoulder instability events, it may be nearly 100%.17,25 HSLs pose a significant risk for recurrent anterior glenohumeral instability that is not readily responsive to surgical treatment. 18 Therefore, addressing and treating HSLs quickly and appropriately when indicated is of high importance.
The idea of an engaging HSL being a strong indication for surgical management was first introduced by Yamamoto et al 26 in 2007. A lesion is considered engaging, or “off-track,” when it is located outside of the glenoid track, which is the contact zone between the glenoid and humeral head. 5 This results in the HSL on the humeral head interacting with the glenoid rim, resulting in the further formation of bony defects on both the glenoid and the humeral head. Recently, Di Giacomo et al 6 proposed the Glenoid Track Instability Management Score, a new scoring treatment algorithm that incorporates the glenoid track concept into the Instability Severity Index Score to predict failure after surgery for shoulder instability. The treatment goal for an HSL is to prevent engagement of the lesion directly or indirectly along the glenoid track (off-track HSL). 17 Notable treatments for engaging HSLs include humeral head reconstruction, tissue filling (remplissage procedure), disimpaction, and prosthesis replacement. 17 When considering the various surgical procedures, certain parameters ultimately make up the decision-making process to determine which procedure to use. Some of these parameters include the size of the HSL, concomitant glenoid bone loss, chronicity, age, and demand of the patients.17,19 Disimpaction may be advocated for acute lesions (<3 weeks) and moderate-sized HSL (<40% of the articular surface). 17 The surgical options, including resurfacing and replacement, are generally preserved for older patients, those who are less active, or patients with severe arthritis. 17 The remplissage procedure achieves excellent results, with limitations relating to the nature of a nonanatomic repair construct. This includes the loss of external rotation (ER), thus severely limiting athletes in various throwing sports.9,16
Humeral head reconstruction is indicated for a large HSL without significant glenoid bone loss. 17 Fresh osteochondral allografts (OCAs) are preferred because they allow for anatomic reconstruction of the humeral head while addressing any associated chondral deficiencies and have a lower resorption rate. 22 A systemic review from Saltzman et al 22 showed significant improvements in clinical outcomes and shoulder motion at 1 year postoperatively after humeral reconstruction using allografts. Their results also demonstrated high graft-related complications, such as graft necrosis (8.7%), resorption (36.2%), and glenohumeral arthritic change (35.7%), after a final follow-up of patients who underwent humeral reconstruction using a frozen allograft. However, there was no report of these complications after receiving a fresh allograft. 22 The use of fresh humeral head allografts has shown success in repairing HSLs. However, concerns over the availability of donors and the risk of graft harvest contamination from the donor have warranted a search for alternative allograft sites. 14
For several reasons, the fresh talus allograft has been indicated as a promising source of OCA for the humeral head.3,11 The superior articular surface of the talus has a similar radius of curvature (receiver operating characteristic [ROC]) to the humeral head; thus, the curvature is not affected by the graft size and laterality of the talar dome graft. 3 In addition, the cartilaginous surface of the talus creates a more profound articular contact with the glenoid, allowing for a more stable graft fixation. 20 Furthermore, anthropometric measurements of the talus are almost identical to the humeral head and the ROC of the glenoid. 11 These numerous features of a talus OCA incentivize further investigation into its use for humeral head reconstruction.
In this study, we aimed to evaluate the surface geometry of talus OCA plug augmentation for the management of anterior shoulder instability with varying sizes of HSLs in the hope of arthroscopic adaptation of this technique. We hypothesized that talus OCA augmentation with single or multiple OCA talus plugs would be able to restore the shoulder’s bone curvature and surface area relative to the native state.
