
Abstract
Background:
Posterior instability has been reported to account for up to 24% of cases of shoulder instability in certain active populations. However, there is a paucity of data available regarding the risk factors associated with posterior glenoid bone loss.
Purpose:
To characterize the epidemiology of, and risk factors associated with, glenoid bone loss within a cohort of patients who underwent primary arthroscopic shoulder stabilization for isolated posterior-type glenohumeral instability.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
This was a retrospective analysis of patients who underwent primary arthroscopic shoulder stabilization for posterior-type instability between January 2011 and December 2019. Preoperative magnetic resonance arthrograms were used to calculate posterior glenoid bone loss using a perfect circle technique. Patient characteristics and revision rates were obtained. Bone loss (both in millimeters and as a percentage) was compared between patients based on sex, age, arm dominance, sports participation, time to surgery, glenoid version, history of trauma, and number of anchors used for labral repair.
Results:
Included were 112 patients with a mean age of 28.66 ± 10.07 years; 91 patients (81.25%) were found to have measurable bone loss. The mean bone loss was 2.46 ± 1.68 mm (8.98% ± 6.12%). Significantly greater bone loss was found in athletes versus nonathletes (10.09% ± 6.86 vs 7.44% ± 4.56; P = .0232), female versus male patients (11.17% ± 6.53 vs 8.17% ± 5.80; P = .0212), and patients dominant arm involvement versus nondominant arm involvement (10.26% ± 5.63 vs 7.07% ± 6.38; P = .0064). Multivariate regression analysis identified dominant arm involvement as an independent risk factor for bone loss (P = .0033), and dominant arm involvement (P = .0024) and athlete status (P = .0133) as risk factors for bone loss >13.5%. At the conclusion of the study period, 7 patients had experienced recurrent instability (6.25%).
Conclusion:
The findings of this study are in alignment with existing data suggesting that posterior glenoid bone loss is highly prevalent in patients undergoing primary arthroscopic stabilization for posterior-type shoulder instability. Our results suggest that patients with dominant arm involvement are at risk for greater posterior glenoid bone loss. Athlete status and dominant arm involvement were identified as independent risk factors for bone loss >13.5%.
Posterior glenohumeral instability is an increasingly recognized cause of shoulder pain and dysfunction, particularly among young, athletic patients.5,18,20,21,23,25,29 While historically thought to comprise only 2% to 10% of cases of shoulder instability, 21 posterior instability may account for up to 24% of cases in certain active populations based on recent studies.25,27 Despite increasing understanding and diagnosis of posterior instability, relatively limited data exist on risk factors associated with failure after operative stabilization.
Glenoid bone loss in the setting of anterior glenohumeral instability has been well described; however, fewer studies have characterized bone loss in patients with isolated posterior instability. Recent studies by Hines et al 16 and Wolfe et al 28 noted posterior bone loss in 69% and 86%, respectively, of patients with primary, isolated posterior instability. While the importance of bone loss with respect to the management of posterior glenohumeral instability is not fully understood, it is a known risk factor for failure after arthroscopic anterior stabilization procedures. 10 Anterior bone loss of >13.5% has been shown to negatively affect functional outcomes after arthroscopic labral repair, and patients with significant bone loss of >20% are often indicated for open bony augmentation.13,24 Additionally, male sex, participation in contact sports, age, and recurrent dislocations have been shown to correlate with greater bone loss in anterior instability. 19 With regard to posterior instability, biomechanical studies have shown that posterior bone loss is correlated with greater posterior humeral translation in cadaveric models. 9 Furthermore, Arner et al 2 found that ≥11% bone loss implicated a 10 times higher surgical failure rate, and ≥15% bone loss was associated with a 25 times higher likelihood of failing after arthroscopic posterior labral repair. However, there is a current paucity of data reporting on variables associated with greater posterior bone loss. Given the high reported prevalence of glenoid bone loss among patients with posterior instability, it is important that surgeons better understand this pathology and its associated risk factors.
The purpose of this study was to characterize the epidemiology of, as well as the risk factors associated with, glenoid bone loss within a cohort of patients who underwent primary arthroscopic shoulder stabilization for isolated posterior-type glenohumeral instability. We hypothesized that glenoid bone loss would be highly prevalent in this population and that male sex and athletic participation would be associated with greater bone loss.
Methods
This was a retrospective analysis of prospectively collected data from patients who underwent primary surgical shoulder stabilization for posterior-type instability between January 2011 and December 2019 with 1 of the 2 fellowship-trained shoulder and elbow surgeons (R.C.T. and N.P.). Institutional review board approval was obtained for the study protocol.
