
Abstract
Background:
There is concern for maintaining the integrity of the reflected head of the rectus femoris during arthroscopic hip joint access. Because of the proximity to the indirect head of the rectus femoris (IHRF), capsulotomy technique and capsular closure during routine hip arthroscopy may play a role in postoperative tendinitis.
Purpose:
To quantify the extent of injury sustained to the IHRF during interportal versus periportal capsulotomy for routine arthroscopic hip joint access.
Study Design:
Controlled laboratory study.
Methods:
A cadaveric study was conducted using 20 fresh-frozen cadaveric hips, in which hip joint access through a periportal capsulotomy (n = 10) or interportal capsulotomy (n = 10) was performed. Capsular closure followed by a layered dissection to the capsuloligamentous complex of the hip joint was then performed to localize the IHRF. Suture proximity to the tendon, tendon disruption, and the IHRF footprint was documented to the nearest 0.01 mm using digital calipers. Statistical analysis was performed using unpaired Student t tests.
Results:
The mean capsulotomy length for the interportal specimens was 19.27 ± 3.25 mm, and the mean medial and lateral capsulotomy length for the periportal specimens was 4.47 ± 1.60 and 4.26 ± 0.89 mm, respectively. There was violation of the tendon in 3 of 10 interportal specimens and 4 of 10 periportal specimens. There was no significant difference in the closest suture measured to the IHRF for specimens with versus without tendon violation, for either interportal or periportal capsulotomy.
Conclusion:
We found comparable outcomes with regard to violation of the IHRF between interportal and periportal capsulotomy, with no significant difference in suture proximity to the IHRF in specimens with or without tendon violation. There remains no consensus on the ideal method by which to avoid iatrogenic damage to the IHRF.
Clinical Relevance:
Our findings provide insight that may lead to future advances in surgical care, such that protection of the tendon during routine hip arthroscopy may allow for improved postoperative rehabilitation and strength.
The interportal capsulotomy is the most commonly used approach for routine hip arthroscopy; however, periportal and T-capsulotomy are alternative approaches used for hip access during arthroscopic surgery. The interportal approach includes the anterolateral (ALP) and anterior portals, which are connected internally through a capsulotomy under arthroscopic visualization. The iliofemoral ligament is transected parallel to the acetabular rim, allowing for adequate access to the peripheral compartments. 4 Although technically challenging, some surgeons recommend that closure of the capsule be performed to maintain postoperative stability of the hip joint. 8 The periportal capsulotomy approach involves smaller, noninterconnecting capsular entry intended to minimize morbidity to the capsuloligamentous stabilizers. The periportal technique has been described to allow for sufficient and safe access to the peripheral compartments of the hip without necessitating capsular closure.4,7-8 Historically, there has been concern over compromised visualization of the femoral head and neck, thus risking incomplete cam deformity resection. However, recent literature has reported significant improvements in clinical outcomes after periportal capsulotomy for hip joint access for treatment of femoroacetabular impingement. 4 McGovern et al 7 noted similar patient-reported outcomes at 2-year follow-up between algorithmically selected periportal or interportal capsulotomy with closure.
Both the interportal and periportal arthroscopic approaches to the hip allow access to the joint through violation of the anterosuperior capsuloligamentous complex, which primarily comprises the iliofemoral ligament but also contains the indirect (reflected) head of the rectus femoris (IHRF) tendon, located at the anterior superior acetabulum in proximity to the labrum. The indirect head arises from the superior acetabular ridge and adjacent joint capsule. 10 The tendon footprint is firmly attached along the lateral wall of the ilium and becomes thinner and wider as it travels posteriorly from its acetabular origin. The tendon becomes free-lying over the acetabular bone more anteriorly and distally toward its muscular attachment. 2 Arguments for maintaining the integrity of the IHRF during arthroscopic hip joint access include availability of the tendon as a local autograft for labral reconstruction and reduction in postoperative tendinitis. 1 A study by Atzmon et al 2 evaluated the IHRF in 26 cadavers and found the tendon to be in an ideal location and source for graft harvest for labral reconstructive surgery. A cadaveric study 11 identified relevant cadaveric anatomy in relation to the interportal capsulotomy including the IHRF, iliocapsularis, and gluteus minimus; however, this study did not perform arthroscopy before dissection, and these relationships were not evaluated with respect to a capsulotomy during the surgical approach.