Methods
Specimen Preparation
The use of cadaveric specimens does not require institutional review board approval at our institution. Seven fresh-frozen cadaveric shoulders (6 men and 1 woman; mean age, 51 years [range, 41-65 years]) were used in this study. The specimens were donated to a tissue bank for medical research and then purchased by our institution. Specimens were excluded if there was any history of injury, surgery, osteoporosis, osteoarthritis, or age >65 years. The shoulders were thawed at room temperature overnight before testing. All skin, subcutaneous tissue, and muscles were dissected down to the glenohumeral joint, leaving only the humeral head. The humeral diaphysis was cut 15 cm from the shoulder joint line after the joint coordinate frame was created using the Romer Arm (SimVITRO). The humerus was rigidly secured to the fixture, and a laser scanner attachment for the Romer Arm was used to record a 3-dimensional (3D) digitized point cloud of the humeral head in the same Romer Absolute Arm coordinate frame.
Study Design
This study had a repeated-measures experimental design to adequately compare the surface geometry of the native humeral head, the HSL, and the humeral head after performing talus OCA augmentation states for all 3 sizes of HSLs on all 7 specimens. Surface analysis was performed on 7 testing states in the following order:
Native state
Small HSL
Talus OCA augmentation of small HSL
Medium HSL
Talus OCA augmentation of medium HSL
Large HSL
Talus OCA augmentation of large HSL
Surgical Technique
A 3D plastic model was created using the actual computed tomography (CT) scans from patients, with the varying size of HSLs as small (mean width, 12.3 mm; mean length, 23.4 mm; mean depth, 3.5 mm; volume, 323.5 mm3); medium (mean width, 17.1 mm; mean length, 23.2 mm; mean depth, 3.1 mm; volume, 501.5 mm3); and large (mean width, 22.4 mm; mean length, 25.2 mm; mean depth, 3.1; volume, 607.2 mm3). The actual CT scan data that were used were from Golijanin et al. 10 We only needed the dimensions of the HSLs to create the small, medium, and large HSLs. The 3 plastic resin HSLs (small, medium, and large) were created using a 3D printer (Ultimaker3; Ultimaker) and converted to the cadaveric model. The exact HSLs were transcribed to each cadaveric shoulder with scaling based on the percentage difference in humeral head articular diameter between the model and each of the shoulder specimens. The humeral head defect and the volume were determined; then, a nearly size-matched humeral head from a cadaveric shoulder was used.
The HSL was created according to measurements from the center of the humeral head and the junction of the articular margin and the neck of the humerus. The plastic mold helped to precisely reproduce the corresponding size, location, and volume in the cadaveric shoulders. Starting with the small HSL defect, the defect was created using a combination of an oscillating saw, burr, and rasp to achieve the precise defect size and shape based on the plastic positive mold of the defect (Figure 1). Next, talus OCA augmentation was performed by harvesting the frozen full talus allograft (JRF Ortho) using the osteochondral allograft transplantation system (OATS 2.0 System; Arthrex), with sizes varying from 8-, 10-, and 12-mm diameter. A single board-certified orthopaedic surgeon (P.G.) chose 1 to 3 talus OCA bone plugs (optimal size) to fill the HSL bone defect in each specimen by placing the bone plugs in the most medial and superior aspect of the small HSL defect. The same process was performed in each specimen for the medium and large HSL defects (Figures 2 and 3).

The right humerus from a cadaveric specimen and a 3-dimensional plastic mold model created from a CT scan of an actual patient. The HSL defect (small size) was created at the site marked on the cadaveric shoulder (arrow) using a combination of an oscillating saw, bur, and rasp to achieve the precise defect size and shape based on the plastic positive mold of the defect. CT, computed tomography; HSL, Hill-Sachs lesion.

The right humerus cadaveric shoulder demonstrated that (A) the medium HSL defect was created using a 3-dimensional plastic mold. (B) The anteroposterior view and (C) the lateral view of the humerus after using talus OCA bone plugs (arrowheads) to fill the HSL bone defect. HSL, Hill-Sachs lesion; OCA, osteochondral allograft.

The right humerus cadaveric shoulder demonstrated that (A) the large HSL defect was created using a 3-dimensional plastic mold. (B) The anteroposterior view and (C) the lateral view of the humerus after using talus OCA bone plugs (arrowheads) to fill the HSL bone defect. HSL, Hill-Sachs lesion; OCA, osteochondral allograft.