The surgical database was queried for all arthroscopic shoulder instability procedures performed over a 9-year period (2011-2019). Operative reports were then reviewed to identify patients with isolated posterior shoulder instability. Included were all patients aged ≤50 years who underwent a primary arthroscopic surgical procedure for posterior-type instability with a minimum 2-year follow-up and who had a preoperative magnetic resonance arthrogram (MRA) with gadolinium, from which glenoid bone loss and glenoid version could be obtained. Patients with a history of previous shoulder surgery, full-thickness rotator cuff tears, glenoid osteochondral defects, or instability secondary to generalized hyperlaxity were excluded from the study. Patients who underwent bony augmentation procedures were not eligible for inclusion. All patients had symptoms recalcitrant to nonoperative management including, but not limited to, nonsteroidal anti-inflammatory drugs, physical therapy, and home exercise programs.
Patient characteristics, preoperative chief complaint, mechanism of injury, and duration of symptoms were collected routinely during clinic visits. Traumatic etiology was defined as symptom onset after a specifically recalled acute event. Athletes were defined as patients who reported weekly participation in organized sporting activities. All patients underwent 1.5-T MRA as part of their preoperative evaluation. Operative reports and imaging were reviewed to determine labral tear location, the number of anchors used for labral repair, concomitant pathologies, and concomitant procedures. Surgical failure rates were collected as part of the postoperative follow-up. Surgical failure was defined as recurrent symptomatic posterior glenohumeral instability.
Glenoid bone loss was determined from preoperative MRAs using an adapted method of the perfect circle technique as described by Hines et al 16 (Figure 1). Maximal posterior glenoid bone loss and glenoid version were recorded. All MRAs were evaluated independently by 2 attending orthopaedic surgeons (R.C.T. and N.P.). For cases in which there was a discrepancy between measurements, the MRA was reviewed by a third attending surgeon.

MRA image of a right shoulder in a 27-year-old male patient demonstrating a posterior glenoid defect of 8.52% (2.46 mm) as measured using the perfect circle technique. MRA, magnetic resonance arthrogram.
Statistical Analysis
Statistical analyses were performed using SPSS software (Version 20; IBM). Student t tests were utilized to compare continuous data series with a normal distribution of variance. Chi-square tests were used to compare categorical variables. Univariate Pearson correlation coefficients were calculated to assess the possible association between the glenoid version, time to surgery, number of anchors used, and age at the time of injury and glenoid bone loss. Interrater reliability was determined by calculating intraclass correlation coefficients (ICCs) based on the mean of 3 measurements for each of the 2 investigators. Intrarater reliability was also determined from separate sets of measurements from each investigator performed 2 weeks apart. Multivariate regression analysis was performed using variables that showed statistical significance in univariate analysis. A linear model was utilized for continuous dependent variables, and a logistical model was utilized for categorical dependent variables. Statistical significance was set at P < .05 for all comparisons.
Results
A total of 146 patients underwent arthroscopic shoulder stabilization procedures for posterior-type shoulder instability during the study period. Eleven patients had concomitant glenoid osteochondral defects, 14 had full-thickness rotator cuff tears, and 9 were subsequently lost to follow-up, leaving 112 patients available for the final analysis (Figure 2). The mean age at the time of surgery was 28.66 years (14-50 years), and 71.21% of patients were men. The mean length of follow-up was 46.47 months (24-117 months), and the mean time to surgery from symptom onset was 19.79 months (1-192 months) (Table 1).

Flowchart showing patient selection.