The primary objective of this study was to quantify the extent of injury sustained to the IHRF during interportal versus periportal capsulotomy for routine arthroscopic hip joint access. We secondarily evaluated accessibility for labral repair and performed capsular closure to evaluate proximity to the IHRF between the portal sites. Determining the extent of injury may offer insight to potentially unrecognized iatrogenic damage during routine surgical practice and offer opportunity to refine current surgical practices.
Methods
Specimen Preparation
Twenty fresh-frozen cadaveric hip specimens consisting of the hemipelvis and femur were obtained and thawed at room temperature for 24 hours. Cadaveric specimens were randomly allocated to 1 of 2 groups, periportal versus interportal capsulotomy, by selection of an assignment card from a shuffled deck with an equal number of cards for each group. This resulted in 10 hips per group. As this was a cadaveric investigation, ethical approval was not required by our institution.
Arthroscopic Procedure
The specimen was mounted on a traction table in the supine-equivalent position. Two large drill bits were advanced through the pelvis superior to the acetabular insertion of the IHRF and locked into the traction device. Care was taken not to infiltrate the acetabulum or surrounding bony acetabular wall and hip capsule. A transcondylar drill hole was placed through the distal femur, and a braided rope was used to pull traction by weights hung from a pulley (Figure 1A).

(A) Specimens were mounted on a traction table in the supine equivalent position. A transcondylar drill hole was placed through the distal femur, and a braided rope was used to pull traction by weights hung from a pulley. (B) Image from the midanterior portal of a specimen.
A single board-certified, fellowship-trained sports medicine orthopaedic surgeon with primary practice in hip arthroscopy (B.D.G.) performed the arthroscopic portion of the procedures for all included specimens. Two arthroscopic portals, the ALP and midanterior (MAP), were utilized for all hips (Figure 1B). For the ALP, an 18-gauge needle was inserted superior and medial to the anterior medial tip of the greater trochanter. The MAP was created 6 to 7 cm distal and anterior to the ALP, just lateral to the vertical line from the anterior superior iliac spine. A transverse interportal capsulotomy between the ALP and MAP was performed for 10 of the cadaveric specimens using a beaver blade. For the remaining 10 cadaveric specimens, a beaver blade was used to enlarge the capsulotomies without connection between the 2 portals according to surgeon preference. A 70-degree arthroscope was used to perform a thorough diagnostic evaluation of each hip (Figure 1). Labral repair was attempted in all cadaveric specimens (Figure 2A) utilizing 3.0-mm suture anchors (BioComposite Knotless Hip SutureTak; Arthrex). Sequential anchors were placed at the chondrolabral junction through drill guides. Capsular repair was performed in all specimens, both periportal and interportal, with No. 2 FiberWire (Arthrex) sutures using CapsuleClose Scorpion (Arthrex) (Figure 2B). Three sequential arthroscopic sliding knots followed by half-hitches on alternating posts were used to secure the knots in the interportal capsulotomy specimens (Figure 2C). A single arthroscopic knot through each capsulotomy site in similar fashion was utilized for the periportal specimens.
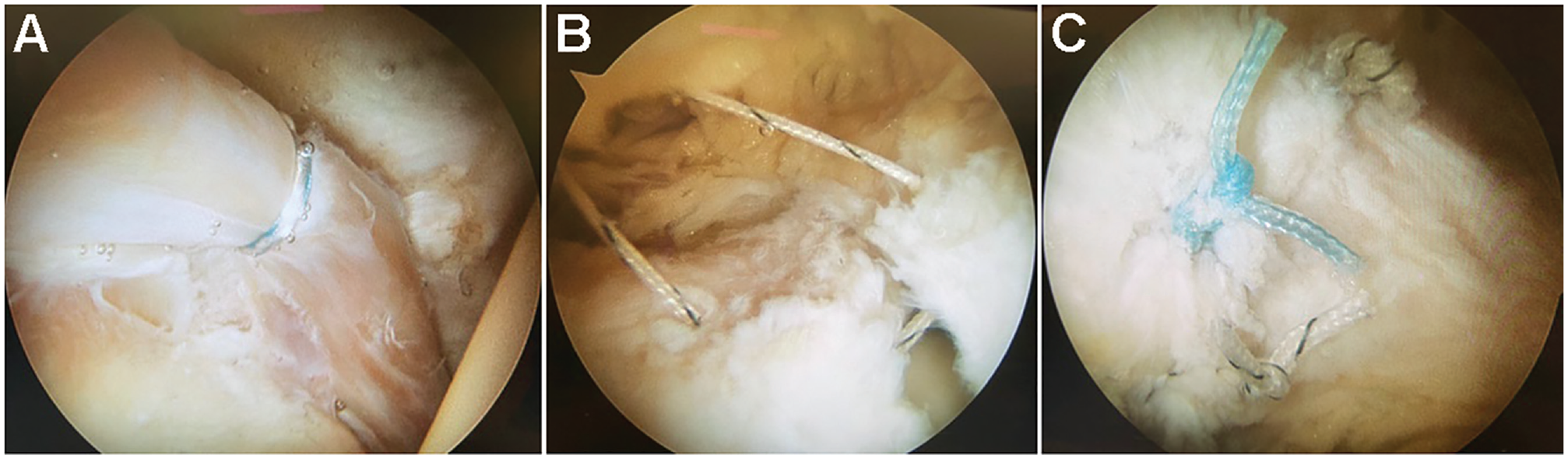
(A) Labral repair was attempted in all specimens. (B) Capsular repair was performed in all specimens. (C) Three sequential arthroscopic sliding knots followed by half-hitches on alternating posts were used to secure the knots in the interportal capsulotomy specimens.