Surface Analysis
The border of the posterosuperior region of the humeral head was defined by creating a fiducial marker at each corner of the border. The humerus was explanted from the specimen and rigidly secured to a fixture adjacent to the laser scanner. The 4 fiducials for each test state were digitized with the pointed tip of a coordinate measuring machine (Romer Absolute Arm; Hexagon Manufacturing Intelligence) to define the global location of the humeral head relative to the coordinate frame of the Romer Absolute Arm. For nonnative testing states, the Romer Absolute Arm was used to define the global location of the HSL. With the humerus still rigidly secured to the fixture, a laser scanner attachment for the Romer Arm (HP-L-8.9; manufacturer-reported accuracy 0.04 mm; Hexagon Manufacturing Intelligence) was used to record a 3D digitized point cloud of the humeral head in the same Romer Absolute Arm coordinate frame. This process was repeated for each testing state.
The laser scan data were processed using a custom MATLAB (Version R2021a; The MathWorks) script. All point clouds were trimmed to the marked boundaries of the humeral head. For each specimen and testing state, the surface area was computed from the point cloud. To determine the surface congruency of the HSL state and the OCA state relative to the native state, the point cloud of each nonnative testing state was registered to the point cloud of the native state using an iterative closest point algorithm. Surface congruency was calculated as the root mean squared deviation in normal distance between registered points from the nonnative specimen to the native specimen. For the OCA testing state, only points on the contact surface of the OCA were included in the congruency calculation (Figure 4).
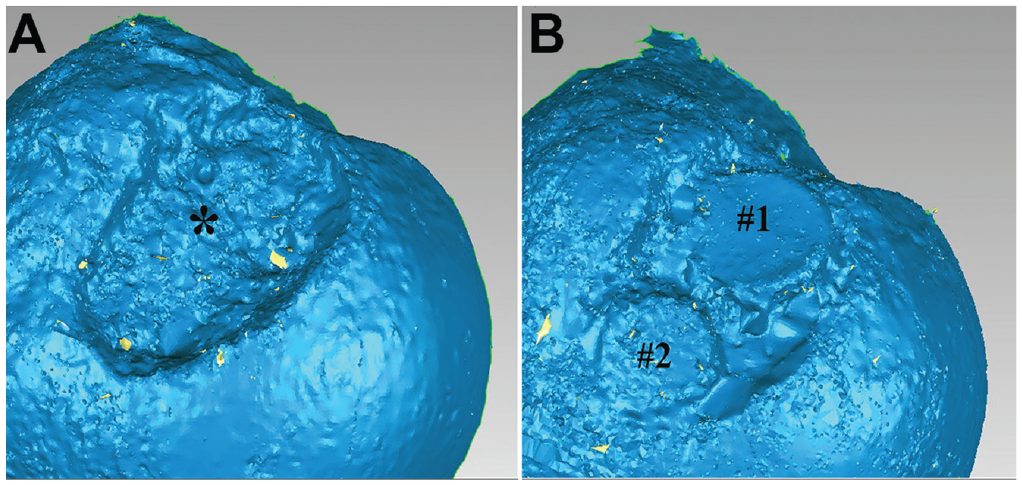
Surface analysis of the laser scan data after processing demonstrated (A) an HSL defect (asterisk) and (B) an improvement in surface area and congruence after the talus OCA augmentation with bone plug (#1 and #2). HSL, Hill-Sachs lesion; OCA, osteochondral allograft.
Statistical Analysis
A 1-way repeated-measures analysis of variance followed by a post hoc test was performed to evaluate the effects of the HSL size differences and associated talus osteochondral augmentations on surface congruency, HSL surface area, and HSL volume. The required sample size was calculated under experimental conditions of small effect size (0.3), a mean correlation of 0.85, and an alpha of .05. A minimum of 7 specimens was needed to show a significant difference in the mean congruency match with a power of 80%. Statistical analysis was performed and graphs were created using the statistical software SPSS for Windows Version 18.0 (SPSS Inc). P values < .05 were considered to be statistically significant.