Overall Patient Characteristics (N = 112) a
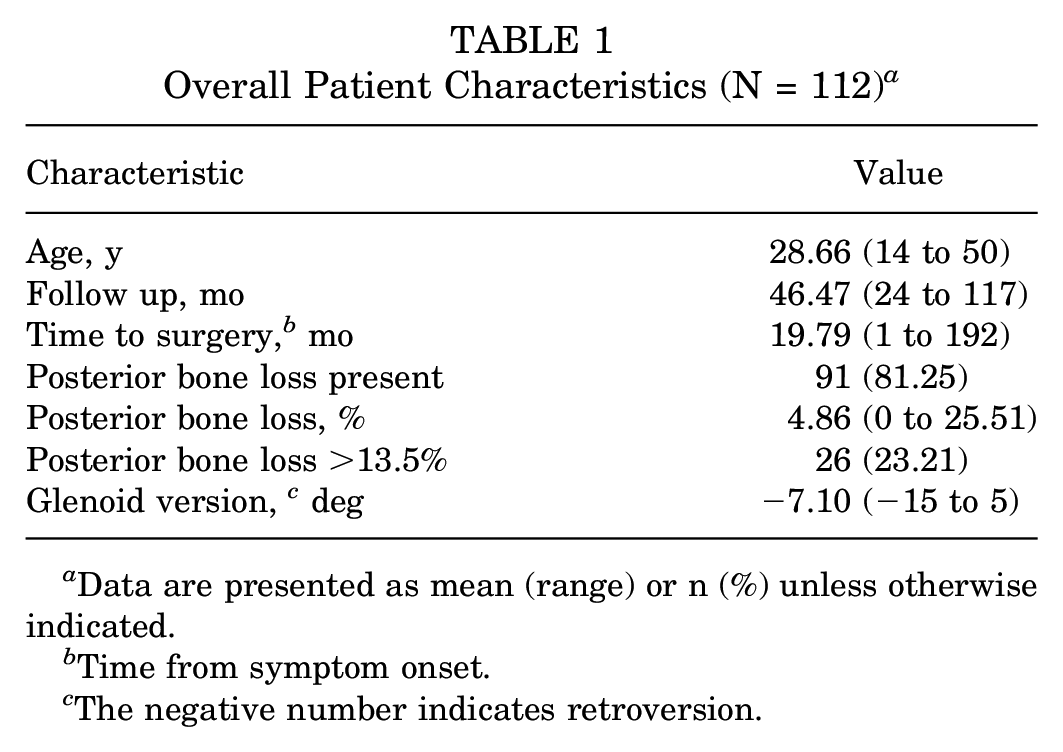
Data are presented as mean (range) or n (%) unless otherwise indicated.
Time from symptom onset.
The negative number indicates retroversion.
Measurable bone loss was noted in 91 (81.25%) patients. All bone loss was located posteroinferiorly. The mean bone loss was 8.98% (2.46 mm), and bone loss followed a normal distribution (K2 value, 1.576). A total of 26 (23.21%) patients had subcritical bone loss of >13.5%, and 5 patients had bone loss of >20%. Intra- and interrater ICCs for glenoid bone loss measurements were 0.94 and 0.87, respectively. With regard to risk factors, univariate analysis revealed a significantly greater bone loss in female patients (11.17% ± 6.53% vs 8.17 ± 5.80%; P = .0212), athletes (10.09 ± 6.86% vs 7.44 ± 4.56%; P = .0232), and patients with dominant arm involvement (10.26 ± 5.63% vs 7.07 ± 6.38%; P = .0064) (Table 2). Of these variables, multivariate linear regression identified dominant arm involvement (P = .0033) as an independent risk factor for greater bone loss (Table 3). No significant differences in bone loss were noted when comparing the traumatic cause or the number of anchors required for labral repair. No significant correlation was found between glenoid bone loss and glenoid version (r = −0.0090; P = .9249), time to surgery from symptom onset (r = −0.1361; P = .1525), age at the time of surgery (r = −0.0823; P = .3882), or the number of anchors used (r = −0.1675; P = .0775). Significantly more women, athletes, and patients with dominant arm involvement had a bone loss of >13.5% when compared with men (36.66% vs 19.51%; P = .0414), nonathletes (32.31% vs 10.64%; P = .0074), or those whose nondominant shoulder was involved (31.34% vs 11.11%; P = .0129). Of these, multiple logistic regression identified athlete status and dominant arm involvement as risk factors for bone loss >13.5% (Table 3). At the conclusion of the study period, 7 patients (6.25%) had reported recurrent symptoms of posterior instability.
Comparison of Glenoid Bone Loss by Variable a

Data are presented as mean ± SD or n (%) unless otherwise indicated. Bold P values indicate statistical significance (P < .05).