Anatomic Dissection
After arthroscopy, the specimens were unmounted and dissected in a layered fashion. A standard anterior approach (Smith-Peterson) was used to isolate and assess the IHRF. A 10-cm longitudinal incision was made from the anterior superior iliac spine toward the lateral aspect of the patella. The incision was curved slightly posterior along the iliac crest. Dissection was carried through skin and subcutaneous tissue to the level of the fascia overlying the sartorius and tensor fascia lata. The fascia was incised in line with the incision just medial to the tensor fascia lata. The direct head of the rectus femoris originating at the anterior inferior iliac spine, and the reflected head at the superior lip of the acetabulum and the anterior capsule of the hip joint were then visualized (Figure 3A). A marking pen was then utilized to map out the footprint of the IHRF (Figure 3B).

(A) The direct head of the rectus femoris originating at the anterior inferior iliac spine (black asterisk), the reflected head at the superior lip of the acetabulum (white asterisk) and the anterior capsule of a right periportal hip joint are visualized. (B) A marking pen was used to map out the footprint of the indirect head of the rectus femoris on a right hip.
Cadaveric Measurements
After dissection, an electronic digital caliper was utilized to measure tendon length, width, and thickness to the nearest 0.01 mm. Tendon width and thickness was measured at the medial-most and lateral-most points, as well as a point marked approximately midway between the 2 extremes. All measurements were performed 3 times. Additionally, capsulotomy length and proximity to the tendon was documented. Any violation of the IHRF tendon was also documented. Violation of the IHRF was defined as any capsulotomy incision extending into the IHRF and/or suture infiltration along the length of the tendon from the capsular closure. All measurements were performed by 2 independent investigators (U.J.P. and D.E.A.), with triplicate measurements performed in a sequential fashion. The mean of the 6 measurements by the 2 investigators was recorded.
Statistical Analysis
Data from all 10 hips from each group were pooled. The mean and standard deviation were determined for all continuous variables. The paired Student t test was used to compare repeated measures for each tendon measurement between the 2 independent investigators (U.J.P., D.E.A.). Interobserver reliability and agreement was calculated between measurements of the 2 independent investigators using the intraclass correlation coefficient (ICC) with a 2-way, random-effects model. Statistical analyses between interportal and periportal groups were performed using unpaired Student t tests for continuous variables and chi-square test for proportions of categorical values. P <.05 was considered statistically significant. A Fisher exact test was used to test the contingency of capsular violation between interportal and periportal groups.