Results
The surface area analysis of the humeral head with the large (1469 ± 75 mm2), medium (1391 ± 81 mm2), and small (1230 ± 54 mm2) HSLs exhibited significantly higher surface areas than the native state (1007 ± 88 mm2; P < .001 for all sizes). The native state exhibited significantly lower surface areas as compared with after talus OCA augmentation for large HSLs (1235 ± 63 mm2; P = 1.39E-05). However, there was no significant difference in the surface area between the native state and after talus augmentation for small (1044 ± 82 mm2) and medium HSLs (1104 ± 73 mm2) (P = 6.61E-05 and P = 1.83E-07, respectively) (Table 1 and Figure 5).
Surface Area Results From the Surface Analysis of HSL Defect States and After Performing Talus OCA Plug Augmentation a .
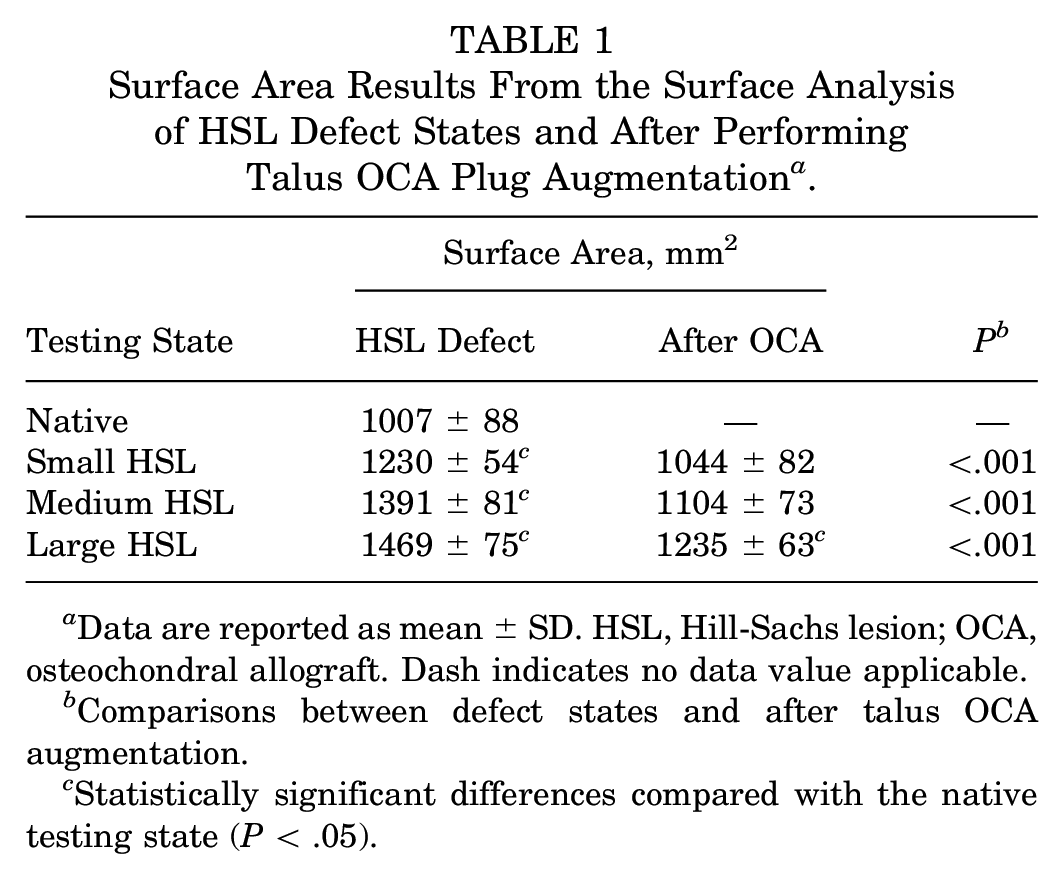
Data are reported as mean ± SD. HSL, Hill-Sachs lesion; OCA, osteochondral allograft. Dash indicates no data value applicable.