Results of Regression Analysis for Glenoid Bone Loss and Bone Loss >13.5% a
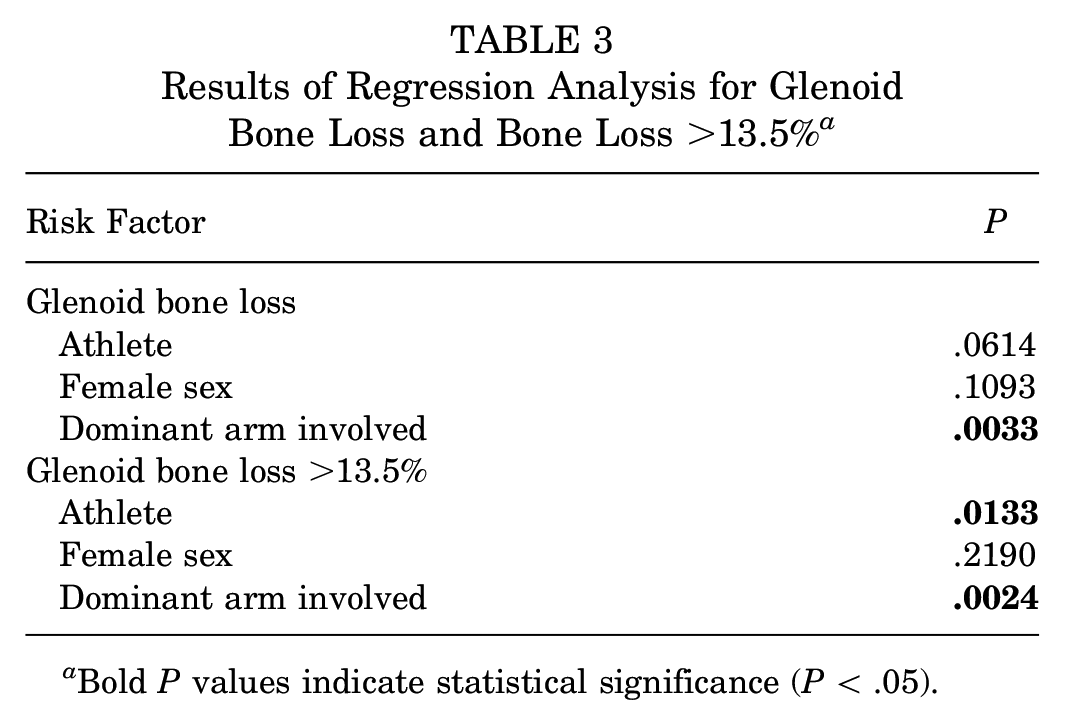
Bold P values indicate statistical significance (P < .05).
Discussion
Our findings indicated that posterior bone loss was highly prevalent in patients undergoing stabilization for posterior instability, with 81.25% of patients having measurable bone loss and 23.21% of patients having bone loss >13.5%. We identified dominant arm involvement as an independent risk factor for greater glenoid bone loss. Furthermore, athlete status and dominant arm involvement were found to be risk factors for bone loss >13.5%. In contrast to our hypothesis, male sex was not an independent risk factor for glenoid bone loss or bone loss >13.5%. To our knowledge, this is the first study to analyze risk factors associated with greater bone loss in patients undergoing primary posterior labral repair. Furthermore, this analysis represents the largest study to date reporting on bone loss in the setting of isolated posterior glenohumeral instability.
While posterior instability has become an increasingly recognized cause of shoulder pain and dysfunction, particularly in active populations, there is a relative paucity of data available regarding associated posterior glenoid bone loss.5,8,17,18,20,21,25,27 A 2018 study by Hines et al 16 noted measurable bone loss in 69% of patients with isolated posterior instability, with 20% of patients in their cohort noted to have a bone loss of >13.5%. Similarly, Wolfe et al 28 reported on a cohort of 66 military patients and observed 86% of shoulders to have minimal posterior bone loss and 14% to have a subcritical bone loss of >13.5%. These findings align with the results of our study, which suggest that glenoid bone loss is highly prevalent in patients undergoing arthroscopic stabilization for isolated posterior shoulder instability. Furthermore, 23% of patients in our study were found to have glenoid bone loss >13.5%.
Recognizing and correctly characterizing bone loss in the setting of instability is important for determining appropriate surgical management. Glenoid bone loss is a well-accepted risk factor for failure after arthroscopic anterior labral repair, and patients with significant anterior bone loss are often indicated for bony augmentation rather than arthroscopic stabilization.10,13,14 While the importance of bone loss with respect to the management of posterior glenohumeral instability has not been fully elucidated, existing data suggest that greater bone loss may be associated with unfavorable outcomes in posterior instability.2,3,16,28 Arner et al 2 reported a 10-fold higher failure rate among patients with ≥11% posterior bone loss and a 25-fold higher failure rate among patients with ≥15% bone loss. Similarly, Hines et al 16 found that military patients with >13.5% bone loss were less likely to return to active-duty service postoperatively than patients with minimal bone loss, albeit without any significant differences in outcome scores appreciated between the 2 groups. Two studies by Bradley et al6,7 have identified smaller glenoid bone width as a risk factor for failure after posterior labral repair.