Results
Specimen Characteristics
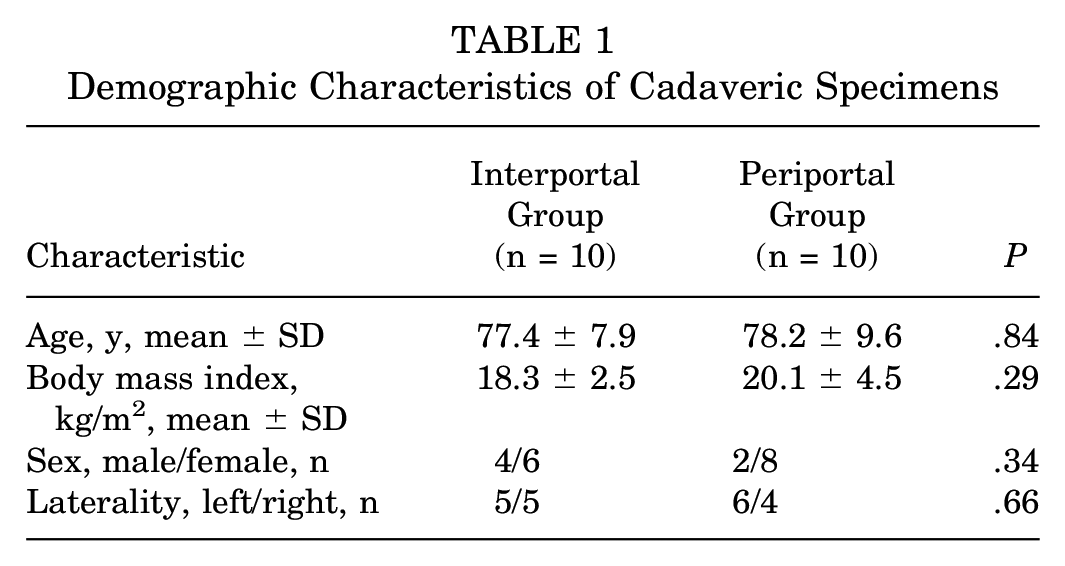
The cadaveric specimens consisted of 4 men and 6 women in the interportal capsulotomy group and 2 men and 8 women in the periportal capsulotomy groups (Table 1). The mean age was 77.4 ± 7.9 years for the interportal specimens and 78.2 ± 9.6 years for the periportal specimens (P = .84). In total, there were 5 left and 5 right hemipelves in the interportal group and 6 left and 4 right hemipelves in the periportal group.
Demographic Characteristics of Cadaveric Specimens
IHRF Tendon Measurements
There was moderate to excellent interrater agreement of the cadaveric measurements (ICC, 0.534-0.931) (Table 2). As we did not anticipate any tendon differences between interportal and periportal cohorts in the tendon itself, the comparison was between the male and female specimens. The mean tendon length was 39.42 ± 6.65 mm for the female specimens and 38.36 ± 6.20 mm for the male specimens (P = .84) (Figure 4A). The mean tendon width was 14.98 ± 2.51 mm medially, 15.31 ± 1.72 mm centrally, and 14.09 ± 2.59 mm laterally in the female specimens and 14.47 ± 2.94 mm medially, 15.03 ± 1.45 mm centrally, and 14.12 ± 2.21 mm laterally in the male specimens. There was no statistically significant difference between the female and male specimens for tendon width medially (P = .67), centrally (P = .69), or laterally (P = .98) (Figure 4B). The mean tendon thickness was 1.88 ± 0.55 mm medially, 1.31 ± 0.49 mm centrally, and 0.74 ± 0.23 mm laterally in the female specimens and 1.43 ± 0.09 mm medially, 1.13 ± 0.20 mm centrally, and 0.87 ± 0.32 mm laterally in the male specimens. There was no statistically significant difference between the female and male specimens for tendon thickness medially (P = .87), centrally (P = .68), or laterally (P = .82) (Figure 4C).
Interrater Agreement of Paired Measurements a

ICC, intraclass correlation coefficient; IP, interportal; PP, periportal.