Comparisons between defect states and after talus OCA augmentation.
Statistically significant differences compared with the native testing state (P < .05).

The surface analysis (surface area, mm2) of the different stages of the study: native state; small, medium, and large HSL defect state; and after talus OCA augmentation of small, medium, and large HSLs. P values indicate comparisons between defect states and after talus OCA augmentation (all significantly different; P < .05). *Statistically significant differences compared with the native state. HSL, Hill-Sachs lesion; OCA, osteochondral allograft.
Talus OCA augmentation yielded improved congruency across small (from 3.73 ± 0.41 mm to 1.60 ± 0.42 mm), medium (from 4.02 ± 0.41 mm to 1.82 ± 0.31 mm), and large (from 4.57 ± 0.45 mm to 1.95 ± 0.23 mm) HSLs (P < .001 for all sizes) (Table 2 and Figure 6).
Congruency Results From the Surface Analysis of the HSL Defect States and After Performing Talus OCA Plug Augmentation a

Data are reported as mean ± SD. HSL, Hill-Sachs lesion; OCA, osteochondral allograft.
Comparisons between defect states and after talus OCA augmentation.
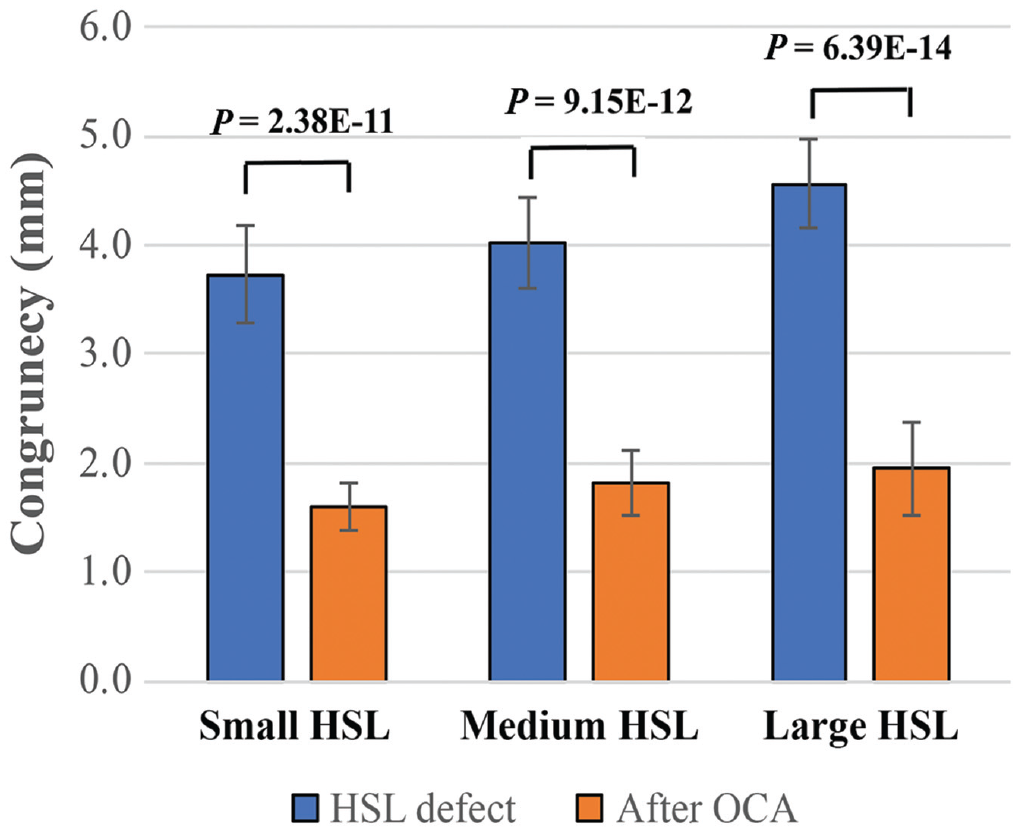
The surface analysis (congruency, mm) of the different stages of the study: small, medium, and large HSL defect state and after talus OCA augmentation of small, medium, and large HSLs. P values indicate comparisons between defect states and after talus OCA augmentation (all significantly different; P < .05). HSL, Hill-Sachs lesion; OCA, osteochondral allograft.