Although no consensus guidelines exist for the use of posterior glenoid augmentation procedures, several bone block procedures have been described for use in patients with clinically significant posterior bone loss. Dickens et al 12 advocate for the use of posterior glenoid reconstruction in patients with bone loss of >20% or >10% in the setting of glenoid retroversion, failed primary posterior labral repair, or incompetent or irreparable posterior capsular-labral tissue. While outcome studies after posterior bone augmentation are limited, Gilat et al 15 found that distal tibial allograft augmentation resulted in good outcomes and a reasonable complication rate in a series of 10 patients. However, a 2022 systematic review by Cognetti et al 11 concluded that posterior bone block augmentation for recurrent posterior shoulder instability does not reliably yield substantial improvements in patient-reported outcomes. Further research is necessary to fully understand the role of posterior bone block procedures in patients with clinically significant bone loss. However, the increasing prevalence of these techniques in combination with the high prevalence of posterior bone loss observed in our cohort suggests that the degree of bone loss should be carefully assessed and taken into consideration when evaluating and treating patients with isolated posterior instability.
We also sought to identify risk factors associated with increased posterior glenoid bone loss. In our cohort, patients with dominant arm involvement were found to be at greater risk for increased posterior bone loss as well as bone loss >13.5%. This finding is intuitive given that posterior instability often results from a wear-and-tear type cause and suggests that surgeons should maintain a high index of suspicion for clinically significant bone loss when evaluating patients with dominant arm involvement. 23 Athletic involvement was also identified as a risk factor for subcritical bone loss. Existing data indicate that active populations sustain a higher incidence of posterior instability, with increased rates noted in military patients and high shoulder-demand athletes.21,25,27 Furthermore, participation in contact sports has been associated with the presence of bone loss in anterior instability. 19 Our findings suggest that athletes may not only be at greater risk for posterior instability but may also be more challenging to treat because of subcritical concomitant bone loss. Although female patients tended to have greater mean bone loss and higher rates of bone loss >13.5%, female sex was not identified by multivariate regression as a risk factor for greater bone loss or bone loss >13.5%. Interestingly, while glenoid retroversion is a known risk factor for posterior instability, 20 we did not observe any significant correlation between the degree of retroversion and measured bone loss. This conflicts with the findings of Bedrin et al 3 who noted increased bone loss in patients with >10 degrees of retroversion, albeit in a sample size of 13 patients. However, it is plausible that the presence of greater retroversion may predispose patients to posterior instability at a smaller degree of bone loss. We also did not find any correlation between the time to surgery and the amount of bone loss. Prolonged time from symptom onset to surgery has been shown to increase the risk of bone loss in anterior instability and as such, many surgeons now favor timely operative stabilization.1,4,22-24,26 However, anterior instability and posterior instability are inherently different pathologies with posterior instability more often resulting from chronic, repetitive microtrauma rather than discrete instability events. 21 It is possible that because these patients are less likely to subluxate or dislocate than patients with isolated anterior instability, greater time from symptom onset to definitive management may not have a meaningful impact on bone loss in isolated posterior instability. Last, no difference was found in bone loss between patients who required ≤2 anchors for labral repair and those who required >2 anchors, suggesting that larger posterior labral tears are not necessarily associated with a greater degree of bone loss. In total, these risk factors provide surgeons with a construct to help identify patients presenting with posterior instability who may be at risk for greater bone loss.
Limitations
This study was not without its limitations. The retrospective design of this study represents a source of inherent bias. Measurements obtained from preoperative MRAs using the perfect circle technique were utilized to determine posterior glenoid bone loss. While any discrepancies were reviewed by a third surgeon, a certain degree of error is unavoidable in any measurement.13-16,25 With regard to the nature of our database collection, specifics regarding the mechanism of injury, such as the number of instability events, or details regarding the type of sports participation were not available for analysis. Additionally, Beighton scores were not available for included patients. Last, this study included only patients who underwent arthroscopic stabilization procedures and therefore did not include those who were managed conservatively or patients who required bony augmentation procedures.
Conclusion
The findings of this study are in alignment with existing data suggesting that posterior glenoid bone loss is highly prevalent in patients undergoing primary arthroscopic stabilization for posterior-type shoulder instability. Our results suggest that patients with dominant arm involvement are at risk for greater posterior glenoid bone loss. Furthermore, athlete status and dominant arm involvement were identified as independent risk factors for bone loss >13.5%. Ultimately, understanding the prevalence of, and risk factors for, glenoid bone loss can help guide surgeons when evaluating and treating patients with posterior-type glenohumeral instability.
Footnotes
Final revision submitted April 7, 2023; accepted April 27, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.H.R. has received education payments from CDC Medical and Zimmer Biomet; consulting fees from DePuy and Zimmer Biomet; and hospitality payments from Stryker. N.P. has received consulting fees from Mitek. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Carson-Carthage (No. 2022-06).