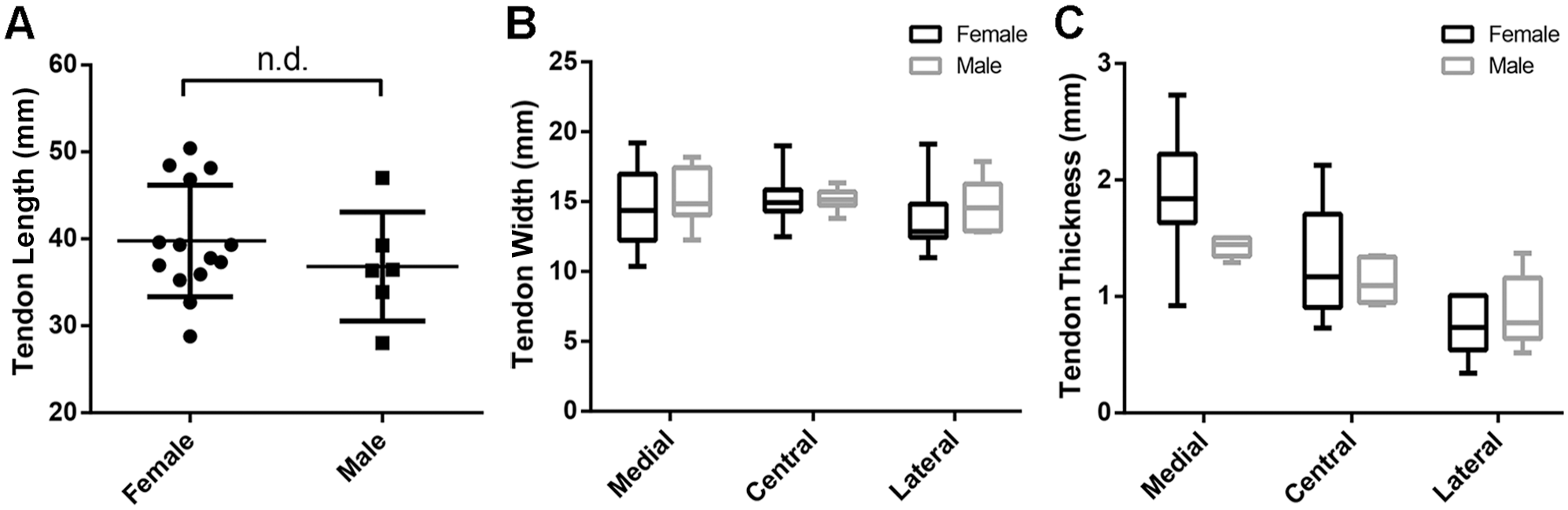
Comparison of indirect head of the rectus femoris tendon (A) length, (B) width, and (C) thickness between male and female specimens. In (A), the center line represents the mean, and the top and bottom lines represent the SD. In (B) and (C), the center line represents the mean, the top and bottom of the box represent the SD, and the whiskers represent the interquartile range. n.d., no significant difference.
Capsulotomy Measurements
The mean interportal capsulotomy length was 19.27 ± 3.25 mm, and the mean ALP and MAP periportal capsulotomy lengths were 4.47 ± 1.60 mm medially and 4.26 ± 0.89 mm laterally (Figure 5A). There were 3 specimens out of 10 in the interportal capsulotomy group and 4 out of 10 specimens in the periportal capsulotomy group with violation of the IHRF (P > .99) (Figure 5B). The closest suture measured to the IHRF for all specimens was 3.10 ± 3.18 mm in the interportal capsulotomy group and 1.97 ± 2.10 mm in the periportal capsulotomy group (P = .37) (Figure 5C).

(A) The interportal (IP) capsulotomy length and periportal (PP) capsulotomy length medially and laterally. (B) There were 3 out of 10 specimens in the IP capsulotomy group and 4 out of 10 specimens in the PP capsulotomy group with violation of the indirect head of the rectus femoris (IHRF) tendon. (C) Comparison of closest suture measured to the IHRF between all specimens of each group. In (A) and (C), the center line represents the mean, and the top and bottom lines represent the SD. n.d., no significant difference.
Discussion
In this study, we primarily investigated violation of the IHRF with routine capsulotomy and closure after interportal and periportal capsulotomies. In both study groups, comparable violation of the IHRF was found with no statistically significant difference in the proximity of suture closest to the IHRF tendon in the periportal cohort as compared with the interportal cohort. Arthroscopy was performed before surgical dissection, which showed infiltration of the capsulotomy and closure sutures in the IHRF tendon in 3 interportal and 4 periportal specimens.
One cause of postoperative pain after hip arthroscopy is iliopsoas tendinitis. Although the iliopsoas tendon has been implicated in hip disorders such as internal snapping hip, instability, psoas impingement, and labral tears, 1 there is a paucity of literature evaluating the incidence of postoperative iliopsoas and rectus femoris tendinitis after hip arthroscopy. Furthermore, there is a void in the literature specifically evaluating tendinitis related to periportal versus interportal capsulotomy surgical techniques. Given that this is a cadaveric study, we were limited in the ability to assess postoperative symptoms, but we did demonstrate violation of the IHRF tendon in 35% of the specimens. We speculate that capsulotomy and closure with nonabsorbable suture after hip arthroscopy may cause local mechanical and inflammatory postoperative IHRF tendinitis or adjacent iliopsoas tendinitis.