Discussion
The principal finding of this study is that using talus OCA bone plugs to fill small, medium, and large HSLs restored the humeral head surface area and congruency across all tested models. Interestingly, talus OCA saw the best improvement in restoring the surface area for the most common HSLs: small (1230 ± 54 mm2 to 1044 ± 82 mm2; P < .001) and medium (1391 ± 81 mm2 to 1104 ± 73 mm2; P < .001) sizes. Talus OCA provided limited benefit in restoring the surface area for large HSLs (1469 ± 75 mm2 to 1235 ± 63 mm2; P < .001). However, the results of this study confirm that the use of talus OCA in the treatment of varying HSL sizes can re-create the humeral head congruency to a near-normal state (small: 3.73 ± 0.41 mm to 1.60 ± 0.42 mm; P < .001; medium: 4.02 ± 0.41 mm to 1.82 ± 0.31 mm; P < .001; large: 4.57 ± 0.45 mm to 1.95 ± 0.23 mm; P < .001). Therefore, in this cadaveric model, talus OCA provides a viable option in returning congruency of the humeral head for the humeral reconstruction of the shoulder in shoulder models with recurrent anterior glenohumeral instability and HSLs.
HSLs have become increasingly recognized in the literature as a risk factor for recurrent instability after both arthroscopic and open shoulder stabilization procedures. Off-track and engaging HSLs are risk factors for recurrent shoulder instability and worse outcomes.4,23,26 In a study by Cetik et al, 2 the extent of the HSLs in 30 patients with recurrent shoulder instability was assessed. It was found that there was a correlation between the number of recurrent dislocations, as well as the extent and depth of the HSL. Another study by Horst et al 12 found that larger HSLs decrease the available contact surface with the glenoid and can lead to a greater risk of recurrent dislocations. Recently, the location of the medial margin of HSL relative to the anterior glenoid rim, medialization, or the peripheral-track lesion is considered one of the significant risk factors for recurrent instability and worse outcomes.13,27 In this study, the authors filled the talus OCA plug in the most medial and superior aspect of the HSL defects. The authors believe that talus OCA plug optimization will be beneficial for humeral reconstruction in the treatment of varying sizes of HSLs by preventing the medialization of the HSLs. In addition, more attention is needed to address HSLs in the treatment algorithm of anterior shoulder instability.
Several different methods have been described to address HSLs. The described methods to address an off-track HSL are remplissage, humeral head reduction, partial humeral head arthroplasty, humeral head hemiarthroplasty, and finally humeral head reconstruction using autografts or allografts. All of these procedures have their pros and cons. Initially described by Purchase et al, 21 the remplissage procedure involves arthroscopically tenodesing the infraspinatus and posterior capsule into the Hill-Sachs defect. A retrospective cohort study review by Pandey et al 15 showed that patients with off-track HSLs who underwent a remplissage procedure in addition to an arthroscopic Bankart repair demonstrated significantly fewer dislocations than patients who did not undergo a remplissage procedure. Additionally, they showed that patients who underwent a remplissage had significantly reduced ER compared with those who did not have a remplissage procedure. Therefore, it is generally regarded that although adding a remplissage procedure can help reduce instability rates, it causes a reduction in ER motion. This loss of ER can be a significant problem for athletes returning to overhead sports, especially baseball. Garcia et al 8 developed a novel method to treat HSL in which the cortical surface of the humerus was tamped up to restore articular congruity; the void was then back-filled with Quickset (Arthrex) injectable calcium phosphate bone cement. The downside of this method is that it can only be used in acute situations, and most attritional bone loss is in the subacute or chronic setting. Additionally, this method lacks long-term follow-ups for the durability of this procedure. Another technique to address large HSLs includes partial or complete humeral head resurfacing arthroplasty. Arthroplasty can be a good technique to treat large HSLs. However, it may not be ideal for young patients or patients who wish to return to contact sports, such as American football, rugby, or wrestling.
Another technique used to treat large HSLs has been the use of bone augmentation or humeral reconstruction using an allograft to fill the lesion with an open approach. 7 In a study by Zhuo et al, 28 a total of 19 patients who had large HSLs were treated using open femoral head allografts to fill the lesion, which resulted in significant improvements in the patients’ American Shoulder and Elbow Surgeons scores and Constant-Murley and Rowe scores at a mean of 27.8 months of follow-up, with an overall satisfaction rate of 94.7%. However, graft resorption was seen radiographically at 1 year in 9 patients (47.4%). Snir et al 24 used a sized matched osteochondral humeral head allograft to reconstruct an HSL by arthroscopic surgery. Size and congruence matching of the humeral head defects play a critical role in stabilizing the shoulder. In a biomechanical study by Bakshi et al, 1 a 25% HSL model and a perfectly matched OCA provided more glenohumeral joint stability and less translation motion than an imperfect OCA repair. Their overall message was that the graft repair must closely match the HSLs and restore the humeral head anatomy. The talus is an ideal graft for humeral head defects as the superior articular surface of the talus has a similar radius of curvature to the humeral head. Our study demonstrated that a talus OCA could be used to restore the congruity of the humeral head and improve the surface area with the most common HSLs—small and medium. Talus OCA saw the best surface area improvement in treating small and medium HSLs, most likely because the larger lesions required more plugs, which may have led to a larger defect area between the plugs. Multiple OCA plugs were used instead of a large graft cut to size because of the eventual goal of arthroscopic implementation of this technique to avoid the morbidity of a subscapularis take-down, subscapularis split, or open posterior approach. Biomechanically, our study showed that the use of the talus OCA could be a viable option to treat HSLs. However, clinical studies are needed to validate the healing rates, overall patient outcomes, risk of recurrent instability, and viability of this graft fixation.
There are several limitations to this study. First, all 3D humeral and HSL plastic models in this study were generated from the CT scans of actual patients who were all men. Therefore, the findings of this study cannot be fully generalized to the general population. Second, all HSL defects were created using a combination of an oscillating saw, bur, and rasp, which depended on the operator. One board-certified orthopaedic surgeon created all the HSL defects to mitigate the error and performed talus OCA augmentation. In addition, scaling the exact HSLs by the difference in humeral head diameter and utilizing a plastic mold helped to meticulously create the corresponding sizes, locations, and volumes of the HSLs in the cadaveric shoulders. Finally, this study presented the degree of restoring the surface area and congruency in time zero. Additional in vivo studies may be beneficial to understand the effect of talus OCA, such as graft healing, resorption, clinical outcomes, and risk of recurrent instability after this procedure.
Conclusion
Talus OCA plug augmentation restored surface area and congruency across all tested HSLs in this cadaveric model, and the surface area was best improved with the most common HSLs—small and medium. Talus OCA plug provides a viable option for restoring congruity of the shoulder in patients with recurrent anterior glenohumeral instability and an HSL. Additional work is necessary to assess the overall mechanics and healing in vivo.
Footnotes
Acknowledgements
The authors express their special appreciation to the Steadman Philippon Research Institute Digital Media team for the illustrations.
Final revision submitted May 1, 2023; accepted May 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: M.T.P. has received research support from DJO; consulting fees from Arthrex, Arthrosurface, JRF Ortho, and Zimmer Biomet; royalties from Anika Therapeutics, Arthrex, Arthrosurface, and Responsive Arthroscopy; and honoraria from Flexion Therapeutics. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.