A 2021 study published by McGovern et al 7 found that patients who underwent periportal capsulotomy without closure had improved patient-reported outcomes and satisfaction at 2-year follow-up as compared with patients who underwent interportal capsulotomy with closure, although the results were not statistically significant. This study used a clinical algorithm for selection of patients to undergo periportal without closure versus interportal capsulotomy with closure. Of note, the authors reported a larger capsulotomy length for both the cohorts than did our findings. Patients in the periportal group reportedly had capsulotomy length of 10 mm for each portal without closure, and patients in the interportal group had capsulotomy length of 4 cm with 1 to 2 suture repairs of the capsulotomy. In our study, the mean periportal capsulotomy length was 4 mm each, with a single suture repair for closure. The mean interportal capsulotomy length was 20 mm with 3 suture repairs of the capsulotomy. Thus, McGovern et al reported close to double capsulotomy length compared with our study, with approximately half the number of sutures used for closure.
A 2022 study by Nguyen et al 9 reported positive patient-reported outcomes after periportal capsulotomy without closure at 1 year after the procedure. The authors attributed improved patient pain, function, and return to sport to change in the hip capsular morphology including a decreased anteroposterior capsular thickness ratio after surgery. However, in their methodology, they also reported periportal dimensions of 8 mm for the ALP and 10 mm for the MAP. The authors theorized that a thicker anterior capsule could exacerbate posterior hip instability that is associated with femoroacetabular impingement and that periportal technique can result in thinning of the anterior capsule from portal dilation, leading to their findings.
Hassebrock et al 5 showed faster return to play in athletes who underwent complete capsular closure after interportal capsulotomy during routine hip arthroscopy compared with nonclosure of the capsule in high-level athletes. Capsulotomy length was not reported. While they found no cases of instability from nonclosure of the capsulotomy, there have been reports of early failure, iatrogenic instability and dislocation, and conversion to total hip arthroplasty.3,6
Ultimately, there is a lack of consensus on whether capsular closure is necessary after routine hip arthroscopy. Previous literature has discussed complications that can arise from capsular closure as well as from leaving the capsulotomy open. Additionally, there is a lack of consensus on capsulotomy length for periportal versus interportal techniques. This can also affect the outcomes reported in prior literature as poor patient-reported outcomes in larger capsulotomy lengths with closure may be comparable to smaller capsulotomy lengths without closure for interportal cohorts. Additionally, periportal cohorts showing improved outcomes may in fact have comparable outcomes to interportal cohorts with similar capsulotomy lengths without closure.
Limitations
This study is subject to several limitations. First, this was a cadaveric study. Our cadavers were fresh-frozen, which allowed for better overall tissue quality and preservation of tissue planes. This allowed the structures to be more clearly delineated and improved the accuracy of our measurements. However, a potential limitation is that measurements of the tendon were based on gross dissection, and a more accurate measurement could have been made with histologic analysis of tendon origin and insertion. Surgical procedures were performed on unmatched hemipelves given resource availability. Additionally, given the advanced age of the pelvic cohorts, suture anchor fixation in the pelvic specimens was limited with increased pullout of the suture anchors due to poor bone quality. Advanced age of the cadaveric specimens is also a relative limitation, as structures of the hip capsuloligamentous complex may attenuate with increasing age, and labral repair or reconstruction is not commonly performed in the elderly population. Because of the limitations of this cadaveric study, clinical correlation with a population of younger patients undergoing hip arthroscopy is not fully understood. All arthroscopic surgeries were performed by a single surgeon at a single institution, which may have limited the generalizability of the results. However, a standardized surgical procedure may also ensure reproducibility of the findings. All measurements were taken in triplicate in an attempt to reduce the limitations of human error in measurements, and there was no significant variation in measures between readers based on ICC.
Conclusion
We found comparable measurements with regard to violation of the IHRF with interportal versus periportal capsulotomies. There was no difference in suture proximity to the IHRF in cases of tendon violation or in cases where there was no tendon violation. There remains no consensus on the ideal method by which to avoid iatrogenic damage to the IHRF. Further prospective studies evaluating patient outcomes after interportal capsulotomies with and without closure versus periportal capsulotomies without closure may help further our understanding of postoperative complications such as tendinitis.
Footnotes
Final revision submitted April 18, 2023; accepted May 4, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for cadaveric specimens and surgical supplies was provided by a grant from Arthrex. Y.-M.Y. has received consulting fees from Smith & Nephew. B.D.G. has received consulting fees, nonconsulting fees, and royalties from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.